Estimating the Economic Impact of Levalbuterol’s Potential Transition From the National Reimbursement Drug List for the Treatment of Pediatric Asthma in China: A Budget Impact Analysis
Tingke Tang, Chunlong Lin, Canghong Zhi, Xuan Li, Yingyu Wu

TL;DR
This study estimates the economic impact of levalbuterol's inclusion in China's drug reimbursement list for treating pediatric asthma.
Contribution
The novelty lies in estimating the budget impact of levalbuterol's inclusion in China's NRDL for pediatric asthma treatment.
Findings
Levalbuterol's inclusion in the NRDL led to cost savings of ¥82.8 million over three years in base-case analysis.
Scenario analysis showed savings decreased to ¥76.1 million over three years.
Results were robust to changes in input parameters according to sensitivity analysis.
Abstract
Background Levalbuterol is a short-acting β2-agonist (SABA) indicated for treating or preventing asthma exacerbation. It was included in the 2020 Chinese National Reimbursement Drug List (NRDL). This study estimates the economic impact of levalbuterol’s status change within and withdrawal from the NRDL in treating pediatric asthma from a publicly funded medical insurance perspective. Methodology A prevalence-based budget impact model was developed. The analysis compared a world with a levalbuterol scenario to a world without levalbuterol. Epidemiological data were obtained from the existing literature. Cost data were estimated based on the drug dosage in clinical trials, real-world settings, and expert opinions. Scenario analysis considered the same length of stay (LOS) in the two groups. One-way sensitivity analyses were carried out to show the impact of varying individual…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
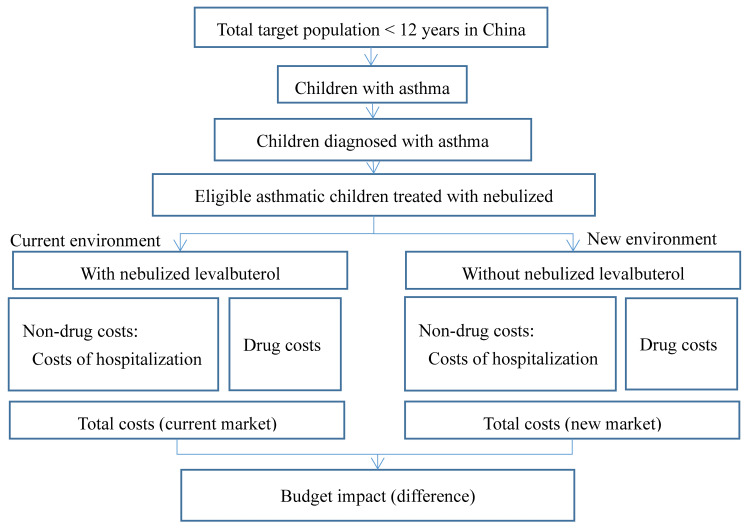 Figure 1
Figure 1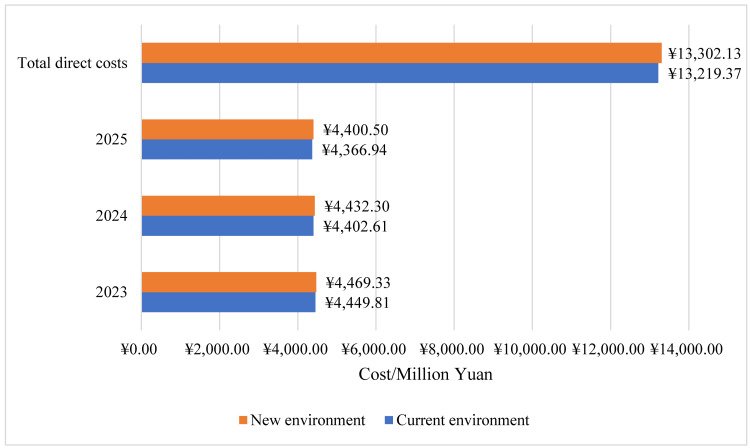 Figure 2
Figure 2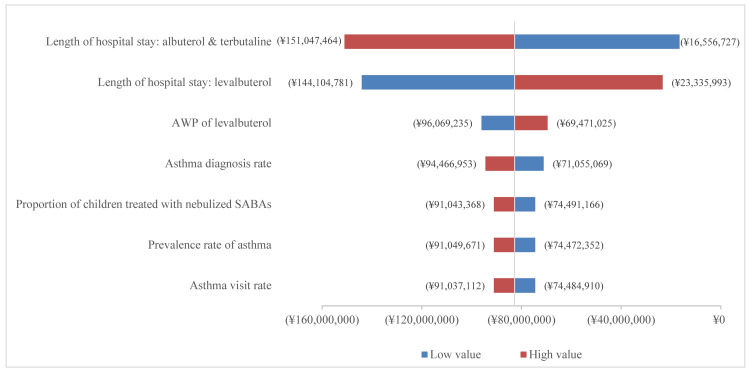 Figure 3
Figure 3| Parameters | Data | Source |
| Natural population growth rate | 0.46% | National Bureau of Statistics [ |
| Overall population in China in 2022 | 1,413,080,284 | National Bureau of Statistics [ |
| Proportion of children under 12 years old | 13.11% | National Bureau of Statistics [ |
| Rate of insurance coverage | 97% | National Bureau of Statistics [ |
| Acute asthma attack rate | 61.45% | National Cooperative Group on Childhood et al. [ |
| Prevalence rate of asthma | 4.91% | National Cooperative Group on Childhood et al. [ |
| Asthma diagnosis rate | 70.70% | National Cooperative Group on Childhood et al. [ |
| Proportion of children treated with nebulized SABAs | 73.4% | National Cooperative Group on Childhood et al. [ |
| Comparators | Dosing | Asthma treatment duration |
| Albuterol Sulfate Nebulized Inhalation Solution 2.5 mL: 2.5 mg | 2.5 mg, four times per day | Outpatient: 3 days; Resident: 7 days |
