Physiotherapeutic Approach Towards Sensory and Motor Recovery in a Patient With Lateral Mass Fixation: A Report of a Rare Case
Jaee P Kapre, Pallavi Harjpal, Komal S Mandhane, Ketki Kunjarkar

TL;DR
A 23-year-old woman with cervical spine instability underwent surgery and physiotherapy, leading to improved mobility and daily functioning.
Contribution
This case report highlights the effectiveness of physiotherapy in improving sensory and motor recovery after C1-C2 lateral mass fixation for atlantoaxial dislocation.
Findings
Post-surgical physiotherapy improved the patient's balance, gait, and upper limb function.
Functional Independence Measure and Berg Balance Scale scores showed significant improvement.
Early intervention positively impacted the patient's quality of life and daily activities.
Abstract
Atlantoaxial dislocations (AAD) are a diverse set of C1-C2 rotatory subluxations that include the inferior and superior axial facet articulations. C1-C2 segments are both covered by cranial-cervical ligaments, indicating that AAD would damage both joints. Whenever the posterior elements are missing or impaired, lateral mass screw fixation has replaced alternative posterior cervical fixation procedures as the preferred treatment for securing the sub-axial cervical spine. An increase in muscle tone, hyperreflexia, pathological reflexes, digit/hand clumsiness, and gait deviations caused by spinal cord compression at the cervical level are the most common clinical features. A 23-year-old female patient came with the chief complaint of weakness, tingling sensation, and numbness in both upper and lower limbs along with imbalance while walking. She had a history of falls which was managed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2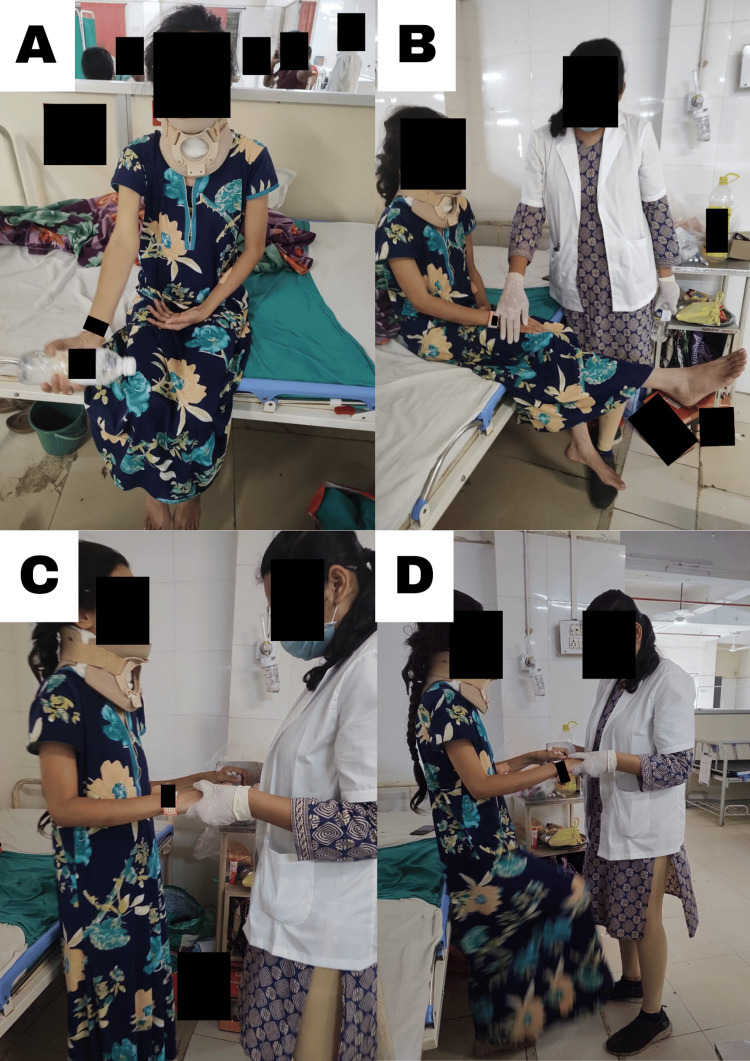 Figure 3
Figure 3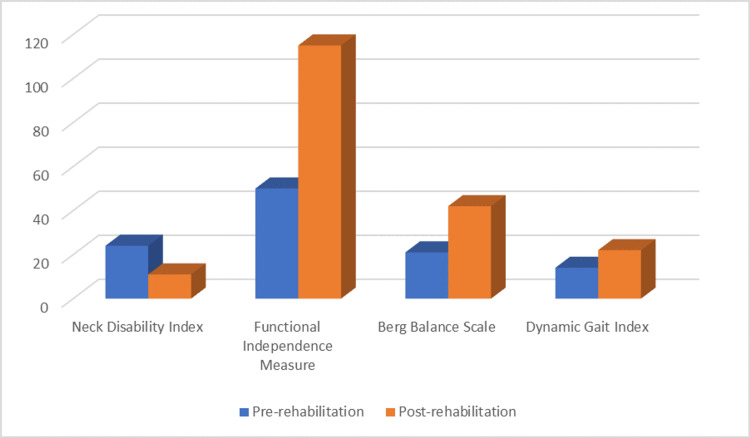 Figure 4
Figure 4| Sr. no. | Date of events | Consultation | Findings |
| 1 | On admission | Neurosurgery OPD | Weakness, tingling sensation, and numbness in both upper and lower limbs (L>R), imbalance while walking |
| 2 | 09/09/2022 | Neurosurgery ward | Admitted for observation |
| 3 | 10/09/2022 | Neurosurgery ward | X-ray (anterior subluxation of the atlas over the axis vertebrae on the left side) |
| 4 | 16/09/2022 | Neurosurgery ICU | Post-surgery (for one day) |
| 5 | 20/09/2022 | Neurosurgery ward | Call for neurophysiotherapy |
| ULTT | Right | Left |
| ULTT 1 | Negative | Positive |
| ULTT 2 | Negative | Positive |
| ULTT 3 | Negative | Positive |
| ULTT 4 | Negative | Negative |
| Problem list | Goals | Interventions |
| Both upper and lower limb weakening | To help boost upper and lower limb strength | Bilateral upper limb strengthening training (1/2 L water bottle and progress to 1 L). Bilateral lower limb strengthening training (1/2 kg weight cuff and progress to 1 kg weight cuff) |
| Tingling and numbness in both upper and lower limbs | To reduce tingling | Neural mobilization for the upper limb and lower limb (until the symptoms subsided) |
