Emergency Revascularization for Acute Vertebral Artery Occlusion Accompanied by Systemic Lupus Erythematosus: A Case Report
Junpei Nagasawa, Makiko Ogawa, Hiromi Konaka, Masaru Yanagihashi, Osamu Kano

TL;DR
A patient with systemic lupus erythematosus experienced successful emergency treatment for a severe vertebral artery blockage causing stroke.
Contribution
This case report highlights the effectiveness of mechanical thrombectomy in a patient with systemic lupus erythematosus and acute stroke.
Findings
Emergency revascularization using mechanical thrombectomy improved the patient's condition.
Percutaneous transluminal angioplasty and stent placement maintained vertebral artery patency.
The patient showed significant clinical improvement post-treatment.
Abstract
The efficacy of mechanical thrombectomy (MT) for acute ischemic stroke has been established, but there are few reports on the effectiveness of MT for stroke patients with collagen disease. We report the case of a systemic lupus erythematosus (SLE) patient with cerebral infarction who underwent MT. A 48-year-old woman had been diagnosed with SLE for 30 years. She visited our hospital because of dizziness from the day before, but when she arrived at the hospital parking lot, she developed vomiting and impaired consciousness. An MRI revealed increased cerebellar hemisphere infarction and magnetic resonance angiography (MRA) did not visualize the right vertebral artery or basilar artery. Urgent cerebral angiography was performed, and angiography of the right vertebral artery revealed occlusion of the V4 segment of the vertebral artery. In addition to these angiographic findings, the patient…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