| Albuterol Sulfate Nebulized Inhalation Solution 2.5 mL: 5 mg | 2.5 mg, four times per day | Outpatient: 3 days; Resident: 7 days |
| Albuterol Sulfate Nebulized Inhalation Solution 2 mL: 10 mg | 2.5 mg, four times per day | Outpatient: 3 days; Resident: 7 days |
| Terbutaline Sulfate Solution for Nebulization 2 mL: 5 mg | 2.5 mg, four times per day | Outpatient: 3 days; Resident: 7 days |
| Levalbuterol Hydrochloride Inhalation Solution 3 mL: 0.31 mg | Low dose: 0.31 mg, high dose: 0.63 mg, dose frequency: four times per day | Outpatient: 3 days; Resident: 7 days |
| Comparator | Current environment (%) | New environment (%) | ||||
| Year 1 | Year 2 | Year 3 | Year 1 | Year 2 | Year 3 | |
| Lishutong | 4.48% | 3.85% | 3.17% | 3.41% | 2.42% | 1.72% |
| Other levalbuterol | 4.14% | 5.93% | 7.47% | 2.17% | 2.14% | 2.11% |
| Abuterol-VBP | 16.05% | 18.49% | 20.28% | 14.97% | 16.80% | 18.30% |
| Abuterol-non-VBP | 11.68% | 10.69% | 9.78% | 11.75% | 10.81% | 9.94% |
| Terbutaline-VBP | 18.14% | 28.05% | 35.37% | 13.73% | 21.42% | 28.00% |
| Terbutaline-non-VBP | 45.50% | 32.99% | 23.92% | 53.97% | 46.42% | 39.92% |
| Parameters | Data | Source | ||||
| Levalbuterol | Albuterol | Terbutaline | ||||
| Base-case analysis | ||||||
| Annual asthma-associated hospitalization rate | 1.1 | Experts panel | ||||
| Levalbuterol: length of hospitalization (day) | 7.17 | Carl et al. [ | ||||
| Albuterol: length of hospitalization (day) | 8.03 | Carl et al. [ | ||||
| Levalbuterol: hospitalization costs per visit (without drug) | ¥1226.77 | Chen et al. [ | ||||
| Albuterol & terbutaline: hospitalization costs per visit (without drug) | ¥1373.91 | Chen et al. [ | ||||
| Scenario analysis | ||||||
| Rate of hospitalization | 45% | 45% | 45% | Carl et al. [ | ||
| Levalbuterol: hospitalization costs per visit (without drug) | ¥1373.91 | Chen et al. [ | ||||
| Albuterol and terbutaline: hospitalization costs per visit (without drug) | ¥1373.91 | Chen et al. [ | ||||
| Other parameters | ||||||
| Reimbursement ratio in an outpatient setting | 50% | National Bureau of Statistics | ||||
| Reimbursement ratio in a resident setting | 65% | National Bureau of Statistics | ||||
| Levalbuterol: Daily dose (mg) | 0.93 | Package insert | ||||
| Albuterol and terbutaline: Daily dose (mg) | 5 | Package insert | ||||
| Levalbuterol, per 1 mg (unit price) | ¥23.11 | Calculated based on price* and market share in 2022 | ||||
| Albuterol-VBP, per 1 mg (unit price) | ¥0.47 | |||||
| Albuterol-non-VBP, per 1 mg (unit price) | ¥3.99 | |||||
| Terbutaline-VBP, per 1 mg (unit price) | ¥0.27 | |||||
| Terbutaline-non-VBP, per 1 mg (unit price) | ¥1.89 | |||||
| Input parameters | Base-case setting | Low input | High input |