| Restricted cervical range of motion | To improve the cervical ranges | Active cervical range of motion exercises, neck isometric exercises, and chin tucks (muscle energy technique was used to train the neck muscles) |
| Reduced bed transfers | To facilitate transfers | Supine-to-side lying training, side lying-to-sitting training, and sitting-to-standing training |
| Decreased mobility | To achieve mobility | Swiss ball, trunk PNF with upper limb movements, transition training, and rolling facilitation |
| Impaired balance | To regain static and dynamic balance | Perturbation and balance training, weight shifting, dynamic standing balance with perturbations, dynamic standing balance with reach-outs, tandem walking, asking the patient to pick up the objects from the floor, and trunk rotation exercises |
| Impaired gait | For gait training | Parallel bar training exercises, spot marching, and obstacle walking |
| Tendency to attain neck flexion posture | For ergonomic modification | Ergonomic advice, cervical range of motion exercises, chin tucks, and stretches |
| MMT | Pre-rehabilitation | Post-rehabilitation | ||
| Right | Left | Right | Left | |
| Shoulder | 3+/5 | 2/5 | 5/5 | 4/5 |
| Elbow | 3/5 | 3/5 | 4/5 | 4/5 |
| Wrist | 3+/5 | 3/5 | 5/5 | 4/5 |
| Hip | 3/5 | 2/5 | 4/5 | 4/5 |
| Knee | 3/5 | 2/5 | 4/5 | 4/5 |
| Ankle | 3/5 | 3/5 | 4/5 | 4/5 |
| Outcome measures | Pre-rehabilitation | Post-rehabilitation |
| Neck Disability Index | 24/50 (moderate disability) | 11/50 (mild disability) |
| Functional Independence Measure | 50 | 115 |
| Berg Balance Scale | 21/56 | 42/56 |
| Dynamic Gait Index | 14/24 | 22/24 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpinal Fractures and Fixation Techniques · Nerve Injury and Rehabilitation · Scoliosis diagnosis and treatment
Introduction
Atlantoaxial subluxation is uncommon, and early detection and treatment are critical to achieving positive neurological results. Because of the specific biomechanics of these injuries, care for such traumatic unilateral atlantoaxial rotatory subluxation (AARS) differs; they frequently necessitate a personalised approach [1]. The currently accepted method for posterior cervical fusion uses lateral mass screw (LMS) fixation with plates or rods. Comparable post-operative segmental stability is provided by bilateral posterior cervical cages and lateral mass structures, both of which dramatically reduced the cervical range of motion [2]. A surgical procedure that is becoming more and more popular for treating atlantoaxial instability is the C1-C2 plate or rod and screw fixation. Excellent fusion rates are achieved with fixation using a plate or rod, a C1 or C2 screw, and structural bone grafting. The procedure is technically challenging and has a chance of vertebral artery, internal carotid artery, spinal cord, and hypoglossal nerve damage. A technique