Eighteen-Year Follow-up After Autologous Chondrocyte Implantation on Medial and Lateral Femoral Condyles: A Case Report
Austin M Paradis, Scott D Gillogly

TL;DR
A 37-year-old man showed long-term recovery after a surgery to repair knee cartilage defects using his own cartilage cells.
Contribution
This case report provides an 18-year follow-up showing successful long-term outcomes of autologous chondrocyte implantation for knee cartilage repair.
Findings
The patient showed clinical improvement over 18 years following autologous chondrocyte implantation.
Arthroscopic images confirmed robust cartilage regeneration on the medial femoral condyle.
The case supports autologous chondrocyte implantation as a long-term solution for large knee cartilage defects.
Abstract
Articular cartilage defects are common injuries of the knee. The defects often progress in size and produce significant clinical symptoms due to the lack of intrinsic repair or regenerative capacity of articular cartilage. With the failure of nonoperative treatment options, surgical treatment is indicated and includes palliative, reparative, and regenerative options. For large defects of the femoral condyles, trochlea, or patella, autologous chondrocyte implantation can provide successful and long-lasting results. Presented is the case of a 37-year-old male with an 18-year follow-up to autologous chondrocyte implantation for extensive left knee articular cartilage defects of the medial and lateral femoral condyles. Recovery from articular cartilage defects is shown through both clinical improvement of the patient and arthroscopic photographs of robust autologous articular cartilage on…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