| Prevalence rate of asthma (%) | 6.59 | 5.93 | 7.25 |
| Asthma visit rate (%) | 52.70 | 47.43 | 57.97 |
| Asthma diagnosis rate (%) | 70.7 | 60.7 | 80.7 |
| Proportion of children treated with nebulized SABAs (%) | 66.15 | 59.54 | 72.77 |
| Total market share of levalbuterol (%) | 4.81 | 4.33 | 5.29 |
| AWP of levalbuterol (¥/mg) | 23.11 | 20.80 | 25.42 |
| Length of hospital stay: levalbuterol (days) | 7.17 | 6.45 | 7.89 |
| Length of hospital stay: albuterol and terbutaline (days) | 8.03 | 7.23 | 8.83 |
| Year 1 | Year 2 | Year 3 | Total | |
| Total target population (million) | 2.29 | 2.29 | 2.29 | 6.87 |
| Total direct costs | ||||
| Current environment (¥, million) | 4,449.81 | 4,402.61 | 4,366.94 | 13,219.37 |
| Drug costs (¥, million) | 392.46 | 350.82 | 319.28 | 1,062.57 |
| Hospitalization costs (¥, million) | 4,057.35 | 4,051.79 | 4,047.66 | 12,156.80 |
| New environment (¥, million) | 4,469.33 | 4,432.30 | 4,400.50 | 13,302.13 |
| Drug costs (¥, million) | 397.41 | 355.48 | 320.19 | 1,073.08 |
| Hospitalization costs (¥, million) | 4,071.92 | 4,076.82 | 4,080.31 | 12,229.05 |
| Year 1 | Year 2 | Year 3 | Total | |
| Total target population (million) | 2.29 | 2.29 | 2.29 | 6.87 |
| Total direct costs | ||||
| Current environment (¥, million) | 4,487.19 | 4,445.02 | 4,413.09 | 13,345.30 |
| Drug costs (¥, million) | 392.46 | 350.82 | 319.28 | 1,062.57 |
| Hospitalization costs (¥, million) | 4,094.73 | 4,094.20 | 4,093.80 | 12,282.73 |
| New environment (¥, million) | 4,493.53 | 4,452.06 | 4,417.10 | 13,362.69 |
| Drug costs (¥, million) | 397.41 | 355.48 | 320.19 | 1,073.08 |
| Hospitalization costs (¥, million) | 4,096.11 | 4,096.58 | 4,096.91 | 12,289.61 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAsthma and respiratory diseases · Pharmaceutical studies and practices · Inhalation and Respiratory Drug Delivery
Introduction
Asthma is one of the most prevalent chronic diseases in the pediatric population in China. In 2010, the estimated prevalence of asthma was 3.02% in Chinese children aged 0 to 14 years and is increasing [1]. Approximately 77% of asthmatic children will suffer from at least one exacerbation, among which 47.3% will be admitted to the hospital [2]. Per child averaged over the hospitalization period, asthma-related costs were estimated as 2,836 to 3,856 yuan [2]. Overall, the total direct medical cost of pediatric asthma is estimated to be over ¥200 billion (US$30.56 billion) in healthcare costs each year. Asthma exacerbation not only seriously affects the quality of life of children with asthma but also greatly burdens families and society, related to morbidity and mortality [3]. It is estimated that approximately 15 million daily adjusted life years (DALYs) are lost each year, accounting for 1% of the global disease burden [4,5].
