Pediatric Critical Care Illness Severity Toolkit: Stata Commands for Calculation of Pediatric Index of Mortality and Pediatric Logistic Organ Dysfunction Scores
Razvan Azamfirei, Colleen Mennie, James C. Fackler, Sapna R. Kudchadkar

TL;DR
A new Stata toolkit simplifies and speeds up the calculation of pediatric critical care severity scores like PIM-3 and PELOD-2.
Contribution
A validated, open-source Stata toolkit for calculating PIM-3, Simplified PIM-3, and PELOD-2 scores with improved accuracy and performance.
Findings
The toolkit achieved 100% accuracy in synthetic data tests and manual checks.
Processing times were 9.74 seconds for Simplified PIM-3, 14.06 seconds for PIM-3, and 21.82 seconds for PELOD-2 on 10 million records.
The toolkit supports SI and Imperial units and includes a graphical interface and data validation.
Abstract
Illness severity scoring tools, such as PRISM III/IV, PIM-3, and PELOD-2, are widely used in pediatric critical care research. However, their application is hindered by complex calculation processes, privacy concerns with third-party online calculators, and challenges in accurate implementation within statistical packages. We have developed a comprehensive, open-source toolkit for implementing the PIM-3, Simplified PIM-3, and PELOD-2 scores. The toolkit includes the pim3 and pelod2 commands and is compatible with Stata versions 12 and above. It features robust data validation, error messaging, a graphical interface, and support for SI and Imperial units. The toolkit's accuracy was validated through unit testing and synthetic data, comparing results with existing implementations. In performance tests, the toolkit exhibited a median processing time of 21.82 seconds for PELOD-2, 14.06…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1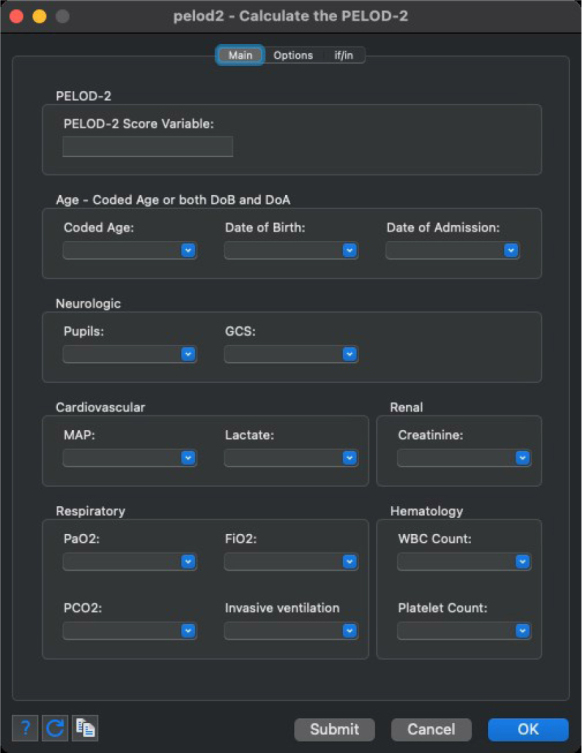 Fig. 2
Fig. 2|
| ||||||
|---|---|---|---|---|---|---|
| PELOD-2 | 21.92 | 21.47 | 21.82 | 21.32 | 22.70 | 21.82 (21.40–22.31) |
| PIM-3 | 14.06 | 13.59 | 14.20 | 13.71 | 14.08 | 14.06 (13.65–14.14) |
| Simplified PIM-3 | 10.14 | 9.69 | 9.73 | 9.74 | 9.81 | 9.74 (9.71–9.98) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSepsis Diagnosis and Treatment · Emergency and Acute Care Studies · Heart Failure Treatment and Management
Introduction
Outcome prognostication tools are indispensable in pediatric critical care research serving to control for the illness severity of pediatric intensive care unit patients. Several scores have been proposed, with the most notable being the Pediatric Risk of Mortality (PRISM III/IV), the Paediatric Index of Mortality 3 (PIM-3), and the Pediatric Logistic Organ Dysfunction-2 (PELOD-2) [1,2,3].
The application of each of these validated scoring systems involves complex, multi-step calculations. Online calculators are available for some of these scores, but they vary in their capacity to support multiple patients and the accuracy of their calculations. Additionally, submitting patient data to third-party websites may raise concerns about privacy and data protection. Implementing outcome prognostication scores in statistical packages is resource-intensive and prone to errors. As a result, researchers undertake custom implementation, leading to duplicated efforts and potential concerns about reproducibility if the implementation is incorrect.
Building on our previous work, where we detailed the development and implementation of a Stata command for calculating PRISM III and IV scores [4], this paper introduces a comprehensive toolkit for outcome prognostication in critically ill pediatric patients. This toolkit, including open-source implementations of the PIM-3, Simplified PIM-3, and PELOD-2 scores, aims to simplify these processes, thereby potentially reducing the challenges associated with their application in clinical research.