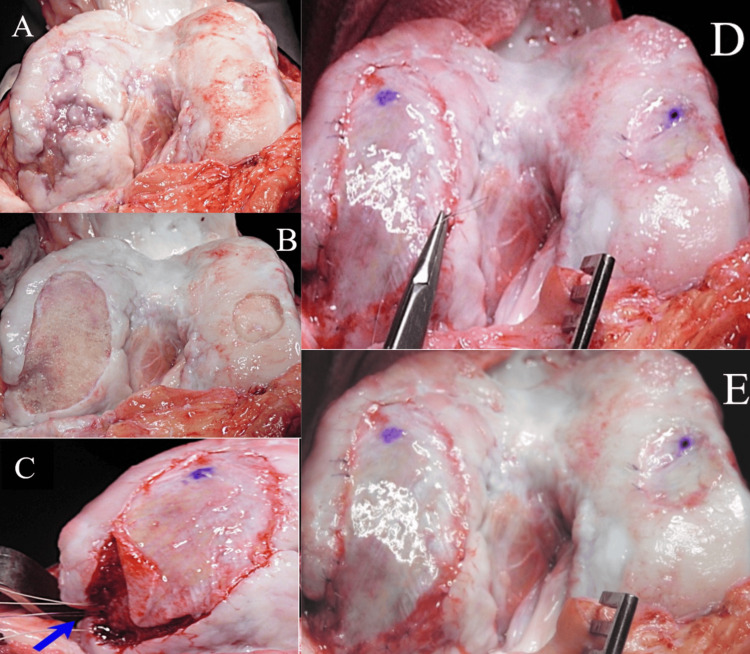 Figure 1
Figure 1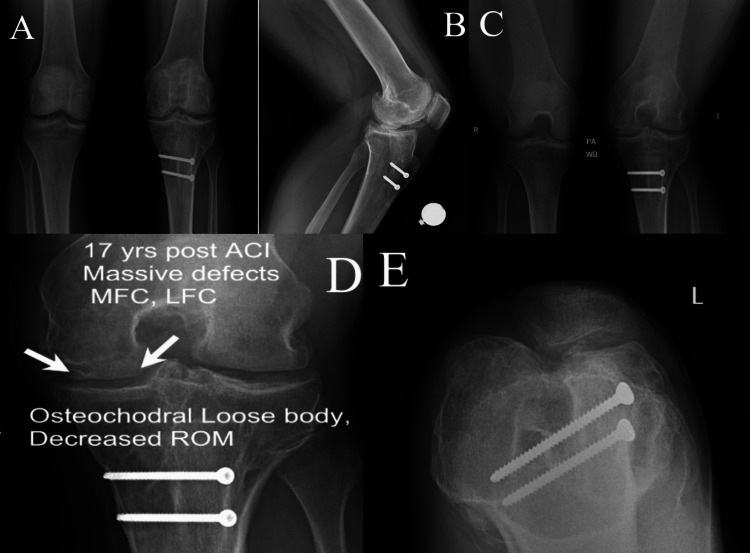 Figure 2
Figure 2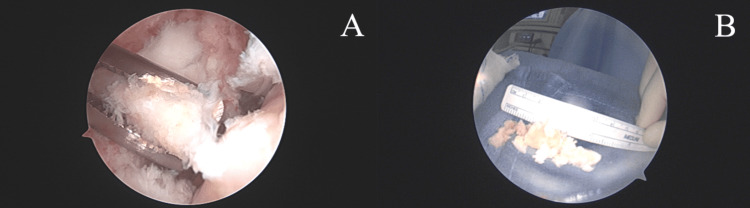 Figure 3
Figure 3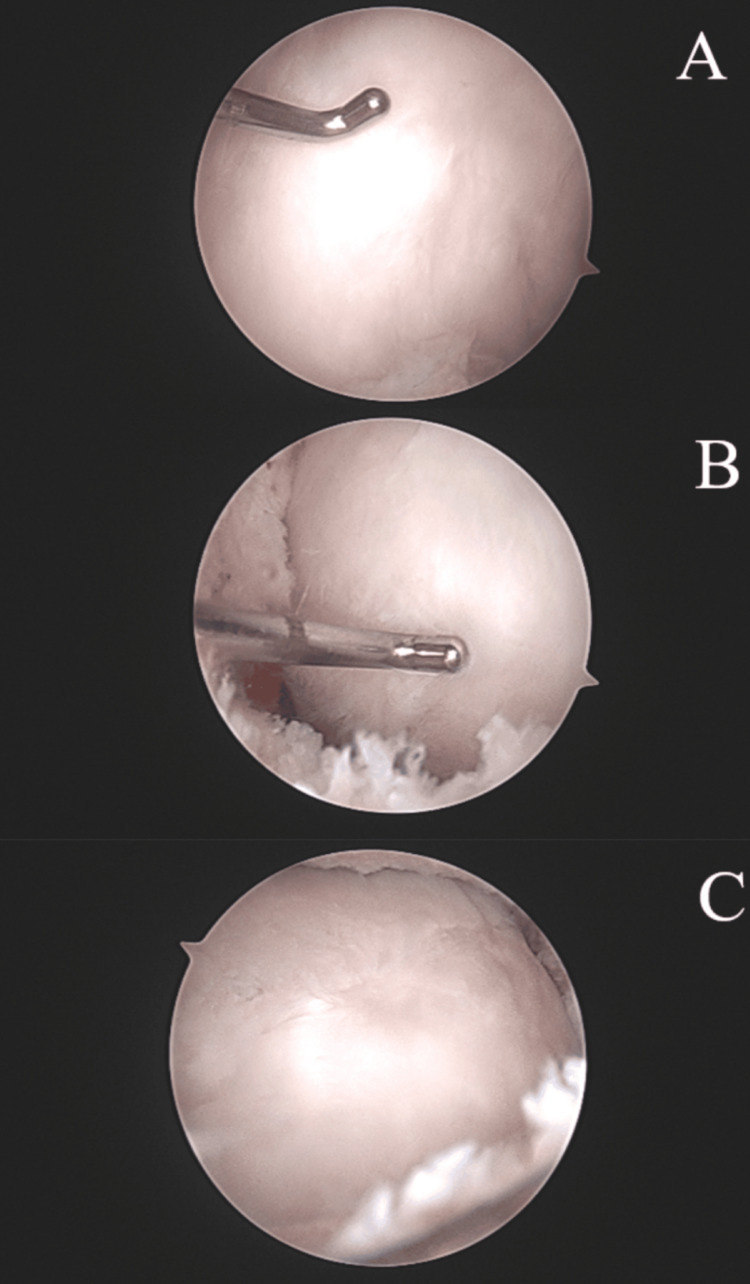 Figure 4
Figure 4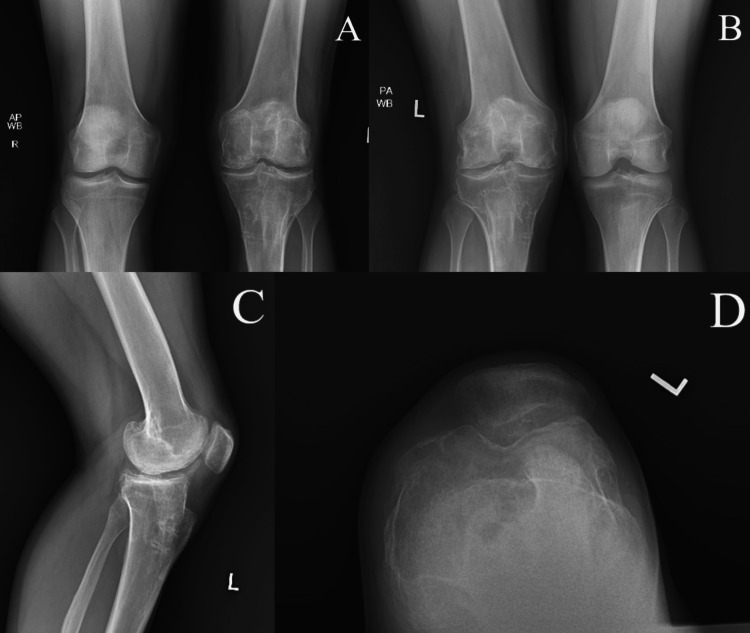 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOsteoarthritis Treatment and Mechanisms · Knee injuries and reconstruction techniques · Total Knee Arthroplasty Outcomes
Introduction
Articular cartilage defects in the knee can produce pain and disability symptoms to the same extent as advanced osteoarthritis or anterior cruciate ligament (ACL) deficiencies [1]. Such deficits greatly impair athletic performance and quality of life parameters. Cartilage defects are known to expand in size over time causing further degradation of articular cartilage [2]. Therefore, earlier detection and definitive treatment can provide symptom relief and improved function while delaying or preventing progression to osteoarthritis [3].
This case report documents a 37-year-old male with an 18-year follow-up after autologous chondrocyte implantation (ACI) on extensive left knee defects of the medial and lateral femoral condyles. This case further supports the long-term benefits of ACI as a surgical intervention for large full thickness articular cartilage defects in the knee. Autologous chondrocyte implantation has been shown to be an effective and durable solution for the treatment of large full-thickness cartilage lesions of the knee joint. Studies support that the clinical and functional outcomes remain high even 10 to 20 years after the implantation [4].
Case presentation
A 37-year-old male presented for an evaluation of a complex left knee problem dating back to a high school sports injury in 2001. At an outside institution, he had undergone an ACL reconstruction followed by an indolent intra-articular infection, debrided, and treated with long-term antibiotics. He later underwent a revision ACL reconstruction at another institution, at which time the large cartilage defects were noted and a cartilage biopsy was obtained. He was then referred to our center in early 2003 for treatment of his cartilage defects with ACI. Intraoperative photographs of the patient’s ACI in 2003 were taken (Figures 1A-1E). At the time of surgery, he underwent first-generation ACL of a 59 mm x 29 mm medial femoral condyle defect and a 28 mm x 18 mm lateral femoral condyle defect, and concomitant anteromedialization of the tibial tubercle and hardware removal of an ACL screw. Postoperatively the patient was treated with a continuous passive motion (CPM) machine (for six hours per day), quad sets, straight leg raises, passive range of motion, and partial weight bearing for four weeks. He was then allowed to advance motion, core, pelvic, and femoral strengthening, and weight bearing as tolerated. At one year postoperatively, he was allowed to advance to full activity although he voluntarily “retired” from cutting sports (Figures 1A-1E).