Current guidelines recommend that nebulized short-acting β_2_-agonist (SABA) therapy, such as albuterol, terbutaline, and levalbuterol, is the first-line therapy in children with acute asthma across all age groups for symptom relief [6,7]. However, higher SABA use has resulted in an increase in SABA-related adverse drug reactions (ADRs) with a higher likelihood of experiencing asthma exacerbations [6,7], emergency department visits and overnight hospital stays [6,7], and even mortality [6,7].
As a purified albuterol, (R)-albuterol (levalbuterol) has been proven to be clinically comparable to four- to eight-fold higher doses of albuterol [8]. There are several randomized clinical trials of levalbuterol, and both their results and the real-world data indicate that, compared with other SABAs, levalbuterol seems to be more effective and safer, with a lower risk of hospitalization, emergency department visits, and adverse events in children [9-11]. Considering its cost-effectiveness, levalbuterol has been included in China's National Reimbursement Drug List (NRDL) since 2020. However, the economic impact of using levalbuterol for the treatment of asthma in children in China has not been studied.
The purpose of this study was to analyze the economic effects of levalbuterol’s status change within and withdrawal from the NRDL, as a treatment for asthma in children, affecting the budget of the Chinese healthcare payer.
We present the following article by the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) reporting checklist (Appendix) [12].
Materials and methods
Model description and structure
We used Microsoft Excel 2016 to build a three-year budget impact model (BIM), assessing levalbuterol’s economic outcomes within the NRDL for pediatric asthma patients under 12. Figure 1 depicts a schematic representation of the model [13]. Incorporated within this model structure are the prevalence of asthma, the allocation of market shares among various medications, the proportion of medication usage, and the hospitalization costs in China. The model's ethical review was not required as it involved no personal patient data.
Budget impact model structure.Source: [13].
The analysis compared a world with a levalbuterol scenario to a world without a levalbuterol scenario from the public-funded medical insurance perspective and included only direct medical costs. Direct medical costs include pharmacy costs and hospitalization costs. Discounting was not considered in this study, consistent with recommendations of the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) [14].
In scenario analysis, we hypothesized that the length of stay (LOS) remained consistent across both cohorts, averaging 8.03 days, in light of the contradictory results about the advantages of the levalbuterol group as compared to the albuterol and terbutaline group. Total healthcare expenditures were calculated using a macro-costing approach, aggregating resource utilization and applying unit costs in renminbi (RMB, ¥) for 2022.
Model inputs and assumptions
Population
The population parameters are shown in Table 1.
Data from the National Bureau of Statistics, including the natural population growth rate, the overall population, the proportion of children under 12 years of age, and the rate of insurance coverage, were used to estimate the number of children under 12 years of age across Medicare plans [15-18]. The asthma diagnosis rate, acute asthma attack rate, and proportion of children treated with nebulized SABAs were derived from a cross-sectional epidemiological trial conducted in 43 cities among the general population of children [19]. The prevalence of asthma was based on the same epidemiological trial, and the expert panel provided the final statistics. This expert panel, which reflected actual clinical practice, was made up of 70 important chief doctors or prominent physicians with expertise in pediatric respiratory diseases who were chosen from China's most representative institutions. These experts engaged in a comprehensive survey, followed by a Delphi process involving repetitive rounds of discussions and systematic queries to reach a collective agreement.
