The measurement and correlation analysis of scleral and choroid thickness in branch retinal vein occlusion
Xiao Yu, Yuling Zou, Ziqing Mao, Huimin Fan, Xiaolong Yu, Teng Liu, Zhipeng You

TL;DR
This study uses OCT to measure eye tissue thickness in patients with a type of eye disease and finds significant differences and correlations.
Contribution
The study introduces a correlation analysis between scleral and choroid thickness in BRVO patients using OCT measurements.
Findings
BRVO-affected eyes showed significantly higher CRT than contralateral and control eyes.
SFCT and ST measurements varied significantly between BRVO-affected and control eyes.
A positive correlation was found between SFCT/CRT and temporal ST in BRVO patients.
Abstract
To use Optical Coherence Tomography (OCT) to measure scleral thickness (ST) and subfoveal choroid thickness (SFCT) in patients with Branch Retinal Vein Occlusion (BRVO) and to conduct a correlation analysis. A cross-sectional study was conducted. From May 2022 to December 2022, a total of 34 cases (68 eyes) of untreated unilateral Branch Retinal Vein Occlusion (BRVO) patients were recruited at the Affiliated Eye Hospital of Nanchang University. Among these cases, 31 were temporal branch vein occlusions, 2 were nasal branch occlusions, and 1 was a superior branch occlusion. Additionally, 39 cases (39 eyes) of gender- and age-matched control eyes were included in the study. Anterior Segment Optical Coherence Tomography (AS-OCT) was used to measure ST at 6 mm superior, inferior, nasal, and temporal to the limbus, while Enhanced Depth Imaging Optical Coherence Tomography (EDI-OCT) was used…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
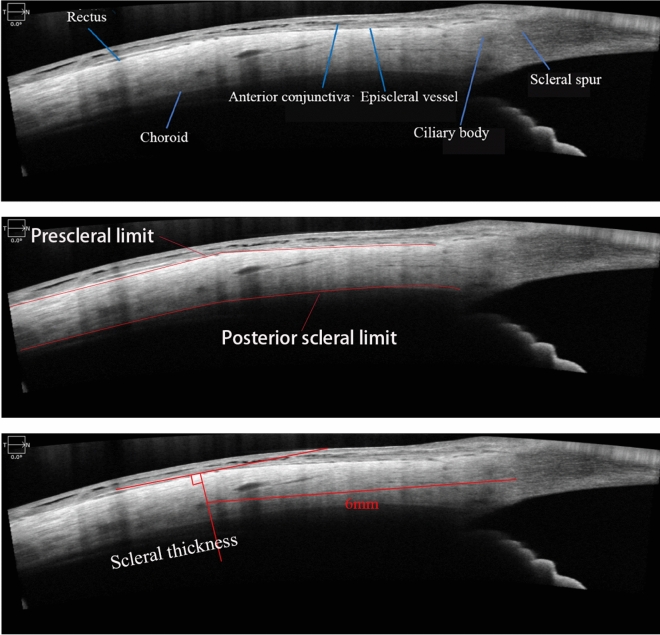 Figure 1
Figure 1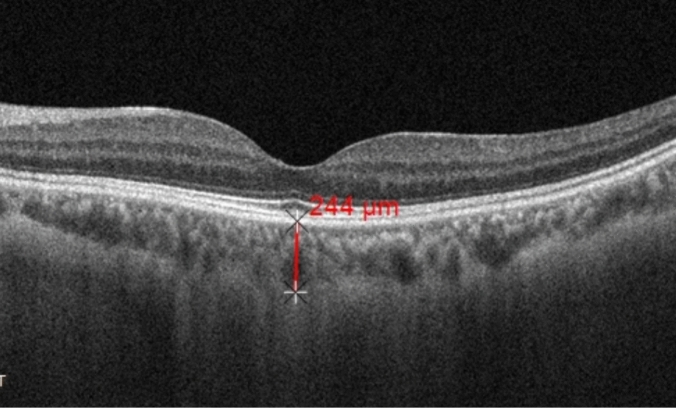 Figure 2
Figure 2- —National Natural Science Foundation of China
- —Key Research and Development Program of Science and Technology Department of Jiangxi Province-Key Projects (Unveiled)
- —cience and Technology Program of Health Commission of Jiangxi Province
- —Key Project of Education Department of Jiangxi Province
- —Key Project of Jiangxi Natural Science Foundation
- —Central Government Guided Local Science and Technology Development Fund
- —Key Project of Science and Technology Innovation of Health Commission of Jiangxi Province
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRetinal Diseases and Treatments · Retinal and Optic Conditions · Retinal Imaging and Analysis
Introduction
Retinal Vein Occlusion (RVO) refers to the blockage of the retinal vein system due to various reasons, leading to a common retinal vascular disease characterized by retinal ischemia and hypoxia. Depending on the degree of retinal vessel involvement, RVO can be further classified into Central Retinal Vein Occlusion (CRVO) and Branch Retinal Vein Occlusion (BRVO)^1^. The global prevalence of BRVO in people aged 30–89 years was 0.64%, making it the most common type of RVO, and it is associated with various factors such as hypertension and atherosclerosis^2^. BRVO often occurs at arteriovenous crossings and is mainly related to changes in hemodynamics, vascular endothelial cell damage, and hypercoagulability, although the exact mechanism of its occurrence is not clear^3^. Recent studies have shown that the pathology of RVO involves not only