for C1-C2 fixation has been devised that involves bilaterally inserting C2 pedicle screws and rolling C1 titanium cable through the posterior arch of the atlas and the plate's cranial hole before fixing the C1-C2 plate [3]. Numerous aetiologies, such as trauma, infection, inflammation, or congenital defects, can cause atlantoaxial joint instability. A single piece of iliac crest bone graft was put between C1 and C2, and it was fastened with a steel wire in a sublaminar fashion according to Gallie's method of C1-C2 fusion. The medial facet line divides the lateral mass, which connects the superior and inferior articular processes, from the lamina. Injury to nearby nerve roots, vertebral arteries, or the spinal cord, facet joint violations, pseudoarthrosis, and screw fixation failure are the most common side effects of lateral mass fixation [4]. The posterior technique was first used to implant bilateral C1-C2 transarticular screws by Magerl and Seeman. The increased bony area for screw placement when compared to the Magerl method is one potential benefit of using the lateral bulk of the atlas for fixation [5].
A disorder known as cervical myelopathy is when the spinal cord is compressed at the cervical level of the spinal column, causing increase in muscle tone, exaggerated reflex, pathologic reflexes, clumsiness in the fingers and hands, and/or gait disruption [6]. Patients who are not treated may have significant paralysis and function loss. Upper extremity symptoms prevail in cervical myelopathy. These could include clumsy hands and a restricted capacity for fine motor activities including combing hair, holding small items, and buttoning shirts. Additionally, typical are radicular symptoms and neck aches. Surgery entails the decompression of the restricted region from the anterior or posterior and likely fusion [7]. And over 18 months of symptom duration, a reduction in cervical spine range of motion, and female gender are all indicators of a bad prognosis. Surgical decompression will help approximately 65% of individuals suffering from neck pain and radicular symptoms [8]. It has been demonstrated that cervical stenosis and myelopathy can be treated surgically, both anteriorly and posteriorly. It has been demonstrated that surgical procedures used to treat cervical stenosis and myelopathy, both anterior and posterior, improve patient outcomes [9].
Analgesic and anti-inflammatory medicines, muscle relaxants, physical therapy approaches, and orthoses are all examples of conservative treatment. Using some type of passive cervical manipulation, cervical collar or halter or skeletal traction, and halo immobiliser are all alternatives for realigning the neck in a decreased posture in physical therapy [10]. Cervical halter traction in the supine position for 24-48 hours, accompanied by mobility with orthotic immobilisation with active range of motion activities, is continued until free mobility is restored [11].
