The Prevalence of Domestic Verbal Abuse in Pregnant Women in a Semi-urban Area
Pankaj Salvi, Sneha Aramandla, Vidya Gaikwad, Swati Ghonge

TL;DR
This study finds that 37% of pregnant women in a semi-urban area experience verbal abuse, with higher rates among younger and unemployed women, and those with previous female children.
Contribution
The study uniquely examines the link between previous female children and domestic verbal abuse in pregnant women.
Findings
37% of pregnant women experienced domestic verbal abuse during pregnancy.
Women aged 18-23 and those with previous female children showed significantly higher rates of verbal abuse.
Pregnant women experiencing verbal abuse had a 57% higher rate of preterm deliveries.
Abstract
Introduction Domestic violence (DV) in the form of verbal abuse is very common among women, especially pregnant women, posing as a serious public health issue that could lead to complications in pregnancy and threaten maternal and fetal outcomes. Studies have determined that domestic verbal abuse (DVA) in pregnancy was more common in women less than 25 years of age as well as in those with low education levels. This study determined the overall prevalence of verbal abuse in pregnant women, in a semi-urban population and is unique in that the verbal abuse in pregnant women with a previous girl child was also determined. This study helps healthcare providers identify the potential causes of DVA in pregnancy and provide timely interventions in the form of counseling for pregnant women and families. Objective This observational study was carried out to assess the prevalence of DVA among…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
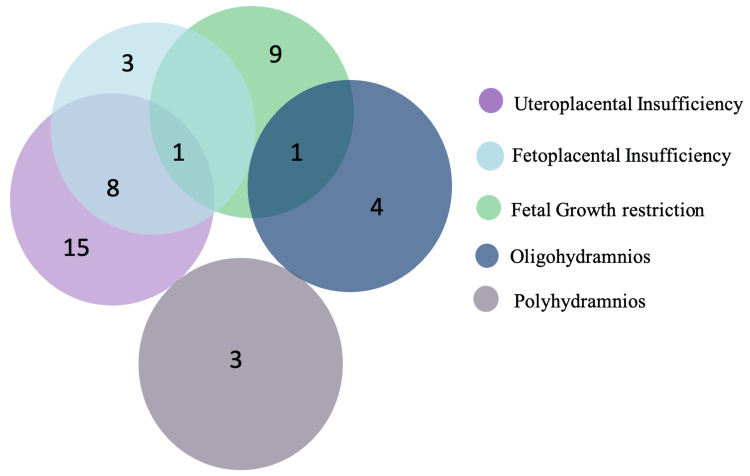 Figure 1
Figure 1| Age group (years) | Frequency | Percentage |
| 18-22 | 41 | 20.5 |
| 23-27 | 86 | 43 |
| 28-32 | 59 | 29.5 |
| 33-38 | 14 | 7 |
| Total | 200 | 100 |
| Parameter | Frequency (%) |
| Primigravida | 101 (50.5%) |
| Multigravida | 99 (49.5%) |
| Preterm delivery | 59 (29.5%) |
| Term delivery | 141 (70.5%) |
| Working | 35 (17.5%) |
| Nonworking | 165 (82.5%) |
| Victims of DVA | Age group | |||||
| 18-23 | 24-27 | 28-32 | 33-38 | Total | p-value | |
| Yes | 28 (68%) | 18 (21%) | 22 (37%) | 6 (43%) | 74 (37%) | <0.0001* |
| No | 13 (32%) | 68 (79%) | 37 (63%) | 8 (67%) | 126 (63%) | |
| Total | 41 | 86 | 59 | 14 | 200 | |
| Occupation status (patient) | Victims of DVA | |||
| Yes | No | Total | p-value | |
| Working | 2 (6%) | 33 (96%) | 35 | <0.0001* |
| Nonworking | 72 (44%) | 93 (56%) | 165 | |
| Total | 74 (37%) | 126 (63%) | 200 | |
| Professional level (partner) | Victims of DVA | |||
| Yes | No | Total | p-value | |
| Level I | 39 | 61 | 100 | 0.073 |
| Level II | 32 | 47 | 79 | |
| Level III | 3 | 18 | 21 | |
| Total | 74 | 126 | 200 | |
| Previous child | Victims of DVA | |||
| Yes | No | Total | p-value | |
| Only boy | 12 (36%) | 21 (64%) | 33 | <0.05* |
| One girl | 16 (34%) | 31 (66%) | 47 | |
| More than one boy | 1 (17%) | 5 (83%) | 6 | |
| More than one girl | 8 (80%) | 2 (20%) | 10 | |
| One boy one girl | 2 (67%) | 1 (33%) | 3 | |
| Birth weight | Victims of DVA | |||
| Yes | No | Total | p-value | |
| IUD | 1 (50%) | 1 (50%) | 2 (1%) | <0.0001* |
| Low | 32 (57%) | 24 (43%) | 56 (28%) | |
| Normal | 41 (29%) | 101 (71%) | 142 (71%) | |
| Total | 74 | 126 | 200 | |
| Gestational age at delivery | Victims of DVA | |||
| Yes | No | Total | p-value | |
| Preterm | 24 (41%) | 35 (59%) | 59 (29.5%) | 0.48 |
| Term | 50 (35%) | 91 (65%) | 141 (70.5%) | |
| Total | 74 (37%) | 126 (63%) | 200 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntimate Partner and Family Violence · Child Abuse and Trauma · Homicide, Infanticide, and Child Abuse
Introduction