the retina but also the choroid. Aribas et al. found that in RVO, the total number of choroidal vessels and the capillary blood flow density in the choroid are reduced, while the choroidal large vessel layer shows vascular dilation^4^. Previous studies have indicated that compared to the normal control group, Subfoveal Choroid Thickness (SFCT) increases in RVO eyes, and SFCT decreases after intravitreal anti-vascular endothelial growth factor injection therapy, suggesting that the increase in SFCT is associated with an increase in vascular endothelial growth factor in the choroid, changes in vascular permeability, and fluid leakage^5–7^. Meryem et al. demonstrated that in BRVO patients, SFCT increases, the area of intercellular stroma and total choroidal area increase, while the total choroidal blood flow does not change, suggesting that the increase in SFCT in BRVO patients is due to extracellular fluid flowing from the retina into the choroid, causing choroidal interstitial edema, rather than changes in vascular quantity and density^8^. Similarly, previous studies have suggested that changes in the choroid in RVO may be due to alterations in choroidal hemodynamics, rather than changes in vascular quantity^4,9^. Recent research has indicated that RVO shares similar pathogenic mechanisms with pachychoroid disease^10^. Venkatesh et al. proposed that an increase in scleral thickness or hardness may be a possible pathogenic mechanism of pachychoroid disease^11^. Whether Scleral Thickness (ST) also plays a significant role in the occurrence of RVO is a question that has been rarely investigated. Therefore, we utilized Anterior Segment Optical Coherence Tomography (AS-OCT) to study changes in ST and SFCT in BRVO and conducted correlation analysis, aiming to provide new insights into the etiology and treatment of BRVO in clinical practice.
Research methods
General information
This was a cross-sectional study. A total of 34 untreated unilateral BRVO patients (68 eyes) who visited our hospital from May 2022 to December 2022 were selected. Additionally, 39 normal control subjects with gender and age matched to the unilateral BRVO eyes were included in the study. Patients with a history of intraocular surgery, concomitant glaucoma, uveitis, idiopathic polypoidal choroidal vasculopathy, age-related macular degeneration, central serous chorioretinopathy, myopia, neurodegenerative diseases, prior intravitreal injections, laser treatment, hypertension which was the absence of a previous history of hypertension and a blood pressure measurement at presentation that did not meet the diagnostic criteria for hypertension guidelines, diabetes, connective tissue diseases, and those with unclear imaging data of systemic diseases were excluded. All patients enrolled in this study underwent AS-OCT, Enhanced Depth Imaging Optical Coherence Tomography (EDI-OCT), Best Corrected Visual Acuity (BCVA) assessment, fundus fluorescein angiography, axial length measurement, intraocular pressure measurement, slit lamp examination, and dilated fundus examination between 9 and 11 am. The study was conducted in accordance with the Helsinki Declaration and approved by the Affiliated Eye Hospital of Nanchang University's ethics committee (YLP20211210). All patients provided informed consent and signed the informed consent form.