Case presentation
Patient information
A 23-year-old female who was a student residing in Amravati came with chief complaints of weakness, tingling sensation, and numbness in both upper and lower limbs for four months, specifically more on the left side of the body. She also complained of imbalance while walking for three months. The patient was alright for four months, and she had a fall, which was managed conservatively. But later on, she slowly and gradually started realizing that there is a bilateral lower limb and upper limb weakness (the left side more than the right). She also has a previous operated history of hemorrhoidectomy, 15 days back. Then, she visited a private hospital where it was managed conservatively by medications. Then, the patient came to our neurosurgery outpatient department (OPD) with the complaints mentioned above, and she was suggested for a magnetic resonance imaging (MRI), computed tomography (CT) scan, and X-ray of the neck. The MRI revealed loss of cervical lordosis, and the CT scan revealed os odontoideum along with atlantoaxial dislocation (AAD). The neurophysician suggested a Philadelphia collar for neck stabilisation, and she was admitted to the neurosurgery ward on 09/09/22. Then, the patient was operated on 16/09/22 for C1-C2 lateral mass fixation. On 20/09/22, she was referred to physiotherapy for further management and rehabilitation, and after a few months, she was able to walk independently with good balance. The timeline of events is shown in Table 1.
Clinical findings
The patient was evaluated while lying supine on a plinth. The vital indicators such as heart rate were increased to 78 beats/min; the respiratory rate was 17 breaths/min. On observation, the patient had an endomorphic build and was wearing a Philadelphia collar for neck stabilisation. The upper extremity was situated by the body's sides, with the forearm in pronation. In bilateral lower limbs, her hips were extended, abducted, and externally rotated with the knee in extension and the ankle in slight plantar flexion. There was the use of accessory muscles of respiration with the thoracoabdominal type of breathing due to a recent operation of the neck region. There was no evidence of oedema or pressure sores. On palpation, there were no noteworthy findings in the context of warmth, tenderness, and swelling. On examination, the higher mental functions were normal, i.e., the cognition of the patient was not impaired as the score was 29/30 on the Mini-Mental State Examination (MMSE). Her short- and long-term memory was intact. In special senses, only VIII (sensory) cranial was impaired. In the sensory examination, the superficial, deep, and cortical sensations were intact bilaterally over the upper and lower limbs along with the trunk. In the motor examination, there was weakness in both upper and lower limbs with truncal instability. Hoffman's sign and Romberg's sign were also positive. On manual muscle testing (MMT), her upper limbs had a grade of 3/5, and her lower limbs had a grade of 3+/5. Her deep tendon reflexes were normal. The neural tension test was positive for the median and radial nerve on the left side as shown in Table 2.
Clinical diagnosis
The patient received a cervical spine MRI examination, which demonstrated a decrease in cervical lordosis. CT scan showed os odontoideum and 6 mm anterior subluxation of the atlas over the axis vertebrae on the left side. X-ray showed anterior subluxation of the atlas over the axis vertebrae (with red arrow) on the left side in Figure 1. Figure 2 shows the post-operative X-ray of the patient's cervical region.
Anterior subluxation of the atlas over the axis vertebrae visible on X-ray of the cervical spine taken in flexion position
Post-operative C1-C2 lateral mass fixation
Physiotherapy intervention
The patient was properly informed of the benefits of physiotherapy, and the procedure was quickly presented to her. After four days of operation, physiotherapy was started, and the patient was shown visually and orally how to do the following activities which are shown in Table 3 and Figure 3. The following treatment procedure was administered once a day for 10 repetitions of one set with enough rest. An appropriate amount of intervals was also offered to the patient to avoid weariness.
Various exercises performed by the patient(A) Upper limb strengthening exercises. (B) Dynamic quadriceps strengthening. (C) Balancing training. (D) Alternative leg raising
Follow-up and outcome measures
There was an improvement in the MMT score, and the outcome measures, i.e., Functional Independence Measure, Neck Disability Index, Berg Balance Scale, and Dynamic Gait Index, are shown in Table 4, Table 5, and Figure 4.
Pre-rehabilitation and post-rehabilitation outcome measures
Discussion
In the majority of patients, rigid fixation with transarticular screws has been shown to be a secure and reliable technique for C1-C2 stabilisation. In comparison to wire/cable fixation, rigid fixation of C1-C2 through transarticular screw implantation provides rapid stability and has superior biomechanical qualities [12]. Adults occasionally experience the trauma of subluxation of the atlantoaxial joint, but there is currently no accepted standard of care. Important static stabilisers, the transverse and alar ligaments, stop the anterior translation of the C1 on the C2 vertebrae [13]. The cervical collar must be worn for at least eight hours continuously per day for three months, with usage time decreasing throughout the course of treatment, along with general rest when doing tasks [14]. When there is no neurological damage following a cervical injury, the patient's prognosis is worse in the short to medium term due to the delayed diagnosis and initial stabilisation. Reduction and early fusion are definite treatments to stop neurological problems from developing. The primary objectives of the physiotherapy programme are to increase ranges of motion at the cervical spine and shoulder, increase strength, enhance hand functions, improve balance and coordination, and avoid any additional deformity [15].
