Development and validation of a community acquired sepsis-worsening score in the adult emergency department: a prospective cohort: the CASC score
François Saget, Adel Maamar, Maxime Esvan, Arnaud Gacouin, Jacques Bouget, Vincent Levrel, Jean-Marc Tadié, Louis Soulat, Paul Georges Reuter, Nicolas Peschanski, Bruno Laviolle

TL;DR
This study developed a new score to quickly identify patients with community-acquired sepsis at risk of worsening in the emergency department.
Contribution
The novel CASC score outperforms existing tools like qSOFA and NEWS-2 in predicting sepsis worsening.
Findings
The CASC score has an AUC of 0.85, showing strong discrimination for sepsis worsening.
A cut-off of 26 provides 88% sensitivity and 95% negative predictive value.
The CASC score outperformed qSOFA and NEWS-2 in predicting clinical deterioration.
Abstract
Sepsis is a leading cause of death and serious illness that requires early recognition and therapeutic management to improve survival. The quick-SOFA score helps in its recognition, but its diagnostic performance is insufficient. To develop a score that can rapidly identify a community acquired septic situation at risk of clinical complications in patients consulting the emergency department (ED). We conducted a monocentric, prospective cohort study in the emergency department of a university hospital between March 2016 and August 2018 (NCT03280992). All patients admitted to the emergency department for a suspicion of a community-acquired infection were included. Predictor variables of progression to septic shock or death within the first 90 days were selected using backward stepwise multivariable logistic regression to develop a clinical score. Receiver operating characteristic (ROC)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
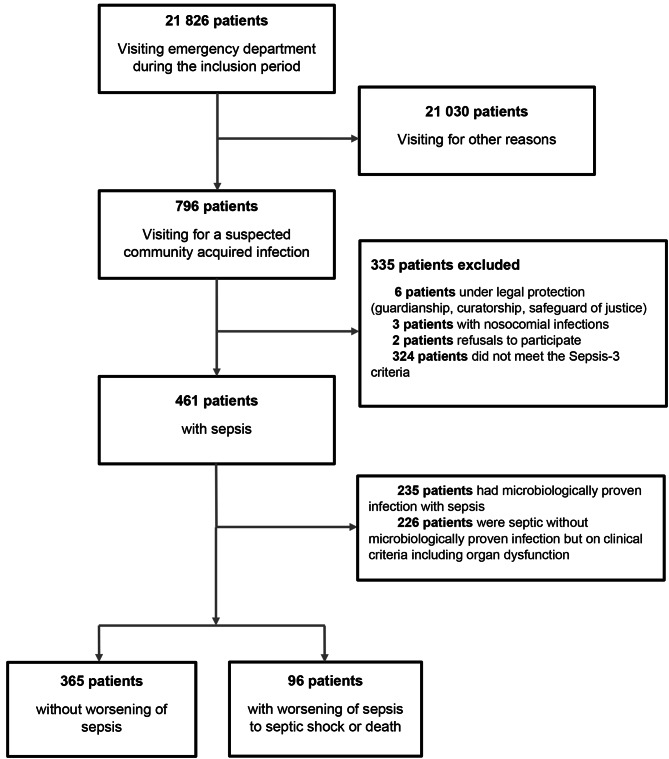 Figure 1
Figure 1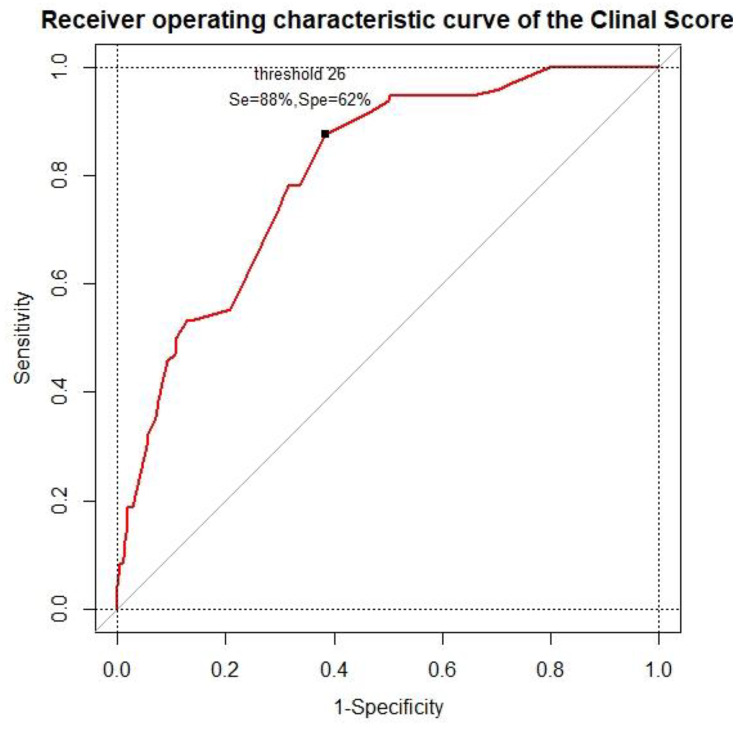 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBiblical Studies and Interpretation · Religion, Society, and Development · Development, Ethics, and Society
Introduction
Sepsis is one of the leading causes of death and serious illness worldwide. After a long period of increasing incidence, sepsis is now actually decreasing, but mortality remains high [1]. It is defined as “life-threatening organ dysfunction caused by a dysregulated host response to infection“ [2]. Its early recognition and treatment are key parameters for improving overall survival, with an estimated in-hospital mortality over 27% [3]. In fact, the World Health Organization (WHO) made this a global health priority in 2017 to encourage research to improve the prevention, diagnosis and management of sepsis [4]. Early identification of patients suspected of having community-acquired sepsis who are at risk of worsening is therefore essential to improve these outcomes.