Imaging examinations
The patients underwent AS-OCT and EDI-OCT using ZEISS CIRRUS HD^5000^. AS-OCT measurements were taken 6 mm posterior to the limbus in the superior, inferior, nasal, and temporal directions to assess ST. According to Suzuki et al., the four straight muscles are adjacent to the sclera and appear as low-reflectance lines^12^. The scleral anterior border was determined by the boundary between the low-reflectance straight muscles (superior rectus, inferior rectus, medial rectus, lateral rectus) and the high-reflectance sclera, while the scleral posterior border was determined by the signal from the choroid (Fig. 1). The ST measurements were conducted following the method described by Read et al.^13–15^. The ST in the four directions represented by the vertical distance between the anterior and posterior borders of the sclera 6 mm posterior to the limbus. EDI-OCT was performed between 9 and 11 am to measure SFCT. The SFCT was defined as the vertical distance from Bruch's membrane to the inner surface of the sclera in the central foveal region, represented by the vertical distance between the high-reflectance line below the retinal pigment epithelium and the low-reflectance line on the inner surface of the sclera (Fig. 2). ST and SFCT measurements were taken three times by the same ophthalmologist, and the average value was recorded and analyzed. Axial length measurements were conducted for all patients using the IOL Master from ZEISS MASTER 5.5.Figure 1. The measurement of scleral thickness.Figure 2. The measurement of subfoveal choroid thickness.
Statistical methods
Statistical analysis was performed using SPSS 24.0 software. For continuous data, the Shapiro–Wilk test was used to assess normality, and Levene's test was used to test for homogeneity of variance. As the data followed a normal distribution and exhibited homogeneity of variance, independent samples t-test was used for comparisons between two groups, and one-way analysis of variance (ANOVA) was used for comparisons among multiple groups. Pearson's correlation analysis was conducted to assess correlation analysis. Continuous data are presented as mean ± standard deviation (mean ± SD). For categorical data comparisons, the chi-square test or Fisher's exact test was used. A significance level of P < 0.05 was considered statistically significant.
Results
General information
The BRVO group consisted of 34 patients with 34 affected eyes, including 18 females and 16 males. There were 20 cases in the left eye and 14 cases in the right eye, with 31 patients having temporal branch vein occlusion, 2 patients with nasal branch occlusion, and 1 patient with superior branch occlusion. The average age was (57.38 ± 12.82) years, with a disease duration of (4.67 ± 1.87) months. The axial length of the affected eyes was (22.92 ± 0.30) mm, ranging from 22.43 to 23.53 mm, while the axial length of the contralateral eyes was (22.89 ± 0.32) mm, ranging from 22.26 to 23.48 mm. The difference in axial length between BRVO-affected eyes and contralateral eyes was not statistically significant (t = 0.37, P = 0.71).