Treatment Comparators and Market Share
Comparators selected for BIM were based on the most recent Recommendations for the Diagnosis and Management of Bronchial Asthma in Children (2020) for the management of acute asthma [6]. Comparators included nebulized albuterol, terbutaline, and levalbuterol (Table 2).
The data about the treatment course in both outpatient and hospitalized settings in pediatric asthma were obtained from the expert panel. Table 3 illustrates the distribution of market shares among comparator drugs in a scenario where levalbuterol is absent from the current market. Data from January 2015 to December 2022 in the information management system (IMS) was used to calculate market shares in both the new and present settings.
The BIM was deliberately designed to reflect market share acquisition for levalbuterol at the expense of albuterol, as the latter served as the comparative agent in the referenced randomized controlled trial (RCT) [8]. Considering the influences of volume-based procurement (VBP) policy, we predicted a slight decrease in the market share of levalbuterol (while within the NRDL) over the next three years. If levalbuterol was withdrawn from the NRDL, the market share of levalbuterol would decline further.
Assumptions and Clinical Inputs
An electronic search was conducted in the following databases: Medline, Embase, Cochrane Library, Chinese Biologic Medical Literature (CBM), Chinese National Knowledge Infrastructure (CNKI), Chongqing VIP, and Chinese WanFang, for studies published up to May 6, 2023, using the keywords "levalbuterol, levosalbutamol, albuterol, levalbuterol, and terbutaline." The following standards were used to determine whether clinical studies were eligible: (1) studies with an RCT design; (2) participants consisting of children and adolescents aged 18 years or younger; (3) diagnosis of asthma established by a physician using suitable diagnostic benchmarks, which encompasses children under one year exhibiting wheezing symptoms; (4) comparing levalbuterol with albuterol or terbutaline (all of the medications restricted to the inhaled solution), without limitations on the treatment duration, frequency of administration, or dosage. There was no limitation of language.
The preliminary search yielded 63 references, with an additional three references found. After removing duplicates, 60 references remained. Nineteen records were included after the first-level screening's titles and abstracts were assessed. Subsequently, a secondary, full-text evaluation led to the exclusion of 12 further records. A total of seven RCTs comparing levalbuterol and albuterol were included. No RCT that met the exclusion criteria was included. Among the above seven RCTs, the hospital admission rate and the change in pulmonary function were reported in one and three trials, respectively. All trials reported adverse events. Only one trial favored levalbuterol for reducing the risk of hospitalization. One study reported a similar improvement in pulmonary function between 0.31 mg levalbuterol and 2.5 mg albuterol. Another trial reported a similar improvement in pulmonary function between 0.31 mg levalbuterol and 1.25 mg albuterol. Only one study reported a clinical benefit of levalbuterol in reducing the risk of rapid heart rate and hypokalemia. The other five studies reported a similar safety effect between levalbuterol and albuterol.
In this study, levalbuterol and other inhaled SABAs were considered to have equivalent efficacy and safety due to the heterogeneous quality and conflicting results of the published studies. The dosage and frequency of administration of levalbuterol, albuterol, and terbutaline were derived from the package insert.
In the base-case scenario, the assumption was that levalbuterol was clinically comparable to eightfold higher doses of albuterol with more safety advantages based on a published RCT [8], while the efficacy and safety were assumed to be equivalent between albuterol and terbutaline. All of the clinical parameters are shown in Table 4.
Cost Inputs
This BIM only covered the direct expenses of healthcare. Drug expenditures and treatment-related medical expenses were included in the category of direct medical costs. Drug costs were obtained from the Drugdataexpy website and were based on average wholesale prices (AWPs) (Table 4).
The final costs of hospitalization applied for BIM were obtained from the expert panel based on published studies [20-22]. Nonmedical and indirect costs associated with caregiving and lost productivity, as well as additional nutrition costs, were not included in the BIM. All cost parameters are presented as 2022 renminbi in Table 4.