New definitions of sepsis and septic shock were published in 2016, abandoning the Systemic Inflammatory Response Syndrome (SIRS) criteria in favor of the Sequential Organ Failure Assessment (SOFA) score [2]. This score was validated in critically ill patients hospitalized in intensive care units (ICUs) and requires biological variables that are not rapidly available when patients arrive in the emergency department. Due to the difficulty of using this score outside the ICU, the Sepsis-3 working group proposed a simplified score, the quick SOFA (qSOFA), based on three clinical variables without any laboratory tests, and can be performed quickly and easily in the ward and emergency departments [2]. Since the creation of this score, many studies have questioned its performance. This score has an acceptable specificity but lacks sensitivity to predict mortality in in Emergency Department [5–9]. This performance may have deleterious consequences in the management of emergencies, leading to a delay in the implementation of therapies and consequently, an impact on morbidity and mortality [10, 11]. The latest recommendations of the Surviving Sepsis Campaign advise against its use as the sole screening tool for sepsis and septic shock [12].
Thus, unlike other critical illnesses, such as stroke, which have the National Institute of Health Stroke Scale (NOS) clinical score is used to assess patient prognosis and estimate severity [13], there is currently no reproducible and reliable consensus prognostic tool for sepsis in the emergency department.
Therefore, the aim of our study is to developed a prognostic clinical score that can rapidly identify a community acquired septic situation at risk of aggravation in patients consulting the emergency department.
Methods
Design and setting
The Community Acquired Sepsis Cohort (CASC) was a prospective, monocentric cohort study in the adult emergency department of Rennes University Hospital (NCT03280992). We included patients who visited our emergency department from March 2016 to August 2018 for a suspected community-acquired infection. The study was approved by the Rennes University Hospital’s ethical committee (no.16.15) and written informed consent was obtained from all subjects participating in the study. We followed the Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD) reporting guidelines [14].
Selection of participants, data collection and endpoints
The CASC cohort included patients ≥ 18 years hospitalized in the emergency department with a clinical suspicion of infection diagnosed by emergency physicians. In our study, we selected patients from the CASC cohort for whom infection was either proven, compatible on the basis of the clinical context or seen by radiological findings. Two experts (FS and JB) reviewed all the data and determined whether the acute presentation at the emergency department was related to infection by analyzing the following parameters: (i) positive culture of blood samples, respiratory samples, cytobacterial examination of urine, lumbar puncture, ascites puncture, and joint puncture; we also considered positive tests, such as specific urinary antigen test for Legionella pneumophilae or Streptococcus pneumoniae, polymerase chain reaction (PCR) for Mycoplasma pneumoniae, Chlamydophila pneumoniae and Chlamydia psittaci, and reverse transcriptase PCR for respiratory viruses; (ii) clinical context; and (iii) radiological findings. Moreover, the two experts assessed whether the infection was community acquired by analyzing if the patients were hospitalized in the ward or ICU within the three previous months.