The control group comprised 39 participants with 39 eyes, including 23 females and 16 males, with 20 left eyes and 19 right eyes. The average age was (57.90 ± 7.83) years, and the axial length was (22.90 ± 0.28) mm, ranging from 22.31 to 23.67 mm. There were no statistically significant differences in age and axial length between the BRVO group and the control group (t = − 0.21, 0.34; P = 0.83, 0.74) (Table 1). The differences of SFCT, temporal, nasal, superior and inferior ST among the three groups were statistically significant (F = 144.34, 18.03, 57.40, 70.00, 62.55, all P values were less than 0.001). Multiple comparisons indicate that BRVO-affected eyes showed statistically significant increases in SFCT, temporal, nasal, superior and inferior ST compared to contralateral eyes and the control group eyes (P < 0.05). The CRT of BRVO-affected eyes was significantly higher than that of the contralateral eyes and the control eyes (P < 0.001). The difference between the CRT of the contralateral and control eyes was not statistically significant (P = 0.421).Table 1. Comparison of general information among the three groups.CategoryBRVO-affectedContralateral eyesControl eyesP_1_P_2_P_3_Axial lengths (mm)22.92 ± 0.3022.89 ± 0.3222.90 ± 0.280.710.740.94Age (years)57.38 ± 12.8257.38 ± 12.8257.90 ± 7.83–0.83–Sex Female181823–0.60– Male161616–0.60–BRVO branch retina vein occlusion, P1 statistical values for comparisons between BRVO-affected and contralateral eyes, P2 statistical values for comparisons between BRVO-affected and control eyes, P3 statistical values for comparisons between contralateral eyes and control eyes.P < 0.05 was statistically significant.
Comparison between BRVO-affected eyes and contralateral eyes
The Best Corrected Visual Acuity (BCVA) of BRVO-affected eyes was (0.92 ± 0.41) LogMAR, while that of contralateral eyes was (0.08 ± 0.73) LogMAR. BRVO-affected eyes showed statistically significant increases in SFCT, temporal, nasal, superior and inferior ST compared to contralateral eyes (P < 0.05) (Table 2).Table 2. Comparison between BRVO-affected eyes, contralateral eyes and control eyes.CategoryBRVO-affected eyesContralateral eyesControl eyest_1_t_2_t_3_P1P2P3SFCT (μm)391.88 ± 38.70246.18 ± 18.13235.41 ± 10.5019.8824.27− 3.15 < 0.001* < 0.0010.002Temporal ST (μm)447.88 ± 50.55388.62 ± 29.76384.67 ± 60.555.894.80− 0.35 < 0.001 < 0.0010.73Nasal ST (μm)466.38 ± 47.24357.82 ± 25.03389.28 ± 51.0011.846.673.27 < 0.001 < 0.0010.002Superior ST (μm)478.44 ± 53.43346.59 ± 28.70389.69 ± 53.2312.687.094.21 < 0.001 < 0.001* < 0.001Inferior ST (μm)455.32 ± 49.08341.47 ± 27.00385.18 ± 46.8211.866.244.79 < 0.001 < 0.001* < 0.001**BRVO* branch retina vein occlusion, SFCT subfoveal choroid thickness, ST scleral thickness.t_1 and P_1: statistical values for comparisons between BRVO-affected and contralateral eyes; t_2_ and P_2_: statistical values for comparisons between BRVO-affected and control eyes;t_3_ and P_3_: Statistical values for comparisons between contralateral eyes and control eyes; P < 0.05 was statistically significant; * indicates P < 0.001.
Comparison between BRVO-affected eyes and the control group
The BCVA of BRVO-affected eyes was (0.92 ± 0.41) LogMAR, while that of the control group was (0.07 ± 0.68) LogMAR. Statistical analysis revealed significant differences in SFCT, temporal ST, nasal ST, superior ST, and inferior ST between the two groups (t = 24.27, 4.80, 6.67, 7.09, 6.24; P < 0.001 for all) (Table 2).
Comparison between the control group and contralateral eyes
The difference in axial length between the control group and contralateral eyes was not statistically significant (t = 0.08, P = 0.94). The difference in temporal ST between the contralateral eyes and the control eyes was not statistically significant (t = − 0.35, P = 0.73).
However, the contralateral group showed statistically significant increases in SFCT, nasal, superior and inferior ST compared to control eyes (t = − 3.153, 3.27, 4.21, 4.79, P = 0.002, 0.002, < 0.001, < 0.001) (Table 2).
