Exploring Choke Holds in Brazilian Jiujitsu Athletes: A Demographic Study
William B Harrington, Patrick R Fugler, Tatiana Midkiff, Stephen J Christensen, Eric Miller

TL;DR
This study explores how often Brazilian jiujitsu athletes experience choke holds and symptoms that may indicate cervical artery dissection.
Contribution
The study is the first to investigate the frequency of choke hold-related symptoms in jiujitsu athletes and their training habits.
Findings
Over half of the athletes reported symptoms consistent with cervical artery dissection.
Younger athletes were more likely to experience these symptoms and trained more frequently and intensely.
The term 'train brain' was described as a cognitive/physical impairing event by most affected athletes.
Abstract
Introduction Brazilian jiujitsu is a relatively new sport that has grown exponentially in popularity along with the growth of the Ultimate Fighting Championship (UFC). In jiujitsu, there are a variety of submissions with a choke hold being one of the most popular. There is a subset of athletes in jiujitsu who believes chokes are safe. However, there have been case reports of relatively young athletes suffering strokes secondary to internal carotid or vertebral artery dissections after being placed in choke holds. There have been manuscripts describing the injury profile in jiujitsu, but none mention stroke or dissections. This study evaluated how frequently chokes happen in jiujitsu and if athletes have ever experienced symptoms consistent with cervical artery dissection (CAD). Additionally, this study aimed to describe the training frequency and baseline demographics of jiujitsu…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
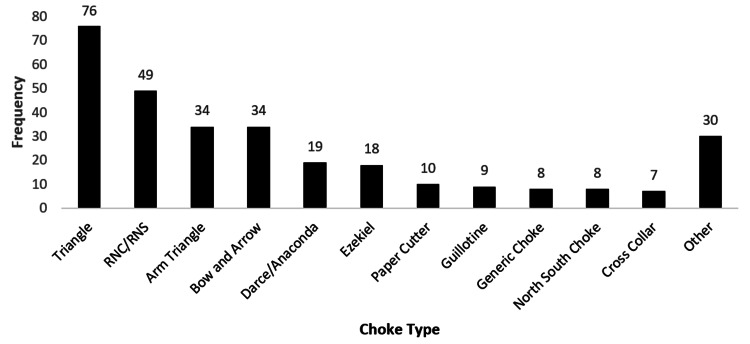 Figure 1
Figure 1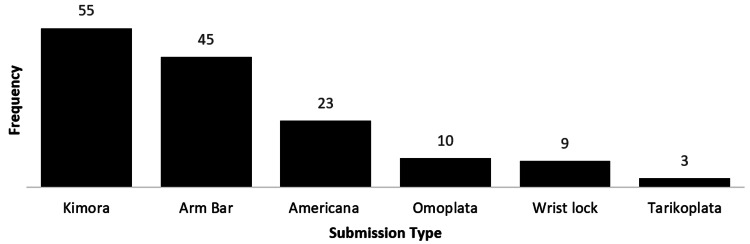 Figure 2
Figure 2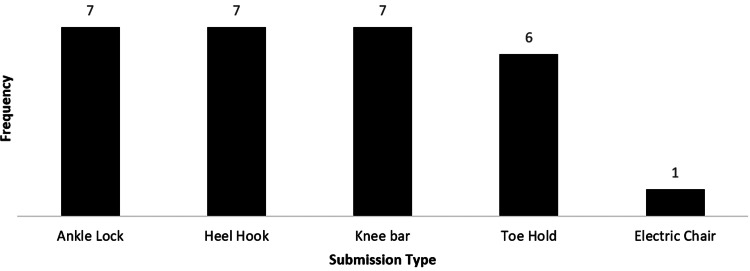 Figure 3
Figure 3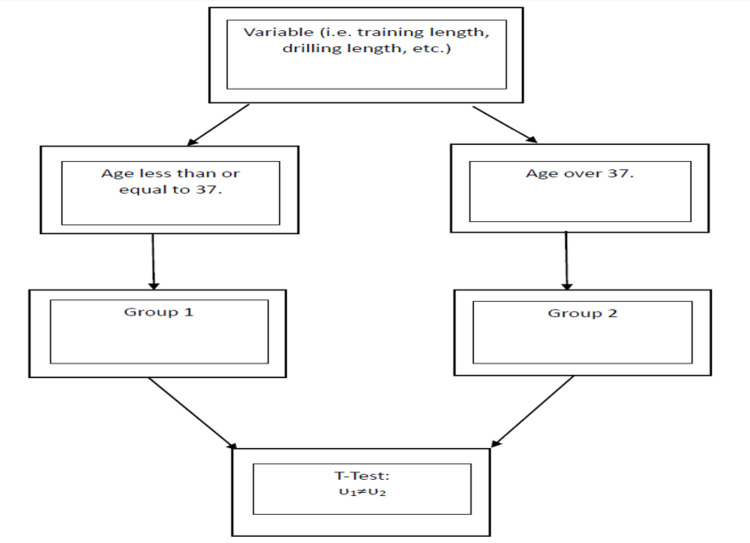 Figure 4
Figure 4| Characteristics | N (%) | Mean | Median |
| Age | 37.1 | 37 | |
| Training length (years) | 6.7 | 4 | |
| Sex (male) | 355 (84.7%) | ||
| Number of training sessions per week: | 3.9 | 4 | |
| -Average time drilling per class (minutes) | 43.3 | 40 | |
| Participates in sparring: | 520 (99.8%) | ||
| -Average time sparring per class (minutes) | 34.4 | 30 | |
| Favorite submission: | |||
| -Choke | 312 (62.3%) | ||
| -Upper extremity submission | 155 (30.9%) | ||
| -Lower extremity submission | 28 (5.5%) | ||
| -Other | 6 (1.2%) | ||