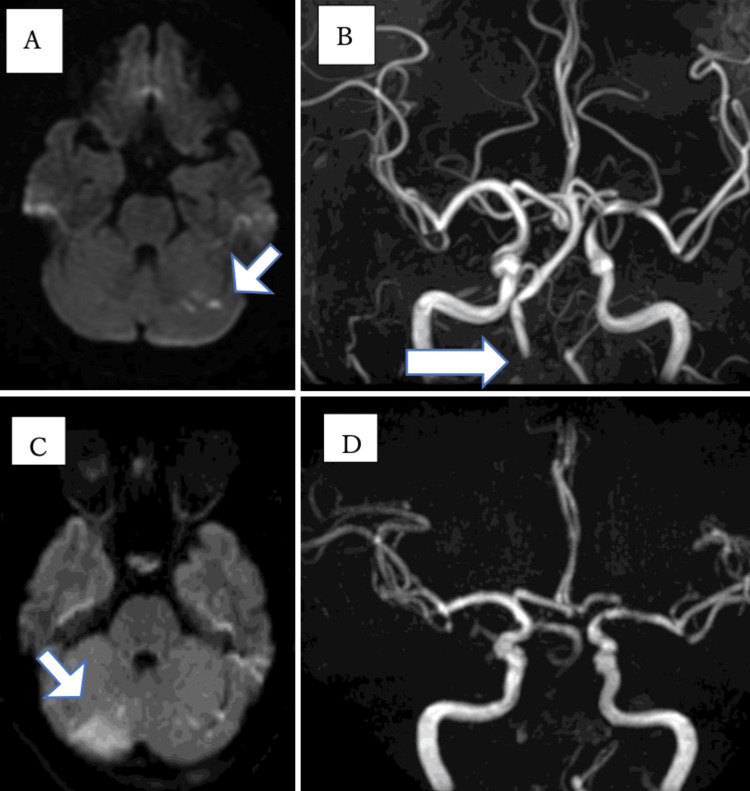 Figure 1
Figure 1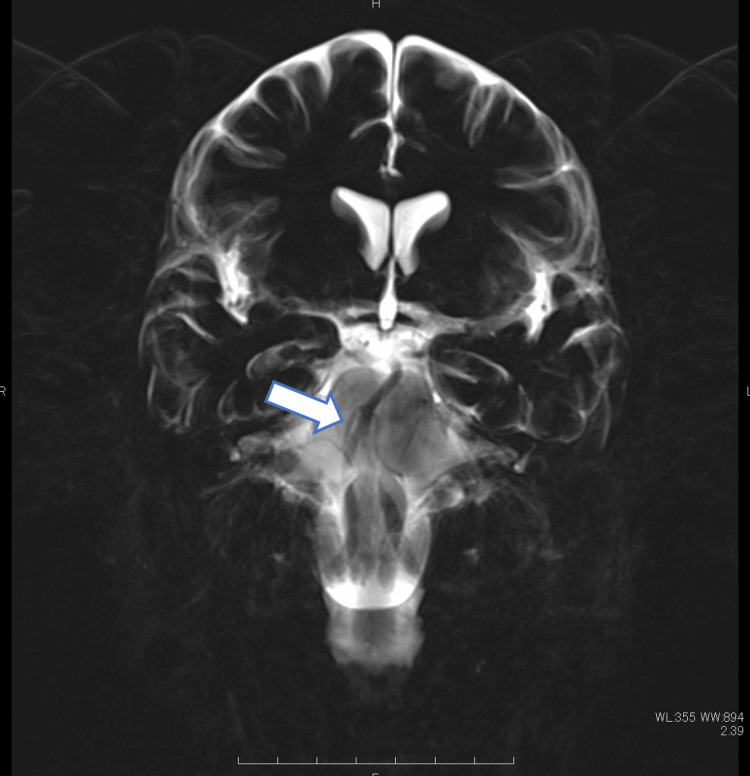 Figure 2
Figure 2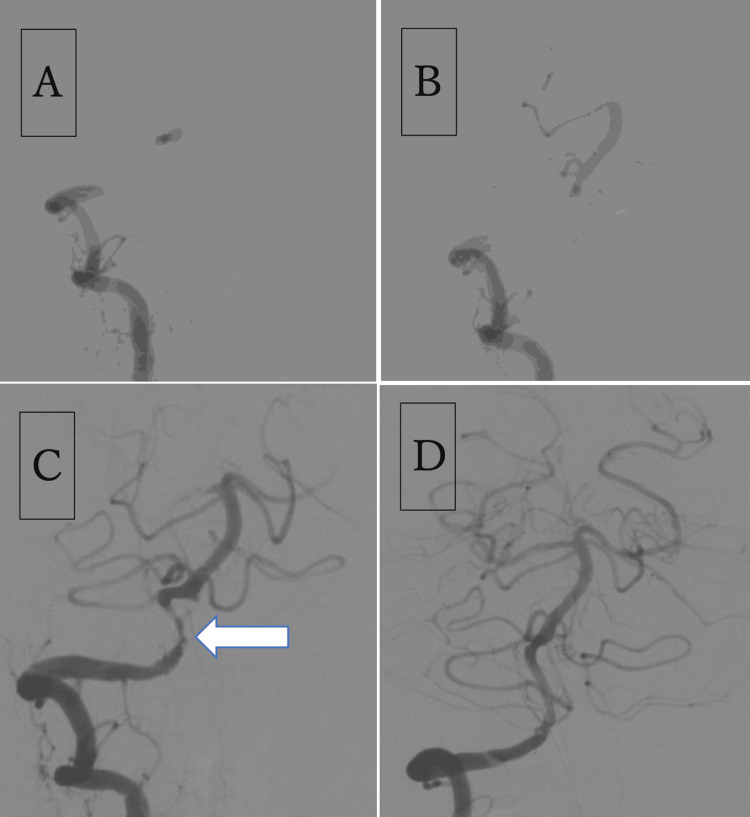 Figure 3
Figure 3| Investigations | Value |
| White blood cells | 9.0 × 103/μl |
| Neutrophils | 5.3 × 103/μl |
| CRP | 0.5 mg/dl |
| Triglyceride | 98 mg/dl |
| LDL-cholesterol | 117 mg/dl |
| HDL-cholesterol | 52 mg/dl |
| HbA1c | 6.0% |
| Glucose | 84 mg/dl |
| PT INR | 1.1 (<1.2) |
| aPTT | 26.5 sec |
| D-dimer | 0.5 μg/ml |
| Anti-cardiolipin antibodies IgG | <0.7 U/m |
| Anti-cardiolipin β2-glycoprotein complex antibody | ≤8 U/ml |
| Lupus anticoagulant (diluted Russell’s Viper venom time) | 0.9 sec |
| Anti-dsDNA antibody | 38 IU/ml |
| C3 | 85 mg/dl |
| C4 | 7 mg/dl |
| SS-A and SS-B antibodies | Negative |
| Authors | Year | Age/sex | Lesion | Etiology | APS | Treatment | mRS score |
| Jiaxia et al.[6] | 2020 | 55/female | BA | Embolic | Positive | MT | mRS 2 |
| Han et al. [1] | 2021 | 38/female | Left MCA | Artery stenosis | Negative | MT | mRS 1 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSystemic Lupus Erythematosus Research · Cerebrovascular and Carotid Artery Diseases · Peripheral Artery Disease Management
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease characterized by systemic inflammatory lesions caused by the deposition of immune complexes, such as anti-DNA antibodies, in tissues. It is an important cause of stroke, whose prevalence among patients with SLE is 3.1% and incidence is 1.25 per 1000 annually; more than half of these cases are acute ischemic stroke (AIS)[1].
