Fatal Viscerocutaneous Brown Recluse Envenomation With Orbital Compartment Syndrome
Jonathan W Meadows, Nima Shayesteh, Eric Crandall, Sarah A Watkins

TL;DR
A 44-year-old man died from a rare severe reaction to a brown recluse spider bite, which caused life-threatening eye and systemic complications.
Contribution
This case report highlights a rare fatal outcome of brown recluse envenomation with orbital compartment syndrome.
Findings
The patient developed fatal systemic loxoscelism following a brown recluse spider bite.
Orbital compartment syndrome required emergency surgical intervention.
The case underscores the potential severity and rapid progression of brown recluse envenomation.
Abstract
Loxosceles is an arachnid genus comprising several species in the United States, popularly known as brown recluse spiders. The venom is cytotoxic, complex, and has a mixture of many proteins, some of which function as proteases. Envenomation can cause necrotic skin lesions that may become extensive and take many months to heal. Even more rarely, venom may cause systemic effects, leading to widespread hemolysis, coagulopathy, and death. These symptoms typically occur rapidly within 24-48 hours following the bite. We describe a rare case of a 44-year-old male with fatal systemic loxoscelism with orbital compartment syndrome requiring emergent lateral canthotomy and cantholysis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1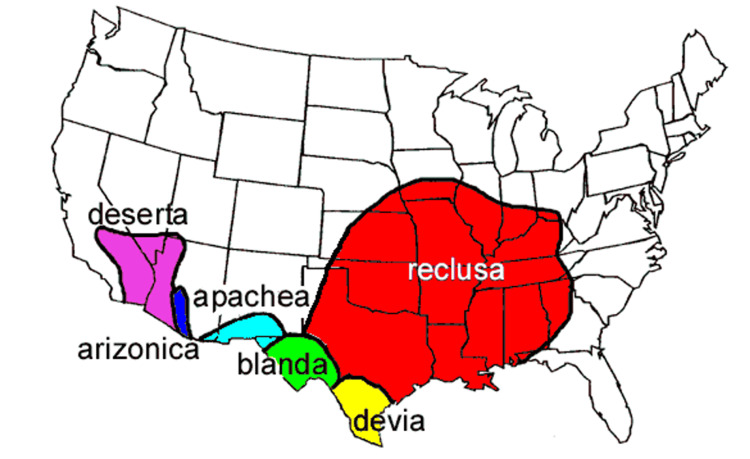 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMethemoglobinemia and Tumor Lysis Syndrome · Biomedical Research and Pathophysiology · Erythrocyte Function and Pathophysiology
Introduction
In 2021, there were 566 brown recluse spider bite cases mentioned, with one death in the USA [1]. There are 11 species of the genus Loxosceles in the USA. Four are in Texas, each with a different geographic distribution [2]. South America’s L. laeta has the highest mortality [2]. Loxosceles is from the Greek word meaning “crooked or slanted legs” when resting [2]. It has three non-touching pairs of eyes, tan legs, and a classic violin-shaped pattern on the dorsal cephalothorax, noting the “violin or fiddleback spider” feature [2]. There is body and color variation among species, leading to potential misclassification and excessive or incorrect treatments [2].
The arachnid is nocturnal, synanthropic, and building dwelling; there is no clear correlation with direct bite frequency as the spider population increases alongside humans [2]. Painless or skin prick bites usually occur during sleep and while changing clothes when it is inconspicuously hidden and suddenly disturbed [2]. Locations include the leg, arm, and torso in most cases, and only 0.6-1.5% are on the face, neck, shoulder, buttocks, or genitalia [2]. The venom is hyaluronidase and cytotoxic sphingomyelinase-D venom mixture, promoting tissue penetration and necrosis with hemolysis, respectively, noting the “red, white, and blue sign” and risk for systemic involvement [1-3]. Through a complaint of a bite, geographical information, clinical manifestations, and laboratory evidence, the diagnosis is either putative, presumptive, probable, or documented [2]. We report a probable viscerocutaneous loxoscelism envenomation by a Loxosceles spider (possibly L. apachea, L. blanda, or L. reclusa) with lateral canthotomy in West Texas.
Case presentation
A 44-year-old male with no past medical history presented to a freestanding emergency department (ED) reporting a spider bite to his face, just superior to the right eyebrow, that occurred while changing a ceiling fan approximately 24 hours earlier. He caught the spider, noting it to be a brown recluse, but did not bring it to the ED or take any photographs. The family also confirmed the spider bite. He denied any other initial symptoms. However, he awoke approximately eight hours later after sleeping due to facial pain, swelling, and progressive right-eye vision loss. This worsened throughout the day, ultimately prompting him to go to the ED the next evening approximately 24 hours after the initial bite.