Methods
We employed the software framework described in our previous work to develop the pim3 and pelod2 commands. The commands accurately implement the methods described in the original publications [1,2,3, 5]. Where necessary, each command is equipped with robust data validation, clear error messaging, a user-friendly graphical interface, and support for alternative units. This further reduces potential errors caused by inappropriate conversions. Clear and comprehensive documentation is provided for the usage of the commands. The commands are compatible with Stata versions 12 and above.
We have consolidated these commands into a toolkit for pediatric critical care research (pccmtoolkit). In addition to the pim3 and pelod2 commands, the toolkit includes the prismscore command as well as other utilities that streamline data management and processing. The entire toolkit, as well as the individual commands, are accessible on the Statistical Software Components (SSC) archive (https://ideas.repec.org/s/boc/bocode.html). Development versions of the toolkit are available on GitHub (https://github.com/razvanazamfirei/pccmtoolkit).
Each command was validated through unit testing, as well as synthetic data. The results were compared to other implementations of the score and manual spot checks were performed to ensure that calculations reflect the original methods. As described previously, we generated 10,000,000 patient records with random realistic data and predefined PELOD-2 and PIM-3 scores. Data generation was done through a separate process that did not rely on the developed command. Each command was benchmarked by performing calculations over 5 distinct sets of 10,000,000 patient records, using Stata/MP 18.0 2-cores. Results are presented as median (IQR). Institutional Review Board approval was not required.
Results
The run-time results for each individual command are described in Table 1. The median time required to calculate scores for 10,000,000 records was 21.82 (21.40 – 22.31) seconds for PELOD-2, 14.06 (13.65 – 14.14) seconds for PIM-3, and 9.74 (9.71 – 9.98) seconds for the Simplified PIM-3 score. Each command achieved 100% accuracy in synthetic data tests, as well as in manual spot checks.
Additionally, the graphical user interface developed for these commands, which is depicted in Figures 1 and 2, enables intuitive variable specification and option selection. This interface streamlines the process for users, making it more accessible and efficient, particularly for those who may not be as familiar with traditional command-line operations.
Stata dialog depicting the graphical user interface for the PIM-3 and simplified PIM-3 commands.
Stata dialog depicting the graphical user interface for the PELOD-2 command.
Discussion
This study demonstrates the robustness and efficiency of the developed commands for calculating PELOD-2 and PIM-3 scores, indicating that the commands are highly reliable for research purposes. The median run times for the calculations suggest that these commands can process large datasets within a feasible time frame. The development of this toolkit serves as a valuable resource for pediatric critical care researchers, now offering the potential to calculate multiple types of severity scores over the same dataset. However, it is important to note that the validity of the scores depends on the underlying quality of the data. Scores may use different definitions for comorbidities and require different intervals for using clinical data. The documentation provided with the commands describes some requirements and limitations; however, it is not a substitute for accurate data extraction, or appropriate data cleaning and management.
Conclusion
Our work introduces a toolkit designed to enhance efficiency and accuracy in calculating the PELOD-2, PIM-3, and Simplified PIM-3 scores. Validation through synthetic data tests and manual spot checks confirmed 100% accuracy, ensuring reliability for research applications. This toolkit will serve as a resource for supporting pediatric critical care research, offering a streamlined approach to complex illness severity calculations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Leteurtre S Duhamel A Salleron JPELOD-2: an update of the P Ediatric logistic organ dysfunction score Crit Care Med 2013417176117732368563910.1097/CCM.0b 013e 31828 a 2bbd · doi ↗ · pubmed ↗
- 2Straney L Clements A Parslow RC Paediatric index of mortality 3: an updated model for predicting mortality in pediatric intensive care*Pediatr Crit Care Med 20131476736812386382110.1097/PCC.0b 013e 31829760 cf · doi ↗ · pubmed ↗
- 3Pollack MM Holubkov R Funai T The Pediatric Risk of Mortality Score: Update 2015 Pediatr Crit Care Med 2016171292649205910.1097/PCC.0000000000000558 PMC 5048467 · doi ↗ · pubmed ↗
- 4Azamfirei R Mennie C Fackler J Kudchadkar SR Development of a Stata Command for Pediatric Risk of Mortality Calculation Pediatr Crit Care Med 2023243 e 162e 1633686244610.1097/PCC.0000000000003149 · doi ↗ · pubmed ↗
- 5Baloglu O Nagy M Ezetendu C Simplified Pediatric Index of Mortality 3 Score by Explainable Machine Learning Algorithm Crit Care Explor 2021310 e 05613469329210.1097/CCE.0000000000000561 PMC 8528230 · doi ↗ · pubmed ↗