We excluded patients who provided written opposition to the collection of their data, pregnant women and adults under legal protection (safeguard of justice, curatorship, guardianship) or deprived of freedom, with septic shock at admission, patients who were transferred from a different hospital prior to their admission with sepsis, and if the microbiological samples were collected before or after the ED stay to avoid including patients who did not meet the inclusion criteria simultaneously.
For each patient, clinical (including vital signs, medical history and treatments), and demographic (including place of residence) data were collected at admission and during emergency room management. The initial symptoms and medical management including the use of crystalloids or the need for oxygenation and ventilation support (nasal cannula, oxygen mask, non-invasive ventilation, mechanical ventilation) were recorded.
Sepsis and septic shock were defined according to the Sepsis-3 Definition [2]. Finally, the vital status was collected at 90 days, by telephone contact if necessary. If the patient did not respond, the attending physician was contacted as well as the town hall in order to have the exact date of death.
The primary endpoint was worsening of sepsis, defined as a composite endpoint of progression to septic shock or death within the first 90 days.
Statistical analysis
Statistical analyses were performed using R 4.1.3 (R Foundation for Statistical Computing, Vienna, Austria), and p-values of less than 0.05 were considered significant.
Normally distributed continuous variables are presented as the means (standard deviations [SDs]), whereas non-normally distributed data are presented as medians (Interquartile ranges [IQRs]). The characteristics of patients who developed worsening of sepsis and those who did not were compared using Student’s t test or the Mann-Whitney test when appropriate for continuous variables, and the χ2 test or Fisher’s exact test when appropriate for categorical variables. Quantitative variables were recoded into categorical variables using the locally estimated scatterplot smoothing (LOESS) regression method [15] according to the points of inflection of the curve into two or three classes. Missing data were handled using multiple imputation [16]. Missing data at random were assumed. A total of 5 imputed datasets were generated, using 10 iterations. The accuracy and acceptability of the imputed data were evaluated with distribution plots.
To identify risk factors independently associated with worsening of sepsis, variables achieving a p-value < 0.1 between the two groups were entered into a backward stepwise logistic regression model. The results are expressed as odds ratios (ORs) with 95% confidence intervals (CIs). (Supplementary Table 1).
As previously described [17], the number of points assigned to each variable from the multivariable model corresponds to the value of the β coefficient of the model multiplied by 10 and rounded to the nearest integer. The score was then calculated for each patient, with mean scores for each group. A ROC curve was produced for each score and thresholds were defined to maximize sensitivity and specificity.
Predictive performance was expressed as discrimination (area under curve [AUC]) and calibration using the Hosmer-Lemeshow goodness-of-fit test, absence of collinearity between variables, and standardized deviance residual analysis. We also calculated the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). The developed model was internally validated using bootstrap resampling [18]. Optimism-corrected performance was calculated as follows: optimism-corrected performance = apparent performance–optimism. We compared the results of our score with the qSOFA [2] and NEWS-2 [19]. Finally, we performed a sensitivity analysis of the application of the score on the complete cases.
Results
Sample characteristics
During the study period, 21,826 patients consulted the emergency department of the University Hospital of Rennes (15,344 between 02/03/2016 and 16/06/2016, 6482 from 16/07/2018 and 27/08/2018), 796 of whom were included in our analysis. Among these patients with suspected community acquired infection, 461 met the inclusion criteria of our study with a sepsis. Among the 461 septic patients, 96 (21%) progressed to septic shock or death at D90. (Fig. 1).
Fig. 1. Flow diagram of study
Population was composed by 54% male with a median age of 72 [54–84] years. The place of residence prior admission to the emergency room was mostly home and 83 (18%) patients were discharged from a retirement home or a long-term care unit. Septic patients presenting to the emergency department had mainly respiratory symptoms (53%). The characteristics of these patients compared to those who did not progress to septic shock or death are presented in Table 1.
