Pulmonary Endobronchial Hamartoma Presenting With Post-obstructive Pneumonia
Diane S Habib, Pushan Jani, Bihong Zhao, Elakiya Anjali Jayaraman, Ramesh Kesavan

TL;DR
This paper reports a rare case of a lung tumor causing airway blockage and repeated lung infections.
Contribution
The novelty is presenting a rare endobronchial hamartoma case with post-obstructive pneumonia.
Findings
Endobronchial hamartomas can cause airway obstruction.
Such tumors may lead to recurrent post-obstructive pneumonia.
Abstract
Pulmonary hamartomas (PH) are rare but are the most common benign tumors found in the lungs. They are slow-growing and are usually found incidentally on chest imaging during the sixth decade of life. Approximately 10% of pulmonary hamartomas are endobronchial. Rarely, pulmonary hamartomas can cause a spectrum of pulmonary symptoms depending on their size and location. We present a case of endobronchial hamartoma causing airway obstruction and recurrent post-obstructive pneumonia.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
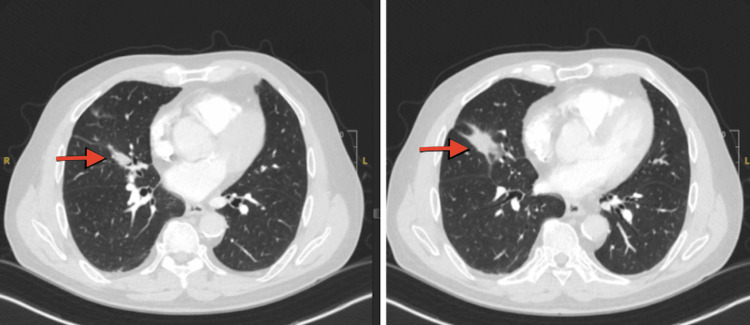 Figure 1
Figure 1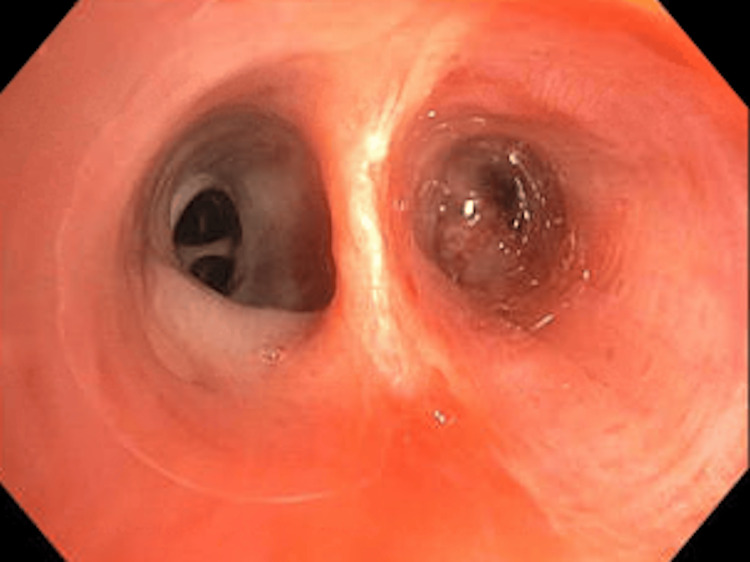 Figure 2
Figure 2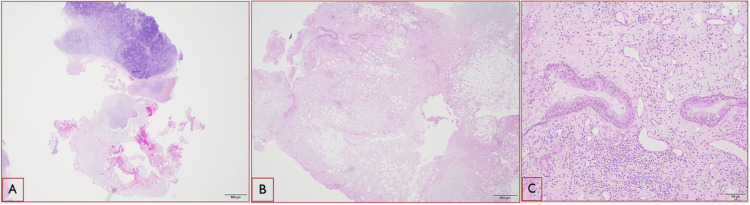 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTracheal and airway disorders · Medical Imaging and Pathology Studies · Tumors and Oncological Cases
Introduction
Endobronchial tumors are difficult to diagnose and rare. Most of the endobronchial lesions are malignant with around 11% of the lesions being benign [1]. Benign endobronchial lesions are slow-growing and present with vague symptoms such as chronic cough, wheezing, and chest pain [2]. Radiographic features are vague, making them a diagnostic challenge. Features include atelectasis, recurrent pneumonia, and bronchiectasis [3,4]. Various etiologies of benign endobronchial lesions such as anthracosis, tuberculosis, sarcoidosis, aspergillosis, hamartoma, lipoma, adenoma, and papilloma have been reported [1,2]. Approximately 22% of benign lesions present with airway obstruction, defined as greater than 50% occlusion [1]. Flexible bronchoscopy plays an important role in evaluating these endobronchial lesions and obtaining a pathologic diagnosis [5]. We present a case of endobronchial hamartoma causing airway obstruction and recurrent post-obstructive pneumonia.