Systemic lupus erythematosus can cause ischemic strokes through multiple pathophysiological mechanisms. Cerebrovascular events account for 10% to 15% of SLE deaths [2]. Therefore, treating stroke in patients with SLE is very important. Evidence of the effectiveness of mechanical thrombectomy (MT) for cerebral infarction with large-vessel occlusion (LVO) has been established in recent years. However, there are few reports of patients with SLE, and the effectiveness of MT in patients with SLE is unknown. We encountered a patient with SLE who developed cerebral infarction due to acute vertebral artery occlusion and underwent emergency mechanical revascularization.
Case presentation
A 48-year-old woman had been diagnosed with SLE 30 years ago and treated with prednisolone (PSL) 6 mg, azathioprine 100 mg, and cyclosporine 200 mg. All medicines were taken orally. The SLE activity was relatively stable, with an SLE disease activity index score of 8 points. She had been taking PSL 20 mg orally during a period of high SLE activity 10 years ago but had been taking less than 8 mg PSL for the past few years. She had no common risk factors for arteriosclerosis, such as high blood pressure, diabetes, and dyslipidemia, other than a history of smoking 10 cigarettes a day.
One day when she woke up, she had dizziness. On the same day, she visited a neurosurgery clinic and underwent MRI. The MRI revealed acute cerebral infarction in the left cerebellar hemisphere and bilateral occipital lobes (Figure 1A), and magnetic resonance angiography (MRA) revealed partial stenosis of the right vertebral artery (Figure 1B). The next day, when she arrived at our hospital parking lot, she developed vomiting and impaired consciousness. At the time of onset, she was in a coma, but after about 15 minutes, her consciousness improved slightly. Physical findings on arrival were as follows: blood pressure 144/86 mmHg; heart rate 80 beats/min; respiratory rate 16 times/min; saturation of peripheral oxygen (SpO2) 99%; Glasgow coma scale (GCS) grade E3V4M6. While the MRI revealed increased cerebellar hemisphere infarction (Figure 1C), the MRA did not visualize the right vertebral artery and basilar artery (Figure 1D). The basi-parallel anatomical scanning (BPAS) MRI revealed no abnormal findings in the right vertebral artery (Figure 2).
The MRI taken at onset (A, B) and the MRI taken at our hospital (C, D)A: Acute cerebral infarction in the left cerebellar hemisphere (arrow) and bilateral occipital lobes; B: MRA revealed partial stenosis of the right vertebral artery (arrow); C: MRI performed the next day shows increased cerebellar hemisphere infarction (arrow); D: MRA does not visualize the right vertebral artery and basilar arteryMRA: Magnetic resonance angiography
The BPAS MRIThe BPAS MRI shows no dilated findings of the right vertebral artery (arrow).BPAS: Basi-parallel anatomical scanning
An urgent cerebral angiography was performed to accurately evaluate the cerebral blood flow. Angiography of the right vertebral artery revealed occlusion of the V4 segment of the vertebral artery (Figure 3 A). Angiography of the left vertebral artery revealed a posterior inferior cerebellar artery end pattern in the left vertebral artery. Collateral flow from the internal cervical artery to the posterior circulation via the posterior communicating artery could not be confirmed on either side. Therefore, we concluded that there was no effective blood flow to the posterior circulation owing to right vertebral artery occlusion. In addition to these angiographic findings, the patient also had impaired consciousness and was judged to be indicated for emergency revascularization treatment.