Model outputs for the base-case model: In the settings with and without levalbuterol, total expenses, as well as aggregated costs per budget category (pharmacy and medical), were ascertained. Calculations were made by multiplying the size of the target population by the projected market share of each comparator, followed by multiplication with the respective pharmacy and medical treatment costs. The projected financial impact of introducing levalbuterol (total incremental cost) was calculated from the variance in total costs between the existing and new market conditions.
Statistical analysis
Scenario Analysis
Given the contradictory results on the advantages of levalbuterol in comparison to albuterol, we presumed that the length of hospital stay was comparable in the levalbuterol group.
One-Way Sensitivity Analysis
To evaluate the robustness of the model, a one-way sensitivity analysis was performed on the base case model for certain inputs. The sensitivity analysis examined the key factors influencing the results of the budget impact by altering each input's base-case value independently (Table 5).
Results
The target population of children with asthma under 12 years of age treated with nebulized SABAs in the three-year horizon was estimated to be 6.87 million, while those covered by national medical insurance were estimated to be 6.63 million in China (Table 6).
Base-case analysis
According to estimates, the combined yearly expenses, including drug and non-drug costs, amounted to ¥13,219.4 million for levalbuterol in the NDRL (current environment). As for the new environment (levalbuterol withdrawal from the NDRL), the total expenses gained to ¥13,302.1 million, resulting in a budget depletion of ¥82.8 million over three years (Figure 2; Table 6).
The total annual direct medical costs of current and new environments in pediatric asthma of the base-case analysis.
Scenario and sensitivity analysis
A scenario analysis was performed under the assumption that patients receiving levalbuterol treatment have a similar duration of hospitalization to those receiving albuterol or terbutaline treatment. The total annual costs (drug and nondrug costs) were estimated to be ¥13,345.30 million for levalbuterol in the NDRL (current environment) compared to ¥13,362.69 million for levalbuterol withdrawal from the NDRL (new environment), leading to a total budget depleting of ¥17.39 million after three years (Table 7).
The results of the one-way sensitivity analysis showed that the LOS of albuterol and terbutaline group, the LOS of levalbuterol group, and AWPs of levalbuterol were found to have the largest impact on the model results in the base-case analysis (Figure 3).
One-way sensitivity analysis tornado chart for the base-case analysis of budget impact.AWP, average wholesale price; SABA, short-acting β2 agonist
Discussion
The objective of this study was to estimate the economic impact of changes in levalbuterol's inclusion in the NRDL on pediatric asthma treatment costs. Findings indicate potential budget savings from the use of levalbuterol in asthmatic children under 12 years of age. This research offers supporting evidence, suggesting policymakers should consider integrating levalbuterol as an improved therapeutic option for managing pediatric asthma in China.
It is important to note that there is an ongoing debate concerning the clinical benefit of levalbuterol vs. albuterol because of the significant pharmacy cost difference between these two SABAs and insufficient evidence supporting the clinical benefits of levalbuterol. Previous studies have proven that levalbuterol has more safety and clinical benefits than albuterol. Without (S)-albuterol, a stimulatory factor of intracellular calcium accumulation and an inhibitory factor of adenyl cyclase [23], levalbuterol (R-) might be safer because of the lower risk of inflammation [24]. Moreover, levalbuterol is more effective than albuterol, which may be induced by its higher binding affinity to the β_2_-receptor (100-fold greater than (S)-albuterol) [25], resulting in longer bronchoprotective and bronchodilator effects (almost six to eight hours), which requires a smaller dose and less frequent dosing. A single-center, double-blind RCT, including 482 asthmatic patients aged 1 to 18 years, indicated that the hospitalization rate was significantly lower in the levalbuterol group than in the albuterol group (36% vs. 45%, *P *= 0.02) [9]. A meta-analysis, including seven RCTs, also supported the conclusion that levalbuterol has a lower risk of hospitalization admission (odds ratio [OR] 0.76; 95% confidence interval [CI] 0.58-0.98; I^2^ = 0%) [26]. Our result was consistent with a cost-utility and budget impact analysis, which estimates that levalbuterol’s NDRL entry could save ¥22.3 million for hospitalized COPD patients in three years [27]. However, the results of another population-based retrospective study including 8,172 asthmatic patients aged 2~18 years demonstrated that levalbuterol was not associated with reduced hospitalizations (adjusted incidence ratio 0.93; 95% CI 0.99-1.63)[11]. Given the conflicting results above, this BIM considered no clinical benefit as a conservative estimate in the base-case analysis, and there was still a budget savings of ¥17.39 million.