The United Nations defines violence against women as "any act of gender-based violence that results in, or is likely to result in, physical, sexual, or mental harm or suffering to women, including threats of such acts, coercion, or arbitrary deprivation of liberty, whether occurring in public or private life” [1]. Women are frequent targets of domestic abuse, with data indicating that it constitutes approximately 5% of the healthy years lost by women in nations with poor economies [2]. Domestic abuse, commonly known as domestic violence (DV), including domestic verbal abuse (DVA), refers to a pattern of behavior that is employed in any relationship to establish or maintain power and control over a spouse or partner. This encompasses any action that alarms, intimidates, terrorizes, manipulates, harms, degrades, blames, or hurts someone [3]. DVA is a variety of phrases or actions intended to coerce, threaten, and uphold authority and control over someone. These consist of taunts, acts of shame and mockery, silent treatment, and attempts to frighten and isolate [4].
DVA in pregnancy frequently goes undetected because victims intend to keep it a secret due to sociocultural norms or are concerned about consequences with their abuser(s) in the event they expose the occurrence [2]. Several factors have been attributed to the prevalence of domestic abuse during pregnancy in some households. These variables include either spouse's low educational status, no or low employment position, impoverishment, unhygienic living conditions, the absence of a male offspring, religious differences, a lack of medical treatment, alcoholism, financial restrictions, and so on [2].
Violence during pregnancy puts at risk both the mother and the baby's health, resulting in a variety of complications such as preterm labor in women, abortion, premature separation of the placenta, and premature rupture of membranes [5]. DV in pregnancy also creates issues for the infant, including low birth weight, fractured bones, soft tissue injury, rupture of the lung or spleen, and hypoxia in the fetus [6]. Abortions, limited contraceptive use, and unintentional pregnancies are all linked to violence [7].
Studies have shown that the incidence of violence within communities, nations, and districts, or between them, indicates that abuse is avoidable and can be abolished. Therefore, there is a need to assess the prevalence of DV and further education among the population [8].
Materials and methods
Study design and setting
This was a hospital-based observational study performed at Dr. D. Y. Patil Medical College, Hospital and Research Centre. This study was reviewed and approved by the DY Patil University Institutional Ethics Subcommittee, with reference number: I.E.S.C./25/2023.
Participants
All pregnant women in the age group of 19-40 years who were admitted to the hospital for delivery between August 1 and February 1, 2023, and who were willing to participate in the study were included. Women with known mental illnesses were excluded.
Inclusion and exclusion criteria
The inclusion criteria for the study comprised women aged between 19 and 40 years who delivered at the institute and were willing to participate. Pregnant women with pre-existing mental illnesses were excluded from the study.
Sample size
A validated modified version of the Abuse Assessment Screen questionnaire was used by a single interviewer on 200 pregnant women admitted for delivery after obtaining their consent.
Data collection and consent
We collected the data using a preformed case record form and a validated modified version of an Abuse Assessment Screening questionnaire, predesigned, pretested, and developed by Neil Jacobson and John Gottman [9]. This questionnaire was used by an interviewer on 200 pregnant women admitted for delivery (Table 9). Each woman was interviewed separately by a single interviewer on the bedside, after feeding her baby, to provide a comfortable and calm environment. Written and informed consent was obtained from all participants following a comprehensive discussion with the patient, ensuring respect for their privacy.
Statistical analysis
Data entry was done utilizing MS Excel (Microsoft Corporation, Redmond, Washington, United States). A statistical analysis was performed using GraphPad Prism 10. Relevant descriptive statistics were analyzed and plotted as frequency and percentage. To ascertain significant associations and patterns within the dataset, Chi-square test was applied wherever needed, and a p-value of 0.05 or less was considered significant.