The congenital fusing of the atlas and the occipital bone is termed atlantooccipital fusion. It is one of the uncommon skeletal variants of the craniocervical area, occurring in 0.12-0.72% of the population [16]. Atlantoaxial Rotatory Dislocations (AARDs) are a diverse set of post-traumatic disorders that are common in children but uncommon in adults [17]. One of the physiotherapeutic rehabilitative uses of task-specific balance rehabilitation is perturbation-based balance training (PBT). Neural mobilization is proven to be effective to reduce tingling in such cases. The muscle energy technique prevents muscle fatigue and enables the strengthening of the muscle to produce better outcomes. When exposed to repeated perturbations, the neuromotor system may be encouraged to acquire the necessary neurophysiological modifications and sensorimotor skills to prevent collapsing [18].
Conclusions
C1 lateral mass fixation is a safe alternative for upper cervical fixation with several potential advantages versus other techniques. Our study emphasises the improvement of patients based on physiotherapeutic interventions that are planned to improve the functional independence and quality of life of the patient. Rehabilitation of such patients requires time to recover, but with proper week-wise intervention, the patient can return to her normal daily life. Neurorehabilitation has different approaches, due to which the recovery of the patient can be fastened. In this case, after the surgery, physiotherapy plays a vital role in the patient's recovery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Traumatic atlantoaxial rotatory subluxation in adults - a case report and literature review Surg Neurol Int Horsfall HL Gharooni AA Al-Mousa A Shtaya A Pereira E 3761120203340891010.25259/SNI_671_2020 PMC 7771491 · doi ↗ · pubmed ↗
- 2Biomechanical evaluation of DTRAX® posterior cervical cage stabilization with and without lateral mass fixation Med Devices (Auckl) Voronov LI Siemionow KB Havey RM Carandang G Patwardhan AG 285290920162760193410.2147/MDER.S 111031 PMC 5003555 · doi ↗ · pubmed ↗
- 3C 2 pedicle screw and plate combined with C 1 titanium cable fixation for the treatment of atlantoaxial instability not suitable for placement of C 1 screw J Spinal Disord Tech Xiao ZM Zhan XL Gong DF Chen QF Luo GB Jiang H 5145172120081883636410.1097/BSD.0b 013e 31815 c 5fba · doi ↗ · pubmed ↗
- 4Lateral mass fixation in subaxial cervical spine: anatomic review Global Spine J Mohamed E Ihab Z Moaz A Ayman N Haitham AE 3946220122435394510.1055/s-0032-1307261 PMC 3864406 · doi ↗ · pubmed ↗
- 5Anterior atlanto-occipital transarticular screw fixation: a radiological evaluation World Neurosurg Xu X Ji W Liu X Kong G Huang Z Chen J 094128201910.1016/j.wneu.2019.04.18331048054 · doi ↗ · pubmed ↗
- 6Clinical indicators of surgical outcomes after cervical single open-door laminoplasty assessed by the Japanese Orthopaedic Association Cervical Myelopathy Evaluation Questionnaire Spinal Cord Nagoshi N Tsuji O Okada E 6446515720193079254010.1038/s 41393-019-0258-4 · doi ↗ · pubmed ↗
- 7Cervical radiographical alignment: comprehensive assessment techniques and potential importance in cervical myelopathy Spine (Phila Pa 1976) Ames CP Blondel B Scheer JK 06038201310.1097/BRS.0b 013e 3182 a 7f 44924113358 · doi ↗ · pubmed ↗
- 8The most influential publications in cervical myelopathy J Spine Surg Donnally CJ 3rd Butler AJ Rush AJ 3rd Bondar KJ Wang MY Eismont FJ 77077942018 https://pubmed.ncbi.nlm.nih.gov/30714009/.3071400910.21037/jss.2018.09.08PMC 6330587 · doi ↗ · pubmed ↗