| Number of times submitted by a choke per class | 1.7 | 1 | |
| Number of times submitting someone with a choke per class | 3.1 | 2 | |
| Number of participants who have been choked unconscious | 173 (33.2%) | ||
| -If yes, how many times | 3.4 | 2 | |
| Number of participants who has choked someone unconscious | 189 (36.3%) | ||
| -If yes, how many times | 3.5 | 2 | |
| Number of participants with CVA dissection symptoms post training | 290 (55.7%) |
| t value | p-value | Group 1 mean (stvd) | Group 2 mean (stvd) | |
| Had been choked unconscious vs not | -1.24 | 0.2162 | 31% (0.46) | 36% (0.48) |
| Choked someone unconscious vs not | -1.48 | 0.1386 | 33% (0.47) | 40% (0.49) |
| Training length (years) | -7.56 | <0.0001 | 4.7 years (4.1) | 8.9 years (8.0) |
| Number of training sessions per week | 2.38 | 0.0177 | 4.0 (1.38) | 3.8 (1.3) |
| Length of drilling | 3.35 | 0.0009 | 46.9 min (30.3) | 39.3 min (19.4) |
| Length of sparring | 1.48 | 0.1390 | 35.4 min (16.4) | 33.3 min (15.9) |
| Favorite submission is a choke | 0.14 | 0.8913 | 62.8% (0.48) | 62.2% (0.49) |
| Average class length | 3.50 | 0.0005 | 81.12 min (36.1) | 72.3 min (26.4) |
| Average time training per week | 3.90 | 0.0001 | 338.5 min (217.3) | 274.6 min (145.5) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealthcare and Venom Research · Psychosomatic Disorders and Their Treatments · Sports injuries and prevention
Introduction
Brazilian jiujitsu is a relatively new sport that has increased substantially in popularity with the growth of the Ultimate Fighting Championships (UFC) from its launch in 1993 [1]. Jiujitsu is a sport which features a combination of traditional wrestling, judo, and submission grappling [2]. In a jiujitsu match, an individual wins one of four ways, opponent disqualification, submission, referee decision, or points [3]. The point system in jiujitsu is similar to collegiate wrestling (i.e., points for take downs, and various positions) [3]. If an athlete is placed in a submission, there are three possible outcomes: escape the submission, “tap out,” or suffer the ill effects of the submission [3]. By tapping out, the individual is acknowledging their opponent has beat them and want to stop the match prior to harm occurring [3]. As previously mentioned, if someone is placed in a submission and chooses not to tap, they can undergo serious bodily harm such as bone fractures, torn ligaments/tendons/muscles, unconsciousness, and rarely paralysis or death [2].