The primary advantage of our research is that it is the first economic assessment carried out in China that focuses on the costs of nebulized SABA and examines the financial impact of levalbuterol in pediatric asthma. This information can help Chinese decision-makers allocate resources more effectively and enhance patient outcomes.
However, there are still several limitations of our study. First, a predictive analysis was required, so several input parameters, including the proportion of members potentially eligible for levalbuterol, albuterol, and terbutaline and the prevalence of asthma and the proportion of children treated with nebulized SABAs for asthma, needed to be predicted, and applied. These values had to be estimated from historical data [19,28,29]. Moreover, a few assumptions were made for usage data expectations regarding market share due to the nature of the IMS sales data. The IMS sales data used in the model did not have a further breakdown by disease and did not include the sales data from private hospitals; thus, the model assumed that the disease-specific breakdown would not significantly affect the market share of SABAs and would not change the results. Additionally, based on previous research, private hospitals account for only 0.3% of all hospitals providing pediatric services, with public hospitals comprising 99.7%. Therefore, the absence of private hospital data in the IMS sales data is not expected to significantly impact the results of our study [30].
Conclusions
In conclusion, base-case analysis findings from the BIM suggest a potential for a moderate net budgetary effect when levalbuterol is used in pediatric asthma treatment, reflecting a downturn in healthcare spending. For now, the results of this budget impact analysis should be viewed as conservative estimates. BIM should be taken into consideration and evaluated when more information on assumption-based inputs becomes available.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1An epidemiological survey of current asthma control status in China Zhonghua Nei Ke Za Zhi Su N Lin J Liu G 60160653201425376820 · pubmed ↗
- 2The economic burden of medical treatment of children with asthma in China BMC Pediatr Wu P Xu B Shen A He Z Zhang CJ Ming WK Shen K 3862020203281147010.1186/s 12887-020-02268-6PMC 7433054 · doi ↗ · pubmed ↗
- 3The disease burden of childhood asthma in China: a systematic review and meta-analysis J Glob Health Li X Song P Zhu Y 1080110202010.7189/jogh.10.01081 PMC 710121232257166 · doi ↗ · pubmed ↗
- 4Variation in asthma beliefs and practices among mainland Puerto Ricans, Mexican-Americans, Mexicans, and Guatemalans J Asthma Pachter LM Weller SC Baer RD de Alba Garcia JE Trotter RT 2nd Glazer M Klein R 1191343920021199567610.1081/jas-120002193 · doi ↗ · pubmed ↗
- 5Global burden of asthma among children Int J Tuberc Lung Dis Asher I Pearce N 126912781820142529985710.5588/ijtld.14.0170 · doi ↗ · pubmed ↗
- 6Recommendations for diagnosis and management of bronchial asthma in children (2020)Zhonghua Er Ke Za Zhi 7087175820203287271010.3760/cma.j.cn 112140-20200604-00578 · doi ↗ · pubmed ↗
- 7Expert consensus on the prevention and treatment of asthma in children by integrated traditional Chinese and western medicine Chinese Pediatrics of Integrated Traditional and Western Medicine Respiratory Branch of Pediatric Society Chinese Association of Integrative Medicine 185191122020
- 8Low-dose levalbuterol in children with asthma: safety and efficacy in comparison with placebo and racemic albuterol J Allergy Clin Immunol Milgrom H Skoner DP Bensch G Kim KT Claus R Baumgartner RA 93894510820011174227110.1067/mai.2001.120134 · doi ↗ · pubmed ↗