Results
The study involved 200 pregnant women. The majority of the study population, 86 (43%) pregnant women, were between the ages of 23 and 27 years, subsequently followed by 59 (29.5%) pregnant women between the ages of 28 and 32 years, 41 (20.5%) pregnant women between the ages of 18 and 22, and 14 (7%) pregnant women between the ages of 33 and 38 years (Table 1).
In our study population, 101 (50.5%) of pregnant women were primigravida, while the remaining 99 (49.5%) were multigravida. The majority of the pregnant women, accounting for 141 (70.5%), had term delivery, while 59 (29.5%) had preterm delivery. We also analyzed the working status of these pregnant women and found that 165 (82.5%) were nonworking and 35 (17.5%) were working (Table 2).
Association of age group with DVA
The association between age group and incidence of DVA in the study population was analyzed using the Chi-square test. It was found that the association was statistically significant (p < 0.0001) (Table 3).
Association of the professional status of the patient with DVA
With further interest in looking at whether the working status of the pregnant women in our study had any association with the incidences of DVA, the association was analyzed through a Chi-square test, and it was found that the association was statistically significant (p < 0.0001) (Table 4).
Association between the professional status of the pregnant women’s partners and the incidences of DVA
DVA has been closely linked to the partners’ educational and professional status. Therefore, to analyze the association between the professional level of the partners of our patients and the incidences of DVA, the professional level of the partner was divided into three levels. Level I included professions that required primary education or below, level II included professions that required high school education, and level III included professions that require higher education (graduates in professional degree or nonprofessional degree). A Chi-square test was used and found that the association was not statistically significant (p = 0.073) (Table 5). Although it was noted that the prevalence of DVA was higher in partners with level I professional education as compared to the others.
Association between previous children and DVA
Pregnant women who have had one or more female children previously have been seen to have an additional layer of vulnerability to the traumatic effects of DVA. A Chi-square test was used to analyze the association between the sex of the previous child and the incidence of DVA. It was found that the association was indeed statistically significant (p < 0.05) (Table 6).
Association between DVA and birth weight
DVA during pregnancy can have significant adverse effects on the birth weight of infants. Studies have shown a clear association between exposure to DVA and adverse pregnancy outcomes, including low birth weight. The analysis found that there was a significant association between the incidences of DVA and the fetal birth weight (p < 0.0001) (Table 7).
Association between DVA and gestational age
High levels of stress and anxiety can contribute to complications such as preterm birth. Therefore, Chi-square test was used to find the association between DVA and gestational age. However, it was found that the association was not statistically significant (p = 0.4858) (Table 8).
Insights into the ultrasound findings among pregnant women with DVA
As the gestational age at delivery is an outcome of several underlying factors, we analyzed the ultrasound results and found that the majority, accounting for 15 (7.5%) of the pregnant women had uteroplacental insufficiency, fetal growth restriction in nine (4.5%), oligohydramnios in four (2%) pregnant women, and polyhydramnios in three (1.5%) pregnant women each. Some pregnant women had more than one condition, as indicated in the Venn diagram (Figure 1).
Venn diagram showing ultrasound results among the study population
Discussion
The primary goal of this study was to determine the prevalence of DVA among pregnant women as well as the factors that influence it. According to the findings of this study, verbal abuse was the most common form of DV (37%). Individual, relationship, community, and social concerns all contribute to the risk of domestic and family violence. There is a negative correlation between education and DVA. Lower education levels are associated with a higher risk of DVA [10]. The relationship between women's education and spousal abuse varied by community, with evidence indicating that communal acceptance of mistreatment reduced higher education's protective effect [11]. Many studies have found that violence is associated with poor pregnancy outcomes. Abused women are far more inclined to delay prenatal treatment, experience early labor, have miscarriages, or have low-birth-weight babies [8]. Continuous stress appears to influence prenatal outcomes through changes in individual behavior, interfering with their ability to sustain adequate nutritional status, rest, healthcare, or adjust physiological responses [8]. The current study found a significant rise in DVA among those aged 18-23 years (68%). A study by Samal et al. found a 7.9% prevalence of DVA among individuals under the age of 25 [12]. Another study by Lin et al. found that those exposed to DV had significantly shorter mother ages (p < 0.001) [13]. According to the current study, there is a 44% higher incidence of DVA among pregnant women who are not working. In a study by Samal et al., it was reported that women who completed high school or higher had a reduced incidence of DVA (4.8%) [12]. Another study by Calikoglu et al. found that better educational status reduced the incidence of DV by 12.8 times [14]. DV during gestation was also twice as prevalent among women with less than a high school education (OR = 2.0; 95% CI: 1.17-3.25) as well as those who did not have employment (OR = 2.0; 95% CI: 1.27-3.19) [2].