Case presentation
A 71-year-old male with a past medical history of hypothyroidism, chronic obstructive lung disease, and tonsillar cancer, who had received chemotherapy and radiation five years ago, presented to the emergency room with two weeks of dry cough, dyspnea, and minimal blood-tinged sputum. The patient had previously been treated for community-acquired pneumonia as an outpatient, but his symptoms did not resolve despite treatment with a course of azithromycin, cefdinir, and prednisone prescribed one week prior to this visit. He had 20 pack-year smoking history in the past but quit five years ago. His oxygen saturation was 96% on room air, and his vital signs were otherwise stable. His lung examination was clear. His WBC count was 11000/microliter with 91% neutrophilia. A CT scan of the chest without contrast (Figure 1) revealed an endobronchial lesion in the right middle lobe (RML) segmental bronchus with a nodular appearance measuring 13 mm × 4 mm with punctate calcification. Findings were suspicious for an endobronchial lesion with post-obstructive lung collapse. During the bronchoscopy, a completely obstructing endobronchial mass was found proximally at the orifice of the lateral segment of the RML (Figure 2). Bronchoalveolar lavage (BAL) and endobronchial brushing were obtained from that segment, as well as endobronchial biopsies under fluoroscopy guidance. Pathology was consistent with a pulmonary hamartoma (PH) (Figure 3). The patient was successfully treated with debulking of the tumor using cryotherapy and argon plasma coagulation. Following debulking, post-obstructive purulent material was therapeutically aspirated, and the distal airway appeared patent.
CT of the chest images showing evidence of right middle lobe endobronchial lesion (red arrowheads) resulting in focal post-obstructive collapse
Endobronchial tumor in the right middle lobe lateral segmental bronchus
Pathology slides(A) Mature cartilaginous tissue with mild and focal calcification (hematoxylin and eosin {H&E}: ×20). (B) A mixture of different types of tissue and cells including adipose, fibrotic, and glandular tissues (H&E: ×20). (C) The higher power of the glandular tissue with respiratory-type epithelium (H&E: ×100)
Discussion
Benign endobronchial tumors are rare and difficult to diagnose given their vague clinical and radiographic presentation [2]. PH are the most common benign tumor found in the lungs [6]. PH were originally described in 1904 by the German pathologist Eugen Albrecht [5]. They are composed of mature mesenchymal tissue commonly found in the lung that develops without preserving its architecture [7]. Given their slow growth, PH are usually found incidentally on chest imaging [5,8]. Endobronchial hamartomas are rare. Approximately 10% of PH are endobronchial, most of them being peripherally located [9]. Endobronchial hamartomas have a higher prevalence in male smokers in their fifth and sixth decade [10]. Rarely, PH can cause a spectrum of pulmonary symptoms depending on its size and location [11]. PH can present with a persistent cough, hemoptysis, pneumonia, pneumothorax, and even airway obstruction [11,12]. Endobronchial hamartomas can lead to recurrent pneumonia and bronchiectasis [13]. Endobronchial hamartomas can be misdiagnosed as asthma [14]. Patients with pulmonary hamartoma have an increased risk of lung cancer [5]. Intervention is necessary when the pulmonary hamartoma expands or becomes symptomatic as in our patient [15]. Treatment should be considered for asymptomatic patients since they can develop obstructive pneumonia and also potentially increased risk for malignancy [5,16,17]. Airway inspection with flexible bronchoscopy is essential to evaluate the airway and obtain a pathologic diagnosis [2]. Tumor debridement using techniques such as argon plasma coagulation, cryotherapy, and mechanical debulking using rigid or flexible bronchoscopy is being used and has shown to be well tolerated with no residual or recurrent disease on follow-up [18,19].
Conclusions
Endobronchial lesions can cause vague symptoms and radiological findings. High clinical suspicion and careful radiological and airway evaluation with a bronchoscope are necessary to clinch the diagnosis. The majority of endobronchial lesions are malignant. Rarely, these lesions are benign. However, despite not being cancerous, these benign endobronchial lesions can cause various complications such as post-obstructive pneumonia, bronchiectasis, and a potential risk of malignancy. As discussed in our case, endobronchial hamartomas, even though rare, can lead to potential complications and warrant further management with advanced bronchoscopy techniques.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Incidence, etiology, and clinicopathologic features of endobronchial benign lesions: a 10-year consecutive retrospective study J Bronchology Interv Pulmonol Marchioni A Casalini E Andreani A 1181242520182934625010.1097/LBR.0000000000000460 · doi ↗ · pubmed ↗
- 2Benign endobronchial tumors: a clinicopathologic review Front Surg Insler JE Seder CW Furlan K Mir F Reddy VB Gattuso P 644656820213374818310.3389/fsurg.2021.644656 PMC 7973360 · doi ↗ · pubmed ↗
- 3Pathological and radiological correlation of endobronchial neoplasms: part II, malignant tumors Ann Diagn Pathol Wilson RW Frazier AA 315421998 https://www.sciencedirect.com/science/article/abs/pii/S 1092913498800336984572110.1016/s 1092-9134(98)80033-6 · doi ↗ · pubmed ↗
- 4Pathological and radiological correlation of endobronchial neoplasms: part I, benign tumors Ann Diagn Pathol Wilson RW Kirejczyk W 314611997 https://www.sciencedirect.com/science/article/pii/S 109291349780007 X 986982410.1016/s 1092-9134(97)80007-x · doi ↗ · pubmed ↗
- 5Symptomatic pulmonary hamartoma Cureus Shukla I Stead TS Aleksandrovskiy I Rodriguez V Ganti L 013202110.7759/cureus.18230 PMC 852607434692355 · doi ↗ · pubmed ↗
- 6Hamartomas and other tumor-like malformations of the lungs and heart Semin Diagn Pathol Wick MR 210362019 https://doi.org/10.1053/j.semdp.2018.11.0023047346210.1053/j.semdp.2018.11.002 · doi ↗ · pubmed ↗
- 7[Pulmonary hamartoma] (Article in Portuguese)Acta Med Port Matos R Carvalho L 165168152002 https://pubmed.ncbi.nlm.nih.gov/12379992/12379992 · pubmed ↗
- 8Pulmonary hamartoma J Chin Med Assoc Lien YC Hsu HS Li WY 2126672004 https://pubmed.ncbi.nlm.nih.gov/15077886/15077886 · pubmed ↗