Obscure Small Bowel Bleeding Related to a Ventral Hernioplasty Mesh Perforation Visualized With Video Capsule Endoscopy
Mei Yang, Biruk Beyene, Elie Chahla

TL;DR
A 76-year-old woman with a history of hernioplasty experienced small bowel bleeding due to mesh erosion, diagnosed using video capsule endoscopy.
Contribution
Highlights the rare but important cause of obscure GI bleeding related to mesh hernioplasty and the utility of video capsule endoscopy in diagnosis.
Findings
Mesh erosion into the small bowel caused transfusion-dependent GI bleeding.
Video capsule endoscopy identified the source of bleeding after prior endoscopies failed.
Early differential diagnosis is crucial for patients with obscure GI bleeding and a history of hernioplasty.
Abstract
We report a case of a 76-year-old female presenting with intermittent obscure gastrointestinal (GI) bleeding originating from the small intestine secondary to a delayed complication related to mesh hernioplasty. The mesh was eroding into the small bowel causing intermittent transfusion-dependent GI bleeding. Multiple upper and lower endoscopic investigations were sought over the last two years, but they were noncontributory. Finally, video capsule endoscopy (VCE) revealed mesh invasion into the small bowel wall associated with bleeding. This case emphasizes the significance of an early sufficient differential diagnosis in patients with obscure GI bleeding. Meanwhile, being cognizant of rare causes of GI bleeding in patients who have had hernioplasty is very important.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
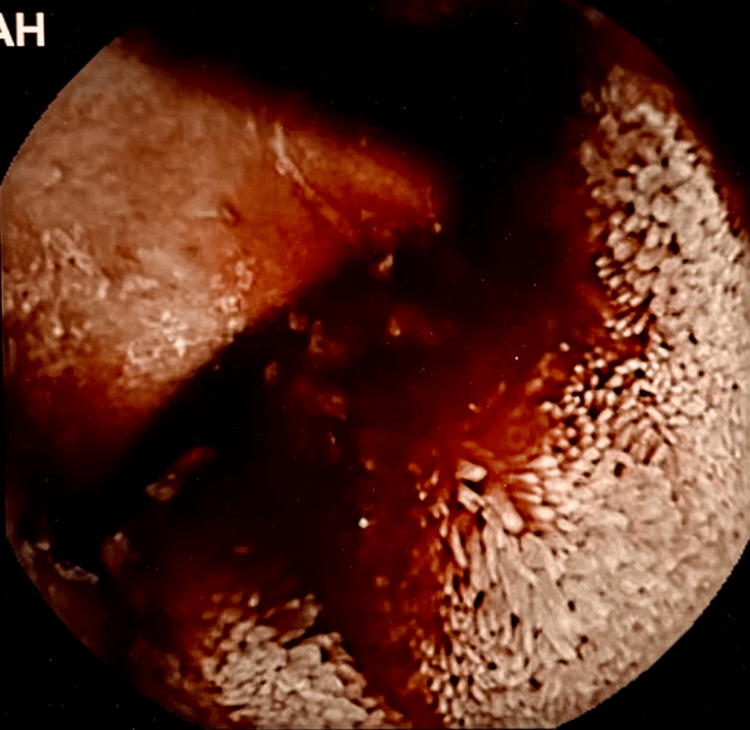 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Gastrointestinal Bleeding Diagnosis and Treatment · Gastric Cancer Management and Outcomes
Introduction
Surgical hernioplasty is a very common procedure that treats different types of hernias like ventral hernias [1,2]. A mesh device is a surgical technique used to repair ventral hernias, which may cause possible serious complications including mesh migration, or improper placement of the mesh [3]. Small bowel obstruction, perforations, erosions, fistulas, and volvulus are complications after this type of hernia repair and have been attributed to mesh migration [2-4]. Imaging procedures, including endoscopy, colonoscopy, or abdominal computed tomography, are useful to locate or diagnose this disease [1,4]. Literature research revealed only one published case of obscure gastrointestinal (GI) bleeding due to mesh migration from ventral hernioplasty in the United States [1].