Comparison between major BRVO and macular BRVO
Patients with BRVO were further divided into more pronounced venous congestion group (major BRVO) and less congestion group (macular BRVO) according to whether the occlusion site involved the macular blood vessels. The comparison of nasal, superior, and inferior ST between the major BRVO group and macular BRVO group did not show any statistically significant differences (t = 0.92, 0.81, 1.05, P = 0.37, 0.43, 0.30). However, the thickness of SFCT and temporal ST in major BRVO group is higher than the macular BRVO group and the difference was statistically significant (t = 6.39, 7.17, P < 0.001 for all) (Table 3).Table 3. Comparison between major BRVO and macular BRVO.CategoryMajor BRVOMacular BRVOtPAge (years)57.50 ± 10.5457.25 ± 15.350.060.96Axial lengths (mm)22.90 ± 0.3122.94 ± 0.31-0.330.74SFCT (μm)536.17 ± 27.44481.19 ± 22.046.39 < 0.001Tempora ST (μm)484.78 ± 35.09406.38 ± 25.997.17 < 0.001Nasal ST (μm)473.39 ± 47.70458.50 ± 46.970.920.37Superior ST (μm)485.44 ± 62.00470.56 ± 42.430.810.43Inferior ST (μm)463.67 ± 43.48445.94 ± 54.581.050.30BRVO branch retina vein occlusion, SFCT subfoveal choroid thickness, ST scleral thickness.P < 0.05 was statistically significant; * indicates P < 0.001.
Comparison between BRVO-affected eyes with and without macular edema
Among the BRVO-affected eyes, 20 eyes had macular edema (ME group) and 14 eyes did not have ME (non-ME group). The axial length of the ME group was (22.834 ± 0.25) mm, while that of the non-ME group was (23.045 ± 0.34) mm. The difference was not statistically significant (t = − 1.96, P = 0.06). The comparison of SFCT and temporal, nasal, superior, and inferior ST between the ME group and non-ME group did not show any statistically significant differences (t = − 1.10, 0.45, -1.30, -0.30, 1.00; P = 0.28, 0.66, 0.21, 0.77, 0.33).
Correlation analysis between SFCT/CRT and ST
Pearson correlation analysis revealed that in BRVO patients, there was a significant positive correlation between SFCT and temporal ST (r = 0.288, P = 0.049). However, there was no correlation between SFCT and nasal ST, superior ST, and inferior ST (r = 0.076, 0.126, 0.183; P = 0.335, 0.238, 0.150) (Table 4).Table 4. Correlation analysis between SFCT and ST in BRVO eyes.SFCTTemporal STNasal STSuperior STInferior STr0.2880.0760.1260.183P0.0490.3350.2380.150BRVO branch retina vein occlusion, SFCT subfoveal choroid thickness, ST scleral thickness.P < 0.05 was statistically significant.
Pearson correlation analysis revealed that in BRVO patients, there was a significant positive correlation between CRT and temporal ST (r = 0.355, P = 0.04). There was no correlation between CRT and nasal ST, superior ST, and inferior ST (r = − 0.081, − 0.102, 0.038; P = 0.650, 0.567, 0.832) (Table 5).Table 5. Correlation analysis between CRT and ST in BRVO eyes.CRTTemporal STNasal STSuperior STInferior STr0.355− 0.081− 0.1020.038P0.040.6500.5670.832BRVO branch retina vein occlusion, CRT central retinal thickness, ST scleral thickness.P < 0.05 was statistically significant.
Discussion
Retinal vein occlusion (RVO) is the second most common retinal vascular disease in the world, following diabetic retinopathy^16^. RVO results in retinal hemorrhage, exudation, and macular edema due to retinal ischemia and hypoxia, leading to vision loss and increased societal burden. Risk factors for RVO include atherosclerosis, advanced age, hypertension, smoking, diabetes, retinal vein blood stasis, and changes in blood flow velocity^2^. However, some RVO patients do not exhibit the previously reported risk factors, indicating the involvement of other factors in RVO development.