In the ED, his triage vitals were as follows: heart rate (HR) of 129 bpm, blood pressure (BP) of 108/67 mmHg, respiratory rate (RR) of 18 breaths per minute, temperature (T) of 36.8°C, and oxygen saturation of 91% on room air. The exam was notable for a puncture mark above the right eyebrow, right-sided facial ecchymosis, swelling extending to the jawline and lips, and marked right eye proptosis. The ocular globe was poorly visualized due to severe eyelid edema with serosanguinous non-purulent discharge. Decompensation occurred within 15 minutes after the initial presentation. On the cardiac monitor, hypoxia occurred despite supplemental oxygen, and hypotension was noted with a mean arterial pressure of 30 mmHg. Diaphoresis, nausea, and worsening facial swelling ensued. Intravenous epinephrine and dopamine were administered, and intubation was completed for airway protection in the setting of clinical tracheal deviation. During intubation, tracheal deviation was confirmed via direct laryngoscopy (DL) and attributed to severe facial edema. A 7.5 Fr endotracheal tube was placed along with a left internal jugular (IJ) central venous catheter (CVC). Medications used for intubation included succinylcholine and etomidate, and a push dose of epinephrine 0.1 mg. Sedation was maintained with propofol. An orogastric tube was inserted, and the output was a mixture of 1300 mL of coffee-ground material and frank blood. As the right-sided proptosis continued to worsen while awaiting transfer to an intensive care unit (ICU), a right lateral canthotomy with cantholysis was performed for suspected ocular compartment syndrome, which resulted in the release of a significant amount of serosanguinous fluid and clinical improvement of the proptosis.
Laboratory studies were notable for a WBC count of 7.5 x 103 cells/mm3, 53% bands, and thrombocytopenia with platelets at 99 x 103/mm3. Initial hemoglobin was 10.1 gm/dL. There was metabolic acidosis with bicarbonate <10 mEq/L, an anion gap of 26.0 mEq/L, a delta gap of 14.0 mEq/L, and a delta ratio of 1.0, suggesting pure anion gap acidosis. Acute kidney injury was noted with blood urea nitrogen (BUN) at 27 mg/dL and creatinine at 3.9 μg/g. An initial serum lactate was unable to be performed due to resource constraints. Hemolysis and disseminated intravascular coagulation (DIC) were diagnosed based on the following: fibrin degradation products >20 mcg/mL, fibrinogen = 501 mg/dL, elevated D-dimer at 10.8 mcg/mL FEU, elevated international normalized ratio at 2.0, and elevated activated partial thromboplastin time (aPTT) at 62.6 seconds. A lactate dehydrogenase test was ordered with no result reported, and a haptoglobin was not ordered. The International Society on Thrombosis and Haemostasis DIC score was 6, consistent with DIC. Liver enzymes were elevated with aspartate aminotransferase at 459 units/L, alanine aminotransferase at 112 u/L, and total bilirubin at 1.1 mg/dL. Rhabdomyolysis was noted given myoglobin at 3,282 ng/mL and creatine kinase at 635 u/L.
The patient was transferred to the ICU and the regional poison control center was contacted. Dopamine and norepinephrine were maximally administered but persistent hypotension continued at 81/49 mmHg with tachycardia at 128 bpm and temperature at 99°F. His face was swollen and dark in color. Lactic acid level was 8.9 mmol/L. The medical toxicologist recommended supportive care, including steroids, blood products, reversal of any coagulation abnormalities, a bicarbonate drip, and plasmapheresis consideration. Unfortunately, the patient continued to deteriorate and not all recommended treatments were started. Nephrology was consulted for continuous renal replacement therapy (CRRT) but the patient was too unstable due to profound hypotension despite four vasopressors, including epinephrine, dopamine, and dobutamine. For the profound acidosis, sodium bicarbonate 150 mEq was administered intravenously. The patient developed asystole with a lactate of greater than 12.2 mmol/L and died approximately 37 hours after the spider bite.
Discussion
This is a case of probable viscerocutaneous loxoscelism envenomation with subsequent DIC, acute hypoxic respiratory failure, gastric hemorrhage, and right ocular proptosis requiring lateral canthotomy with cantholysis. The differential diagnosis includes spider bites from other genera, including Tegenaria agrestis (hobo spider, northwestern brown spider, and Walckenaer's spider) and Kukulcania hibernalis (southern common house spider, most commonly misidentified) [1,3]. An example of a brown recluse spider notes the aforementioned distinguishing features (Figure 1). Other differential diagnoses were sepsis, allergic dermatitis, necrotizing fasciitis, cutaneous leishmaniasis, fungal infection, pyoderma gangrenosum, chemical burns, ischemic vascular disorders, and drug use [1,2]. The previously published mnemonic “NOT RECLUSE” can aid in clinical diagnosis, but this mnemonic needs further validation [4]. Systemic loxoscelism cases have been published previously, with three brown recluse bites involving the eyes, and one of those three involving lateral canthotomy [5-7].
An example of a brown recluse spider.Image credits: Sarah A. Watkins.