Case presentation
A 76-year-old Caucasian female with a significant past medical history of obesity, Insulin-dependent diabetes mellitus, hypertension, dyslipidemia, chronic obstructive pulmonary disease (COPD), early-stage esophageal adenocarcinoma status post concurrent chemotherapy and radiation therapy with good response, complicated diverticulitis status post left hemicolectomy, pancreatitis, chronic blood loss anemia, open cholecystectomy with incisional hernia repair and persistent large ventral hernia, recurrent hospitalizations for anemia and hematochezia. Two times esophagogastroduodenoscopies (EGDs) and a one-time colonoscopy as part of her anemia workup were done recently. EGD showed the esophageal cancer was in remission, without any active bleeding. A colonoscopy revealed a benign-appearing nonobstructing inflammatory proximal rectal anastomotic stricture which was less likely as an etiology of her anemia. She was hemodynamically stable, and her hemoglobin was noted at 7.6 g/dL down from a baseline of 9 g/dL in the last year. Recent upper and lower endoscopies were just done several weeks ago, which showed no clear source of bleeding. A small bowel bleeding source needed to be excluded this time and a video capsule endoscopy (VCE) followed. This revealed evidence of a foreign body compatible with mesh perforating the lumen of the mid jejunum with associated small bowel bleeding (Figures 1, 2). Abdominal CT with intravenous contrast was done and failed to reveal the presence of perforation. Since it was not possible to extract the mesh or correct the bleeding endoscopically, she was transfused a total of three units of blood with stabilization of her hemoglobin. We consulted the surgical services. When presented with the potential complications linked to the surgery given her significant comorbidities, the patient refused additional interventions. She was eventually discharged home with a close hematology follow-up. She is still doing well with scheduled iron infusions and blood transfusions on an as-needed basis.
Video capsule endoscopy showing small bowel intraluminal bleeding.
Video capsule endoscopy showing intraluminal coiled mesh eroding through wall of the jejunum into lumen.
Discussion
Recent literature reported that ventral hernia repair has various complications with the mesh technique, especially bowel perforation, peritonitis, and bowel obstruction from mesh migration [4,5]. The case we described here represents the second-ever published case of a ventral hernia mesh migration into the mid jejunum visualized with VCE in a patient presenting with melena [1].
VCE is a well-established diagnostic method for further small bowel investigation in obscure GI bleeds, according to endoscopic recommendations released by the American Society for Gastrointestinal Endoscopic. A VCE is a procedure in which a patient needs to swallow a capsule with a small wireless camera inside to take thousands of pictures as it passes through the small intestine. Compared to Push enteroscopy and CT angiography, VCE offers a higher yield for identifying bleeding sources and clinically relevant lesions in the small intestine. An uncommon complication of VCE is capsule retention (1.4%), which can cause bleeding, infection, or obstruction [6,7]. If capsule retention happens, close monitoring was suggested because capsule retention generally can resolve spontaneously by itself. However, if the conservative method fails, then a surgical approach would be the next step.
Our team determined that VCE was the best course of action because the patient had recurrent episodes of obscure GI bleeding after unrevealing upper endoscopy and colonoscopy. Thus, another essential diagnosis method VCE is very significant to find the bleeding source and etiology [7]. Meanwhile, the mesh is a large prosthetic hernia repair device that cannot be removed endoscopically without major complications, and surgery would be the next step consideration if the patient is unstable after transfusion. But, in our case, the elderly patient has many complicated medical histories and is not a good candidate for surgery.
Conclusions
Mesh migration, a well-known side effect of surgical hernioplasty, frequently results in perforation or small bowel obstruction. GI bleeding from mesh migration is an uncommon and rare complication. This case highlights the significance of a thorough diagnostic examination in patients with obscure GI bleeding as well as the need to be aware of uncommon causes of GI bleeding in patients who have had hernioplasty.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Obscure overt gastrointestinal bleeding secondary to ventral hernioplasty mesh small bowel perforation visualized with video capsule endoscopy ACG Case Rep J Mendez-Ishizaki Y Parra JL 03201610.14309/crj.2016.140PMC 517193628008400 · doi ↗ · pubmed ↗
- 2Mesh migration following repair of inguinal hernia: a case report and review of literature Hernia Agrawal A Avill R 79821020061625870510.1007/s 10029-005-0024-8 · doi ↗ · pubmed ↗
- 3Complications associated with the plug-and-patch method of inguinal herniorrhaphy Hernia Le Blanc KA 135138520011175979810.1007/s 100290100027 · doi ↗ · pubmed ↗
- 4Mesh plug migration into scrotum: a new complication of hernia repair Int Surg Dieter RA Jr 5759841999 https://europepmc.org/article/med/1042102010421020 · pubmed ↗
- 5Bowel complications after prolene hernia system (PHS) repair: a case report and review of the literature Hernia Lo DJ Bilimoria KY Pugh CM 4374401220081823600010.1007/s 10029-008-0338-4 · doi ↗ · pubmed ↗
- 6Wireless capsule endoscopy Gastrointest Endosc Wang A Banerjee S Barth BA 8058157820132411950910.1016/j.gie.2013.06.026 · doi ↗ · pubmed ↗
- 7The role of endoscopy in the management of obscure GI bleeding Gastrointest Endosc Fisher L Lee Krinsky M Anderson MA 4714797220102080128510.1016/j.gie.2010.04.032 · doi ↗ · pubmed ↗