Our study showed that the SFCT of eyes in the BRVO group was significantly increased compared to contralateral eyes and normal control group patients, with statistical significance. This finding is consistent with previous studies indicating increased SFCT in BRVO patients^17,18^. Research suggests that the pathogenic mechanisms of RVO and thick choroid diseases are similar, in RVO patients, central serous chorioretinopathy, idiopathic polypoidal choroidal vasculopathy, and other thick choroid diseases are more common, suggesting that eyes with choroidal thickening characteristics may have slowed blood flow, making them more susceptible to RVO^10^. However, it seems unlikely that the retrograde choroidal blood flow associated with localized BRVO could affect the sclera to the extent of causing overall thickening. If choroidal thickening were a cause of RVO, anti-VEGF treatment would not be expected to reduce the choroid thickness. Interestingly, studies have shown that the SFCT of eyes with primary RVO-ME is thickened. Anti-VEGF therapy can effectively reduce SFCT, improve ME, and improve BCVA^19^, suggesting that its thickening in BRVO is a consequence of increased intraocular VEGF and nitric oxide levels. Even so, the exact mechanism for choroidal thickening in BRVO are still unclear.
The choroid accounts for approximately 85% of ocular blood volume, providing oxygen, nutrients, and regulating temperature primarily to the outer retina^20^. The choroid is the most vascularized and metabolically active region in the eye, making it susceptible to influences from retinal vascular occlusions. Adequate intraocular blood circulation necessitates vessel penetration into the eye wall. Recent insights into choroidal thickness and its spectrum of diseases highlight the interplay and dependency between the three layers of the eye wall and intraocular vessels. Research has suggested that diseases involving choroidal thickness are primarily caused by choroidal vein stasis and vortex vein remodeling leading to retinal pathology, with the venous reflux within the eye likely involving the sclera^21^. Our study also demonstrates a statistically significant increase in temporal, nasal, superior, and inferior ST in BRVO-affected eyes compared to contralateral eyes and normal control group patients. Moreover, our study showed that the thickness in SFCT and temporal ST in the more pronounced venous congestion group (major BRVO) is higher than the less congestion group. This may be attributed to choroidal blood flow reflux through vortex veins, which enter the superior and inferior ophthalmic veins through the sclera. The increased thickness or hardness of the sclera may compress the vortex veins, leading to impaired choroidal blood reflux, venous stasis, ischemia, hypoxia, increased vascular endothelial growth factor, changes in vascular permeability, interstitial edema, and increased SFCT. Our speculation is consistent with previous research findings. Taiji et al. studied the SFCT in patients with RVO before and after intravitreal injection of aflibercept, showing a decrease in SFCT after the treatment^22^. Kohji et al. followed RVO patients for 12 months after intravitreal injection of anti-vascular endothelial growth factor therapy and found no statistically significant changes in retinal superficial and deep vascular densities or in the area of the avascular zone in the fovea, but observed a decrease in choroidal thickness^8^. Chung et al. demonstrated a significant increase in choroidal volume in eyes affected by BRVO compared to contralateral eyes, which decreased after intravitreal injection of anti-vascular endothelial growth factor therapy. They also suggested that the increased vascular permeability in BRVO patients is the reason for the thickening of SFCT, which decreases after treatment, leading to a reduction in vascular permeability^23^. These studies indicate that an increase in SFCT in BRVO patients is not related to changes in vascular density but may be associated with alterations in vascular permeability. Our correlation analysis in this study also revealed a positive correlation between SFCT/CRT and temporal ST in BRVO patients (r = 0.288, 0.355, P = 0.049, 0.04). There was no correlation between SFCT and nasal, superior, and inferior ST (P > 0.05). This may be attributed to the majority of cases in our study being patients with temporal branch vein occlusion, indicating a correlation between the increase in SFCT/CRT and the location of vascular obstruction in BRVO. Additionally, our study found that the presence of macular edema (ME) in BRVO did not have a significant impact on SFCT, as well as temporal, nasal, superior, and inferior ST. What’s more, our study also showed a general increase in scleral thickness and an increase in SFCT in the contralateral eyes of BRVO patients, which further confirmed the presence of scleral and choroidal thickening features in BRVO patients.