Table 1. Baseline clinical characteristics of study participantsCharacteristicsOccurrence of septic shock or death at Day 90p-valueNo (N = 365)Yes (N = 96)Age, median [IQR], y70 [48–82]81.5 [67.75- 89]P < .001 Sex, No. (%) Female181 (50)32 (33)0.006 Male184 (50)64 (67) Place of residence, No. (%) Home318 (87)60 (63)P < .001 Nursing home or long-term care unit47 (13)36 (37) Physiological parameters Systolic blood pressure, mean (SD), mmHg134 (27)120 (29)P < .001 Diastolic blood pressure, mean (SD), mmHg77 (16)72 (17)0.008 Mean blood pressure, mean (SD), mmHg96 (20)89 (21)0.001 Heart rate, mean (SD), bpm100 (20)104 (22)0.138 Temperature, median [IQR], °C38.2 [37.3–38.9]37.7 [36.8–38.6]0.001 Respiratory rate, median [IQR], breaths/min26 [20–32]28 [24–33]0.024 Glasgow coma scale, median [IQR],15 [15–15]15 [14–15]P < .001 Medical history Active cancer, No. (%)54 (15)31 (32)P < .001 Organ transplant, No. (%)6 (2)1 (1)P > .99 Chronic inflammatory disease under immunosuppressant, No. (%)11 (3)5 (5)0.344 Chronic viral infection treated, No. (%)8 (2)3 (3)0.705 Hypertension, No. (%)146 (40)46 (48)0.165 Diabetes, No. (%)61 (17)18 (19)0.649 Dyslipidemia, No. (%)81 (22)25 (26.0)0.417 Active smoking, No. (%)44 (12)10 (10)0.725 Alcoholism, No. (%)21 (6)9 ( 9)0.242 Heart failure, No. (%)29 (8)12 (13)0.163 Coronary heart disease, No. (%)39 (11)9 ( 9)0.852 Arterial disease, No. (%)36 (10)15 (16)0.142 Cerebrovascular accident, No. (%)37 (10)15 (16)0.147 Heart valve surgery, No. (%)9 (3)3 ( 3)0.720 Chronic obstructive pulmonary disease, No. (%)49 (13)15 (16)0.619 Chronic liver failure, No. (%)4 (1)2 (2)0.609 Chronic renal failure, No. (%)17 (5)13 (14)0.004 Disturbance of the known cognitive functions, No. (%)31 (9)31 (32)P < .001 Splenectomy, No. (%)3 (1)1 (1)P > .99 Beta-blocker therapy, No. (%)72 (20)15 (16)0.463 ACE blockers or, ARB, No. (%)74 (20)17 (18)0.666 Symptoms on admission Respiratory, No. (%)175 (48)69 (72)P < .001 Abdominal, No. (%)97 (27)17 (18)0.097 Genital or urinary, No. (%)81 (22)16 (17)0.298 Cutaneous, No. (%)41 (11)6 (6)0.213 Articular, No. (%)21 (6)3 (3)0.439 Neuromeningeal, No. (%)50 (14)11 (12)0.684 Management Room air ventilation, No. (%)216 (59)18 (19)P < .001 Oxygenation and/or ventilation support, No. (%)149 (41)78 (81)P < .001 Use of crystalloids, No. (%)42 (12)29 (30)P < .001Data are median [interquartile range] or mean (standard deviation) for continuous variables and number (%) for categorical variablesDefinition of abbreviations: ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blockers
Clinical model development and validation
The final multivariable model retained eight predictors to establish the clinical score: sex, place of residence, Glasgow coma score, presence of cancer, use of crystalloids, oxygenation or ventilation support, presence of known cognitive impairment, and temperature. The regression coefficients and odds ratios of the final model are shown in Supplementary Table 2.
The prognostic performance of the clinical model is presented in Supplementary Table 3. The AUROC of the clinical model for predicting sepsis worsening was 0.85 (95% CI, 0.81–0.89) (Supplementary Fig. 1). The clinical model had a sensitivity of 0.81 (95% CI, 0.76–0.91), a specificity of 0.75 (95% CI, 0.70–0.79), and a negative predictive value was 0.94 (95% CI, 0.90–0.96) for predicting sepsis worsening. The Hosmer-Lemeshow test showed a p-value of 0.23 indicating a good calibration. The optimism corrected performance found by the bootstrap method (1000 iterations) was 0.84 indicating acceptable discrimination for internal validation.