Emergency revascularization for acute right vertebral artery occlusionA: Angiography of the right vertebral artery showing occlusion of the V4 segment of the vertebral artery; B: Angiography from the basilar artery after the lesion crossing the vertebral artery occlusion revealed no occlusion of the basilar artery; C: Angiography showing reperfusion to the basilar artery and right vertebral artery stenosis (arrow); D: The final angiogram reveals no stenosis of the vertebral artery and good blood flow to the basilar artery.
A Trevo NXT 4 mm × 28 mm (Stryker Corp., Kalamazoo, MI, USA) was deployed at the obstructed part of the right vertebral artery through a Trevo Track 21 microcatheter (Stryker Corp.). Immediately after the angiography examination, reperfusion to the basilar artery and severe stenosis of the right vertebral artery were noted (Figure 3 C). Later, the right vertebral artery stenosis caused poor blood flow to the basilar artery and was occluded again. Therefore, percutaneous transluminal angioplasty (PTA) for vertebral artery stenosis was considered necessary. The PTA was performed with a Gateway OTW, 2.0×12 mm, microballoon catheter (Stryker Corp.). The balloon catheter was inflated to a nominal pressure (6.0 atm) for 60 s. This procedure resulted in temporary dilation of the artery stenosis, but restenosis appeared 5 minutes later. Next, the balloon catheter was inflated to the rated burst pressure (10.0 atm) for 60 s. However, the dilation of the stenosis was temporary, and restenosis reappeared 5 minutes after angiography. Therefore, stenting was required to maintain blood flow to the basilar artery. A Neuroform Atlas 3×12 mm (Stryker Corp.) was deployed through a Trevo Track 21 microcatheter, and post-dilation was performed using a SHIDEN 2.5×20 mm microballoon catheter (Kaneka Corp., Tokyo, Japan). Subsequently, angiography was performed every 5 minutes for 30 minutes; this procedure successfully maintained the patency of the vertebral artery and blood flow to the basilar artery (Figure 3 D). The following day, the patient's consciousness improved. She only had mild nausea and there were no remarkable neurological findings.
The patient's laboratory test results are displayed in Table 1. Cerebrospinal fluid (CSF) analysis showed 3 WBCs/μl, protein 55 mg/dL, and normal glucose 52 mg/dL. The thrombus retrieved by MT was a red thrombus, and pathological examination revealed that it was a thrombus containing a mixture of fibrin and red blood cells. Blood tests did not reveal the presence of antiphospholipid antibodies; thus, the patient did not meet the diagnostic criteria for antiphospholipid syndrome (APS). Transthoracic echocardiography revealed no endocarditis. Cerebrospinal fluid examination revealed no increase in the cell counts or protein levels. Follow-up angiography, CT angiography, and MRA showed no restenosis of the right vertebral artery. The patient was discharged after 15 days of hospitalization. At discharge, she had a modified Rankin scale score of 0.
Discussion
Systemic lupus erythematosus increases the risk of ischemic stroke, especially in people aged <50 years [3,4]. Cerebral infarction is more likely to occur in the first year or 10 years after diagnosis of SLE [2]. Furthermore, individuals with SLE have a lower rate of survival after stroke than the general population [5]. Only two cases of MT for cerebral infarction in patients with SLE have been reported, and there have been no reports of PTA and stenting, as in this case (Table 2) [1,6].