Intraoperative photographs of the patient’s ACL in 2003The medial and lateral condylar defects shown are undebrided (A) and then debrided (B). Anchors for the uncontained area were placed (C) and the periosteum was fully sutured in place with interrupted 6-0 Vicryl sutures (D). The final repair after the suture line is sealed with fibrin glue and the autologous cells injected below the secured periosteal membrane is shown (E).ACL: anterior cruciate ligament
In August 2020, the patient was evaluated for complaints of progressive pain in the left knee over the past year. He described the pain to occur on attempted squatting or kneeling. He also complained of hardware pain around his tibial tubercle and said that the screws are palpable and bothered him with physical activity. Examination demonstrated a 1+ effusion, palpable loose body, motion from full extension to 110 degrees, trace Lachman, negative pivot, and negative anterior and posterior drawer testing. He was neurovascularly intact and had a good quadriceps tone. There was tenderness to palpation over the prominent screws about the tibial tubercle.
Radiographs of both knees were obtained and demonstrated the presence of large loose bodies with preservation of the medial and lateral joint spaces. There was a questionable intra-lesional osteophyte of the trochlea on a sunrise view (Figures 2A-2E). Based on the patient’s symptoms correlating with radiographs and examination, arthroscopic removal of loose bodies, debridement, and removal of retained hardware was recommended.
Anterior-posterior (A), lateral (B), posterior-anterior (C +D), and sunrise (E) radiographs of the patient’s knees upon initial examination; panel D is increased magnification of panel C with text superimposed to highlight the presence of an osteochondral loose body
The patient then underwent the recommended procedure with an exam under anesthesia unchanged from the preoperative exam. In addition to standard anterolateral and anteromedial portals, superomedial and superolateral portals were made to assist with the lysis of extensive adhesions and the removal of large loose bodies that were partially embedded in scar tissue in the anterior and patellofemoral compartments. The loose body in the anterior compartment was greater than three centimeters in size. The loose bodies were fragmented and resected from the scar tissue so that they could be removed through the portals (Figures 3A-3B). After lysis of the adhesions and removal of the osteochondral loose bodies, there was full visualization of the femoral condyles. The medial femoral condyle showed robust smooth articular cartilage with appropriate firmness with the ACL site fully repaired. The lateral femoral condyle showed intact repair tissue with a new area of chondral involvement in the lateral trochlea, which was debrided, and the chondral flap was stabilized via chondroplasty (Figure 4A-4C).
Intraoperative, arthroscopic photos of removal of osteochondral loose bodies (A) and the accumulated size of the loose bodies removed (B).
Intraoperative, arthroscopic photos (A+B+C) of the medial femoral condyle 17 years post autologous chondrocyte implantation
The patient’s passive range of motion was improved to 120 degrees of flexion. The patient’s retained hardware was then removed from the tibial tubercle through small incisions. The wounds were all closed with absorbable sutures. Postoperatively, the patient was treated with calf pumping exercises, quad sets, passive range of motion, and weight bearing as tolerated for three weeks and progressed to femoral strengthening and return to full activity as tolerated. At four weeks postoperatively, the patient showed healed incisions, full extension, flexion to 115 degrees, good stability, decreased crepitus, and improved comfort.
He was again re-evaluated 15 months post arthroscopic removal of loose bodies with lysis of adhesion and partial synovectomy and 18 years post autologous chondrocyte implantation of the medial and lateral femoral condyles. Examination showed full extension and flexion to 120 degrees with no effusion. There was good stability on varus and valgus testing, as well as anterior and posterior drawer testing, and no significant pain during open chain terminal knee extension. Radiographs showed a preserved medial joint space narrowed by 25% with mild persistent subchondral irregularity (Figures 5A-5D). The patient stated that he was able to participate in cardiovascular fitness workouts and training such as running. He was able to participate as tolerated in physical activities with no restrictions.