Clinical score
Table 2 shows the respective points attributed to each category of the clinical variable used to calculate the score. The points assigned to each variable vary from 0 to 16. Thus, the clinical score ranges from 0 to 90 (a higher score reflects a more severe prognosis). The median score was 24 [10–34] the group without worsening sepsis and 41 [32–50] in the group with worsening sepsis. A cut-off value of 26 was identified from the ROC curve as the best compromise between sensitivity (0.88, 95% CI 0.79–0.93) and specificity (0.62, 95% CI 0.57–0.67), while maintaining an excellent negative predictive value (0.95, 95% CI 0.91–0.97). (Fig. 2). The area under the ROC curve for CASC score was 0.85 (95% CI, 0.81–0.89) versus 0.73 (95% CI, 0.68–0.78) for qSOFA and 0.66 (95% CI, 0.60–0.72) for NEWS-2. We obtained a sensitivity for the qSOFA of 0.33 (95% CI, 0.24–0.43), and 0.49 (95% CI, 0.39–0.59) for the NEWS-2. (Supplementary Fig. 2).
Table 2. Clinical score to predict worsening of sepsis to septic shock or death at Day 90VariablesPoints089101516SexFemaleMalePlace of residenceHomeNursing homeTemperature≥ 38 °C< 38 °CGlasgow ScoreNormal< 15Active cancerNoYesCognitive impairmentNoYesOxygenation and/or ventilation supportAmbiant airYesUse of crystalloids fluidsNoYes
Fig. 2. Clinical score receiver operating characteristic curve for predicting sepsis worsening
Sensitivity analysis
A sensitivity analysis was performed on 407 complete cases. Eighty-six of these patients presented septic shock or death at Day 90. Using our clinical score on complete cases found 76 patients were considered true positives and 196 patients were considered as true negatives. The performance of the score in the sensitivity analysis is shown in Table 3.
Table 3. Diagnostic performance of the clinical score with threshold of 26 for prediction of sepsis worseningFor Prediction of worsening sepsisWhole populationSensitivity analysis populationSensitivity % (95% CI)0.88 (0.79–0.93)0.88 (0.80–0.94)Specificity % (95% CI)0.62 (0.57–0.67)0.61 (0.55–0.66)Predictive value (95% CI) Positive0.38 (0.31–0.44)0.38 (0.31–0.45) Negative0.95 (0.91–0.97)0.95 (0.91–0.98)Likelihood ratio (95% CI) Positive2.30 (1.98–2.67)2.27 (1.94–2.66) Negative0.20 (0.12–0.34)0.19 (0.11–0.34)Definition of abbreviations: CI, confidence interval
Discussion
In this study, we developed a new and easy to use clinical prediction score that presented a high accuracy to early identify community acquired septic patients at risk of deterioration into septic shock or death at 90 days. Its high negative predictive value is important for diseases such as sepsis where the risk of being undetected can lead to serious consequences. Indeed, delays in recognition of sepsis and administration of antibiotics are both associated with increased hospital mortality [11], especially after three hours of delay in the administration of antibiotics [20]. Consequently, our score could be used at the time of admission, using only clinical features, and might allow simple and rapid identification of patients at risk of deterioration.
While many severity scores currently in use are designed for critically ill patients and focus on predicting mortality, our score was specifically developed as a prediction tool [17, 21]. It presented a high sensitivity (88%) and negative predictive value (95%) to identify septic patients admitted to the emergency department at risk of worsening, superior to the qSOFA and NEWS-2 scores in our study which had sensitivities of 0.33 (95% CI, 0.24–0.43), and 0.49 (95% CI, 0.39–0.59) respectively, and negative predictive values of 0.84 (95% CI, 0.80–0.88) and 0.85 (95% CI, 0.82–0.89). These patients can subsequently be rapidly diagnosed and treated accordingly. Moreover, our score was created from an emergency population on routinely clinical data collected in the first hours of admission in an emergency department. Consequently, our score is not designed to replace the SOFA score, but could be complementary.
Interestingly, we found that fever was not associated with possible degradation. This may seem surprising in a septic context but could be explained by several points. First, 60% of adult septic patients are elderly, and thus are undergoing immunosenescence, which can lead to a decrease in cytokine production, alterations in the function and expression of Toll Like Receptors, and thymic involution [22]. This immunosenescence could explain why in 30–50% of cases, the elderly septic population does not present with fever [23]. Second, the fever of septic patients in the emergency room at admission may have been masked by the use of antipyretics. As fever helps in the recognition of sepsis and its early management, its absence probably delayed the recognition and, consequently, treatment initiation management explaining the severity of these patients.