The mechanisms underlying cerebral infarction in patients with SLE are assumed to be endocarditis, autoimmune-mediated vasculitis, inflammation-mediated atherosclerosis, or blood hypercoagulability secondary to antiphospholipid antibody (aPL) emergence [7,8]. In pathological examination, cases associated with vasculitis are relatively few, and thrombus, vascular wall degeneration, and endothelial proliferation are often observed [9]. In this case, cerebral infarction might have developed due to autoimmune-mediated vasculitis or inflammation-mediated atherosclerosis, because angiography revealed stenosis of the artery itself, and there were no findings suggestive of endocarditis or APS on transthoracic echocardiography or blood sampling. Arterial dissection is also considered for juvenile vertebral artery occlusion.
However, in this case, no findings suggestive of dissection (such as the pearl and string sign, double lumen, intramural hematoma, and an intimal flap) were found on angiographic or MRI and BPAS images, and vertebral artery dissection was ruled out. Unlike embolic infarction, in infarctions associated with arterial stenosis, even if a temporary recanalization can be obtained with MT alone, artery stenosis is often re-occluded in a short time. Therefore, the effective way to treat such cases is not only to remove the thrombus but also to perform PTA and stenting for stenosis to maintain the patency of the blood vessel.
As already mentioned, there have been no reports of PTA and stenting in SLE patients. However, there are reports of PTA and stenting for intracranial arterial stenosis due to giant cell arteritis. The results of this systematic review show that immediate angiographic improvement in luminal diameter was observed in all cases. Regarding complications, procedure-related arterial dissection was observed in 10.5%, and none were associated with new neurologic deficits [10]. Both PTA and stenting may be effective for vascular stenosis related to collagen disease or vasculitis, but it is necessary to collect more cases related to SLE in the future.
Conclusions
In patients with SLE, severe cerebral infarction associated with large-vessel occlusion can occur. It can occur not only due to thromboembolism but also due to vasculitis. Therefore, it is important to consider the mechanism underlying the infarction and not miss the indication for emergency treatment, including MT and PTA.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Perfusion image guided mechanical thrombectomy combined with tirofiban successfully revascularize systemic lupus erythematosus related acute large vessel occlusion: a case report Medicine (Baltimore) Wang H Hu H Xu J Qian C 0100202110.1097/MD.0000000000025779 PMC 810430033950971 · doi ↗ · pubmed ↗
- 2Stroke in systemic lupus erythematosus: epidemiology, mechanism, and long-term outcome Lupus Guraieb-Chahín P Cantú-Brito C Soto-Mota A 4374452920203215118210.1177/0961203320908947 · doi ↗ · pubmed ↗
- 3Risk of myocardial infarction and stroke in newly diagnosed systemic lupus erythematosus: a general population-based study Arthritis Care Res (Hoboken) Aviña-Zubieta JA To F Vostretsova K De Vera M Sayre EC Esdaile JM 8498566920172812947510.1002/acr.23018 · doi ↗ · pubmed ↗
- 4Ischemic stroke as initial manifestation of systemic lupus erythematosus: a case report and review of the literaturee Neurological Sci Ioannidis S Mavridis M Mitsias PD 26301320183050595710.1016/j.ensci.2018.11.001PMC 6251781 · doi ↗ · pubmed ↗
- 5Overall and cause-specific mortality in patients with systemic lupus erythematosus: a meta-analysis of observational studies Arthritis Care Res (Hoboken) Yurkovich M Vostretsova K Chen W Aviña-Zubieta JA 6086166620142410615710.1002/acr.22173 · doi ↗ · pubmed ↗
- 6Intravascular mechanical thrombectomy for a patient with systemic lupus erythematosus and acute cerebral infarction with antiphospholipid syndrome Int J Psychol Brain Sci Li J Cao S Hu W Zhu Y Xia M 212752020
- 7The atherogenic effect of lupus sera: systemic lupus erythematosus-derived immune complexes stimulate the accumulation of cholesterol in cultured smooth muscle cells from human aorta Clin Immunol Immunopathol Kabakov AE Tertov VV Saenko VA Poverenny AM Orekhov AN 214220631992162364110.1016/0090-1229(92)90225-d · doi ↗ · pubmed ↗
- 8Is atherosclerosis an immunologically mediated disease?Immunol Today Wick G Schett G Amberger A Kleindienst R Xu Q 2733161995788038610.1016/0167-5699(95)80067-0 · doi ↗ · pubmed ↗