Anterior-posterior (A), posterior-anterior (B), lateral (C), and sunrise (D) radiographs of the patient's left knee one year post arthroscopic removal of loose bodies with lysis of adhesions, partial synovectomy, and hardware removal. Radiographs were also 18 years post autologous chondrocyte implantation. AP and PA showed a preserved joint space with mild subchondral irregularity.
Discussion
An articular cartilage defect involves an injury to the cartilage that, in turn, causes disruption of proteoglycan synthesis, increased tissue hydration, and collagen disorganization. These characteristics lead to a progression of the cartilage injury, which causes a degenerative cycle of the cartilage in the joint. An articular cartilage defect can lead to pain, impaired function, joint catching/clicking, recurrent effusions, and swelling. If left untreated, the defect may lead to osteoarthritis [5-10]. Non-operative treatments that may relieve the symptoms of the defect include physical therapy, non-steroidal anti-inflammatory medication, and injection therapy. If non-operative treatment strategies fail to provide pain relief, surgical treatment strategies should be considered [11].
Articular cartilage injuries of the knee are common. Studies of over 30,000 knee arthroscopies have found that 63% of the arthroscopies revealed a cartilaginous lesion [12]. The average age of these patients was 43 years old, with ages ranging up to 92 years old. Of the arthroscopies that showed a cartilage lesion, almost 20% had a full thickness lesion with exposed bone. Articular cartilage defects affect a wide range of patients. Many of these patients are young and could benefit from a treatment option such as ACI.
Articular cartilage full thickness injuries are also prevalent in young active populations. One study evaluated the incidence and risk factors of full thickness chondral defects in college football athletes invited to the National Football League Scouting Combine over a three-year period [13]. The study found that 20.3% (198/975) of players had at least one full-thickness chondral defect detected by MRI. The study also found that 8.06% (79/975) had more than one defect. Treatment of this younger population provides additional complications because prostheses used in total knee replacement have a limited lifetime [14]. The use of autologous cellular material provides an opportunity for new cartilage to form that could potentially have a lasting effect to prevent the need for total knee replacement in young patient populations [15].
There is no single physical finding on examination specifically related to articular cartilage defects. Small or large effusions may be present. The motion of the knee is typically preserved, however, osteochondral fragments, a common complication of articular cartilage defects, can cause intermittent locking of the knee. Larger defects can cause repeatable catching or clicking during knee motion examination and patellar manipulation. Radiographs are important for evaluating for any malalignment and degenerative changes of the knee that may be related to the defect [11]. In addition to lateral and sunrise views, weight-bearing standing anteroposterior (AP) and 45-degree posteroanterior (PA) view radiographs are essential to evaluate chondral defects. Long-limb full-length hip-to-ankle anteroposterior views can be critical for the evaluation of knee malalignment [16].
Due to its avascular nature, articular cartilage has a low metabolic rate and a very poor regenerative capacity [17]. Therefore, articular cartilage defects typically do not heal without surgical intervention [3]. The size of the defect plays an integral role in the selection of the surgical treatment option. Previous studies have shown that there are different outcomes of the surgical procedure based on the size of the defect [18-21]. Small defects (<2-4 cm^2^) are treated most effectively with microfracture, marrow stimulation, osteochondral autograft transfer (OATS; Arthrex, Naples, FL), and edge stabilization procedures. Large defects (>2-4 cm^2^) are treated most effectively with ACL and osteochondral allograft transfer (OATS). Large defects are also typically found with concomitant pathology such as multiple defects, uncontained defects, and bone deficiency. In the presence of treatment of a chondral injury, concomitant knee pathology, such as malalignment, ligamentous instability, or meniscal deficiency, must also be addressed to improve the intraarticular environment for any cartilage repair process [3,11,22-24].