Blood pressure did not appear to be a predictor of our score, which may seem surprising given the findings in the literature. Nevertheless, we assume that the assessment of hemodynamics and therefore blood pressure is assessed by the use of crystalloids. Elements of our score are found in several other scores. For example, the presence of cognitive impairment is found in the qSOFA [2], the NEWS-2 [19] and the MEDS score [24] and the place of residence is included in the MEDS score. In contrast, we believe that two variables are more comprehensive in our score: the need for ventilatory support and the use of crystalloids. Indeed, they are found to some extent in the MEDS score with tachypnea or hypoxia, in the NEWS-2 with oxygen administration, assessment of saturation and blood pressure, and finally in the qSOFA with respiratory rate and blood pressure. As far as temperature is concerned, we explained in the discussion why being apyretic can be a real danger in the emergency department which could lead to a delayed management and underecognition. We believe that this is an important point in our study, particularly in the geriatric population [22].
One strength of our score is its simplicity. This ease of application could allow to extend its use to the regulation of the Emergency Medical Services and thus trigger an alert signal that could reduce the delay in the administration of antibiotics [25]. The main limits our study was its monocentric design and no external validation cohort was used. Nevertheless, it was decided a priori to construct the score on the whole population and not to separate the sample into a derivation and a validation cohort. We validated our score using the Boostrap resampling method, and we found with 1000 iterations a corrected area under the curve close to our initial result. Second, as we aimed to develop a clinical score that can be used by the reception team, we excluded biological parameters and all features that are not routinely collected early after the admission. Therefore, we cannot rule out that using biological features could have enhanced the accuracy of our score. Another limitation is the use of cognitive impairment in our score rather than the Glasgow score. These two variables were statistically dependent in our analysis and are strongly clinically correlated, as the presence of a severe cognitive dysfunction impairs the Glasgow score. Thus, for our analysis, we selected the one that made the best contribution to our multivariable model.
Conclusion
This study presents a simple and accurate clinical score that can rapidly identify community acquired septic patients at risk of deterioration among patients consulting the emergency department. Our score has to be validated in the future in sepsis case in general.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
Supplementary Material 3
Supplementary Material 4
Supplementary Material 5
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rudd KE Johnson SC Agesa KM Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the global burden of disease study Lancet 20203952001110.1016/S 0140-6736(19)32989-731954465 PMC 6970225 · doi ↗ · pubmed ↗
- 2Singer M Deutschman CS Seymour CW The Third International Consensus definitions for Sepsis and septic shock (Sepsis-3)JAMA 201631580110.1001/jama.2016.028726903338 PMC 4968574 · doi ↗ · pubmed ↗
- 3Fleischmann-Struzek C Mellhammar L Rose N Incidence and mortality of hospital- and ICU-treated sepsis: results from an updated and expanded systematic review and meta-analysis Intensive Care Med 20204615526210.1007/s 00134-020-06151-x 32572531 PMC 7381468 · doi ↗ · pubmed ↗
- 4Reinhart K Daniels R Kissoon N Machado FR Schachter RD Finfer S Recognizing Sepsis as a Global Health Priority — a WHO Resolution N Engl J Med 2017377414710.1056/NEJ Mp 170717028658587 · doi ↗ · pubmed ↗
- 5Tusgul S Carron PN Yersin B Calandra T Dami F Low sensitivity of q SOFA, SIRS criteria and sepsis definition to identify infected patients at risk of complication in the prehospital setting and at the emergency department triage Scand J Trauma Resusc Emerg Med 20172510810.1186/s 13049-017-0449-y 29100549 PMC 5670696 · doi ↗ · pubmed ↗
- 6Serafim R Gomes JA Salluh JPóvoa PA comparison of the Quick-SOFA and systemic inflammatory response syndrome criteria for the diagnosis of Sepsis and Prediction of Mortality Chest 20181536465510.1016/j.chest.2017.12.01529289687 · doi ↗ · pubmed ↗
- 7Brink A Alsma J Verdonschot RJCG Predicting mortality in patients with suspected sepsis at the Emergency Department; a retrospective cohort study comparing q SOFA, SIRS and National Early warning score. Lopez-Delgado JC, éditeur P Lo S ONE 201914 e 021113310.1371/journal.pone.021113330682104 PMC 6347138 · doi ↗ · pubmed ↗
- 8Song JU Sin CK Park HK Shim SR Lee J Performance of the quick sequential (sepsis-related) organ failure Assessment score as a prognostic tool in infected patients outside the intensive care unit: a systematic review and meta-analysis Crit Care 2018222810.1186/s 13054-018-1952-x 29409518 PMC 5802050 · doi ↗ · pubmed ↗