To the best of our knowledge, this is the first study investigating changes in ST in BRVO. Our study indicates an increase in SFCT, temporal ST, nasal ST, superior ST, and inferior ST in eyes affected by BRVO. However, our study also has some limitations: 1. It is a cross-sectional study, lacking longitudinal comparisons before and after intravitreal anti-vascular endothelial growth factor therapy and laser treatment in BRVO patients; 2. We did not utilize optical coherence tomography angiography to quantitatively analyze choroidal vasculature to further validate our speculations.3. The sample size was small, and due to the different pathogenic mechanisms of BRVO and CRVO^24^, our study only included BRVO patients, lacking research on CRVO patients.4. This study lacks research on the optic disc morphology and blood flow in patients with BRVO. It is currently unclear whether small optic discs are also associated with thick sclera and play a significant role in the occurrence and development of BRVO. In CRVO, a small optic disc is a risk factor, but Yang Rundong et al. measured optic disc morphological parameters, including cup-to-disc ratio, optic disc area, and rim area, in patients with unilateral RVO, contralateral eyes, and healthy control groups, and found no significant differences^25^. Zhu Shaojin et al. found a decrease in blood flow density in the optic disc region of the affected eye in patients with unilateral RVO^26^; 5. All measurements were done manually, and measurement errors were unavoidable. Taking the average value of ST at different distances from the corneal edge may reduce some measurement errors. The next step in our exploration will involve a large-sample prospective comparative study using optical coherence tomography angiography to investigate the effects of intravitreal anti-vascular endothelial growth factor therapy in patients with RVO.
Conclusion
In patients with BRVO, both SFCT and ST are increased, and there is a significant correlation between SFCT and the location of vascular obstruction in ST.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nicholson L Talks SJ Amoaku W Retinal vein occlusion (RVO) guideline: executive summary [J]Eye (Lond)20221110.1038/s 41433-022-02007-4PMC 904615535301458 · doi ↗ · pubmed ↗
- 2Song P Xu Y Zha M Global epidemiology of retinal vein occlusion: a systematic review and meta-analysis of prevalence, incidence, and risk factors [J]J. Glob. Health 2019911042710.7189/jogh.09.010427 PMC 651350831131101 · doi ↗ · pubmed ↗
- 3Rehak J Rehak M Branch retinal vein occlusion: pathogenesis, visual prognosis, and treatment modalities [J]Curr. Eye Res.200833211113110.1080/0271368070185190218293182 PMC 2430176 · doi ↗ · pubmed ↗
- 4Aribas YK Hondur AM Tezel TH Choroidal vascularity index and choriocapillary changes in retinal vein occlusions [J]Graefes Arch. Clin. Exp. Ophthalmol.2020258112389239710.1007/s 00417-020-04886-332860575 · doi ↗ · pubmed ↗
- 5Chen L Yuan M Sun L Choroidal thickening in retinal vein occlusion patients with serous retinal detachment [J]Graefes Arch. Clin. Exp. Ophthalmol.2021259488388910.1007/s 00417-020-04983-333205242 · doi ↗ · pubmed ↗
- 6Sakanishi Y Tamaki K Mashimo K Relationship between recurrence of macular edema due to branch retinal vein occlusion and changes in choroidal thickness [J]Ophthal. Res.202164336336810.1159/000512357 PMC 825906433070137 · doi ↗ · pubmed ↗
- 7Tang F Xu F Zhong H Comparison of subfoveal choroidal thickness in eyes with CRVO and BRVO [J]BMC Ophthalmol.201919113310.1186/s 12886-019-1143-931226968 PMC 6588881 · doi ↗ · pubmed ↗
- 8Alis A Guler AM The effect of branch retinal vein occlusion on the vascular structure of the choroid [J]Photodiagn. Photodyn. Ther.20223710268710.1016/j.pdpdt.2021.10268734923154 · doi ↗ · pubmed ↗