The ACL procedure has developed through multiple generations. The first generation involved the implantation of cultured autologous chondrocytes beneath a previously harvested periosteum sutured the edges of the chondral defect. This first-generation treatment, also known as PACL, had complications with periosteal graft detachment and the risk of subsequent procedures due to periosteal hypertrophy. The second generation of ACI involved the implantation of cultured autologous chondrocytes beneath an absorbable collagen membrane. This generation found a lower rate of graft hypertrophy compared to the first generation [25,26]. Further studies also found that more patients who received the second-generation ACL reported good to excellent results two years after their procedure compared to patients who received the first generation (82% compared to 55.5%) [27]. The third generation of ACL, also known as matrix-induced ACI or MACI, uses cultured autologous chondrocytes that are pre-seeded into a collagen membrane. This technique is less invasive and requires a shorter surgical time while still being an effective treatment for cartilage defects. A randomized study of over 140 patients treated with MACI versus microfracture for symptomatic chondral defects showed a significant improvement in 87.5% of MACI patients versus 68% of microfracture patients [28].
Conclusions
This case study reports the excellent long-term functional and clinical outcomes for extensive chondral defects of the medial and lateral femoral condyles treated with first-generation ACL in a then-20-year-old athlete with an 18-year follow-up. Full thickness chondral defects that are symptomatic should be considered for surgical intervention. Large defects and multiple defects are both indications for treatment with autologous chondrocytes, now with the third-generation matrix autologous chondrocyte implantation (MACI). The use of ACL in this case yielded articular cartilage regeneration that proved durable and provided pain relief and markedly improved clinical outcome for the patient at 18 years post the index procedure.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Focal cartilage defects in the knee impair quality of life as much as severe osteoarthritis: a comparison of knee injury and osteoarthritis outcome score in 4 patient categories scheduled for knee surgery Am J Sports Med Heir S Nerhus TK Røtterud JH Løken S Ekeland A Engebretsen L Arøen A 2312373820102004254610.1177/0363546509352157 · doi ↗ · pubmed ↗
- 2Time matters: knee cartilage defect expansion and high-grade lesion formation while awaiting autologous chondrocyte implantation Cartilage Pettit RJ Everhart JS Di Bartola AC Blackwell RE Flanigan DC 1802180813202110.1177/19476035211063866 PMC 880485834894761 · doi ↗ · pubmed ↗
- 3Autologous chondrocyte implantation and anteromedialization for isolated patellar articular cartilage lesions: 5- to 11-year follow-up Am J Sports Med Gillogly SD Arnold RM 9129204220142451918110.1177/0363546513519077 · doi ↗ · pubmed ↗
- 4Autologous chondrocyte implantation: a long-term follow-up Am J Sports Med Peterson L Vasiliadis HS Brittberg M Lindahl A 111711243820102018180410.1177/0363546509357915 · doi ↗ · pubmed ↗
- 5Temporal patterns of stromelysin-1, tissue inhibitor, and proteoglycan fragments in human knee joint fluid after injury to the cruciate ligament or meniscus J Orthop Res Lohmander LS Roos H Dahlberg L Hoerrner LA Lark MW 2128121994811393910.1002/jor.1100120104 · doi ↗ · pubmed ↗
- 6Increased levels of proteoglycan fragments in knee joint fluid after injury Arthritis Rheum Lohmander LS Dahlberg L Ryd L Heinegård D 14341442321989255493110.1002/anr.1780321113 · doi ↗ · pubmed ↗
- 7The long-term prognosis for severe damage to weight-bearing cartilage in the knee: a 14-year clinical and radiographic follow-up in 28 young athletes Acta Orthop Scand Messner K Maletius W 165168671996862357310.3109/17453679608994664 · doi ↗ · pubmed ↗
- 8Degradation of cartilage type II collagen precedes the onset of osteoarthritis following anterior cruciate ligament rupture Arthritis Rheum Price JS Till SH Bickerstaff DR Bayliss MT Hollander AP 239023984219991055503510.1002/1529-0131(199911)42:11<2390::AID-ANR 18>3.0.CO;2-9 · doi ↗ · pubmed ↗