Poison control recommendations were implemented except for plasmapheresis and CRRT. Fresh frozen plasma may not have been indicated (based on the prothrombin time/aPTT ratio of 0.38 and normal fibrinogen), and retrobulbar and gastrointestinal bleeding would not have supported anticoagulant use. Treatment should address cutaneous and symptomatic features simultaneously, including wound care, immobilization, tetanus prophylaxis, analgesics, antipruritics, antibiotics, and follow-up for delayed corrective surgery and chronic wound care management [2]. Equivocal evidence is demonstrated for dapsone use; colchicine, tetracycline, hyperbaric oxygen therapy, corticosteroids, and nitroglycerin have shown no benefit [2,3]. Ongoing vaccine trials and use of antivenom are noted in Latin America, with none indicated in the USA [2,4,8,9].
Previously authors have proposed a secondary warm autoimmune hemolytic anemia (AIHA) process, but the mechanism is unknown. Standard initial treatments are indicated for the ED setting with admission [10]. No Coombs test was completed, but it may be warranted in future cases.
Regarding pregnant and pediatric patients, management is similar. Data from the National Poison Data System from 2009 to 2018 showed no maternal deaths; however, three fetal deaths were reported [11]. There was a report of a pregnant patient from Mexico who had systemic features and was provided standard treatments, including dapsone and wound care [12]. A review of pediatric brown recluse pediatric complications and outcomes found 26 cases over 10 years and made similar recommendations for treatment [13]. One pediatric case report described myocarditis, pulmonary edema, and cardiogenic shock, and the patient recovered with treatment that included steroids, plasmapheresis, and intravenous immunoglobulin [14].
The main limitation of this case report is that we were unable to definitively determine that the patient was envenomated by a Loxosceles spider due to no specimen being presented to the ED clinician, photographic evidence or confirmatory testing, such as a passive hemagglutination inhibition test (PHAI) assay and toxin enzyme-linked immunosorbent assay, which were not performed due to the patient’s rapid clinical deterioration and limited resource availability [3,15]. Furthermore, limited testing was performed, such as blood cultures, due to rapid decompensation. Standard evaluation of infection and sepsis was not completed. Laboratory data were also limited and can be typical of poison control center cases. There are other case reports noting a differential diagnosis of skin infection and spider bites [16]. The temporal association of the patient’s reported spider bite, the geographic distribution of the spider, the clinical features, and the clinical deterioration are nevertheless highly suspicious for viscerocutaneous loxoscelism envenomation (Figure 2) [2,17].
Geographic distribution of Loxosceles species.Figure adapted from [17]. Permission for use was obtained from the original publishers.
Conclusions
Systemic Loxosceles envenomation is a rare condition with potentially high mortality, causing rapid clinical deterioration and possible need for lifesaving surgical intervention. The acute care clinician must have a high index of suspicion for visceral manifestations in the presence of cutaneous Loxosceles envenomation. Systemic loxoscelism may warrant admission, interdisciplinary team coordination, and significant other healthcare resources. Future opportunities for research include standardization of laboratory work-up, such as consideration of Coombs testing, and broadening treatment options, such as antivenom therapy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 12021 Annual Report of the National Poison Data System© (NPDS) from America's Poison Centers: 39th Annual Report Clin Toxicol (Phila) Gummin DD Mowry JB Beuhler MC 13811643602022 https://pubmed.ncbi.nlm.nih.gov/36602072/3660207210.1080/15563650.2022.2132768 · doi ↗ · pubmed ↗
- 2Loxosceles spiders Critical Care Toxicology: Diagnosis and Management of the Critically Poisoned Patient Malaque CMS Vetter RS Entres M 25772594 Cham, Switzerland Springer 2017
- 3Arthropods Goldfrank's Toxicologic Emergencies Repplinger DJ Hahn I 15441547 New York, NY Mc Graw-Hill Education 2019 https://accesspharmacy.mhmedical.com/content.aspx?sectionid=210276505&bookid=2569#216826897
- 4NOT RECLUSE—a mnemonic device to avoid false diagnoses of brown recluse spider bites JAMA Dermatol Stoecker WV Vetter RS Dyer JA 37737815320172819945310.1001/jamadermatol.2016.5665 · doi ↗ · pubmed ↗
- 5Brown recluse spider bite to the eyelid Ophthalmology Jarvis RM Neufeld MV Westfall CT 1492149610720001091989610.1016/s 0161-6420(00)00183-4 · doi ↗ · pubmed ↗
- 6Emergency department death from systemic loxoscelism Ann Emerg Med Rosen JL Dumitru JK Langley EW Meade Olivier CA 4394416020122230533310.1016/j.annemergmed.2011.12.011 · doi ↗ · pubmed ↗
- 7Loxosceles arizonica bite associated with shock Ann Emerg Med Bey TA Walter FG Lober W Schmidt J Spark R Schlievert PM 701703301997936058710.1016/s 0196-0644(97)70092-1 · doi ↗ · pubmed ↗
- 8Partial in vivo protection against Peruvian spider Loxosceles laeta venom by immunization with a multiepitopic protein (r MEP Lox)Toxicon Quispe RL Jaramillo ML Torres-Huaco F Bonilla C Isasi J Guerra-Duarte C Chávez-Olórtegui C 1521520223566062510.1016/j.toxicon.2022.05.044 · doi ↗ · pubmed ↗