According to the current study, there is a 41% relationship between DV during pregnancy and low-birth-weight births among pregnant women. In a study conducted by Lin et al., the percentage of low birth weight in the DV-exposed group was significantly higher compared to the unexposed group during full-term childbirth (4.9% vs. 3.3%, p = 0.001) [13].
In India, it is common knowledge historically that there is a relevance to having a girl child, who is treated as a burden. In this study, a unique aspect was added to note the prevalence of DVA in pregnant women who had given birth to a girl child previously. This study found that the previous delivery of a female child had a significant impact on DVA, which was more common, particularly if two female children were born prior (80%). Mahapatro et al. discovered that the desire for male children was much higher (24%) in women experiencing DVA, whereas the demand appeared almost negligible when such an incidence was not observed, which was also statistically significant (z = 6.519; p = 0.0001) [15].
The current study found that partner education had a 39% impact on DVA during pregnancy. Emotional or psychological abuse is the least examined, with few studies on its associated components, because most women do not see it as a kind of abuse and do not openly accept it [12]. The repercussions of DVA on young children during pregnancy continue after delivery. Women who suffer DV during their pregnancy or in the year before pregnancy are much less likely to nurse their newborns, and those who do start nursing are more likely to stop by four weeks postpartum [16].
The American College of Obstetricians and Gynecologists (ACOG) suggests that all women be evaluated for signs and symptoms of DV during routine and prenatal visits [10]. Pregnancy is the one time where healthy women have frequent interaction with health care professionals, which may allow doctors to spot abuse more quickly [17]. Providers should provide assistance and referral information.
Pregnant women are more likely to experience DV than to develop preeclampsia or gestational diabetes. DV is especially dangerous since it threatens both the mother and the fetus. Healthcare practitioners should understand the psychosocial effects of DVA during pregnancy [10]. If medical professionals fail to respond to the woman, it can lead to revictimization and exacerbate feelings of self-pity, hopelessness, and discrimination [18].
Limitations of the study
This study was limited to the semi-urban population admitted for delivery, while there should be a larger study at the community level to find out the prevalence of DVA, its associated factors, and measures to safeguard women.
Conclusions
This research discusses the critical issue of DVA among pregnant women and its profound implications for maternal and fetal health. The results underscore the need for increased awareness strategies to reduce such incidences. As our results suggest, DVA during pregnancy is not only associated with the immediate risks to the well-being of expectant mothers but also with the growth and development of the unborn child. It is therefore of critical importance in the interest of public health that healthcare professionals, policymakers, and advocacy groups collaborate to elucidate the root causes of DVA, provide support and resources for affected women, and implement strategies that encompass education and empowerment of pregnant women.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Declaration on the Elimination of Violence against Women: Proclaimed by General Assembly resolution 48/104 of 20 December 1993 4 2024 1993 https://www.un.org/en/genocideprevention/documents/atrocity-crimes/Doc.21_declaration%20elimination%20vaw.pdf
- 2Magnitude and predictors of female domestic abuse in pregnancy in a patriarchal African society: a cross-sectional study of pregnant women in Enugu, South East Nigeria Pan Afr Med J Njoku IV Enebe JT Dim CC 82402021 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 8607940/3490907110.11604/pamj.2021.40.82.28157 PMC 8607940 · doi ↗ · pubmed ↗
- 3United Nations: What Is Domestic Abuse? 4 2024 https://www.un.org/en/coronavirus/what-is-domestic-abuse
- 4Signs of Verbal Abuse (Emotional and Verbal Abuse) 4 2024 2022 https://www.webmd.com/mental-health/signs-verbal-abuse
- 5Intimate partner violence, forced first sex and adverse pregnancy outcomes in a sample of Zimbabwean women accessing maternal and child health care BMC Public Health Shamu S Munjanja S Zarowsky C Shamu P Temmerman M Abrahams N 5951820182972421610.1186/s 12889-018-5464-z PMC 5934870 · doi ↗ · pubmed ↗
- 6Effect of intimate partner violence on birth outcomes Afr Health Sci Laelago T Belachew T Tamrat M 6816891720172908539510.4314/ahs.v 17i 3.10PMC 5656217 · doi ↗ · pubmed ↗
- 7Spousal physical violence against women during pregnancy BJOG Peedicayil A Sadowski LS Jeyaseelan L Shankar V Jain D Suresh S Bangdiwala SI 68268711120041519875810.1111/j.1471-0528.2004.00151.x · doi ↗ · pubmed ↗
- 8Domestic physical violence and pregnancy: results of a survey in the postpartum period Rev Bras Ginecol Obstet Menezes TC Amorim MMR Santos LC Faundes A 309316252003 https://www.scielo.br/j/rbgo/a/k VW Cj Yjgd P 6649 zn 6hw Trwm/abstract/?lang=en