Similar to other martial arts, jiujitsu practitioners will practice multiple times per week with jiujitsu forums suggesting that athletes need to train three times a week [4]. Depending if the individual is a competitive jiujitsu athlete or trains as a hobby/self-defense, the number and intensity of their training sessions can greatly vary. A typical jiujitsu class will be structured with a warmup period, a drilling period, and a sparring period [5]. The drilling portion of the class is when the instructor will teach a specific technique and the students will repeatedly perform the movement for a certain amount of time. There is seemingly an infinite amount of techniques with one of the most popular techniques being a choke hold. Drilling most movements and submissions in jiujitsu is a rather benign activity; however, drilling choke holds may not be so safe. When a choke hold is placed in the drilling phase, the partner will usually tap out prior to unconsciousness, but individuals will occasionally be choked unconscious during a drilling session [6,7]. However, unlike in a match, the athlete will immediately be placed in another choke or submission after tapping. This is how submissions are drilled; one partner will be submitted repeatedly for either a set number of reps or time. This repetitive trauma could lead to dissection of the vessels in the neck which can manifest in a variety of different ways. Common symptoms from dissection of the carotid artery include ipsilateral neck pain, headache, facial or eye pain, and Horner syndrome with or without stroke symptoms [8]. Vertebral artery dissections typically present with lateral medullary syndromes, occipital headache, and neck pain [9]. There are case reports of individuals suffering either internal carotid, vertebral artery dissections, or strokes after drilling chokes during a routine training session [8,9].
As mentioned, the jiujitsu community is relatively new but is growing rapidly. A reddit group for jiujitsu holds 782,000 members and ranks in the top 1% of all reddit pages [10]. Unfortunately, there is a proportion of the jiujitsu community that believes chokes are completely safe [11]. Some individuals believe that if you do not tap to a choke hold, you will simply pass out and regain consciousness. Examples of this can be seen by celebrities/professional MMA fighters choking reporters unconscious, jiujitsu schools forcing their students to be choked unconscious as a right of passage, or popular podcasts speaking about the safety of chokes [12-14]. This nonchalant attitude carries over to competitive jiujitsu as well. Depending on the format of the jiujitsu tournament, athletes can be choked unconscious and allowed to compete again after a short 5-10-minute break [3]. Additionally, this rule set is applied to the youth who train jiujitsu as one of the largest jiujitsu organizations allows certain choke holds in children as young as four years old [3]. There are videos online of six-year-old children choking their opponent unconscious and gyms using these videos to promote their training curriculum [15].
With how new of a sport jiujitsu is, it is not well described in literature. There are several studies which describe the injury profile of jiujitsu, but none report the ill effects that can occur from choke holds (vascular dissections, stroke) [16,17]. This is a particular area of interest as internal carotid and vertebral artery dissections are the leading cause of stroke in individuals under the age of 40-45 [18]. For the purpose of this manuscript, we will collectively refer to internal carotid and vertebral artery dissections as cervical artery dissection (CAD). The training regimen of jiujitsu athletes is also not well described. To better understand jiujitsu, our study aimed to gather baseline demographic information regarding training habits, the prevalence of choke holds in jiujitsu, and if they have ever experienced symptoms compatible with a CAD.
Materials and methods
This study was approved and designated as exempt by the Liberty University’s Institutional Review Board (IRB). Data was collected by distributing a survey through social media platforms and groups. Qualtrics (Qualtrics, Provo, UT) was used for the development of the survey. After approval of the final survey, a weblink was generated which was posted to social media. This link was shared with an IRB-approved post to different social media platforms (Facebook, Instagram, etc.). Once the original post was created, it could then be shared freely across social media. The original IRB post ended up being shared to several large jiujitsu-specific Facebook groups. All surveys were completed online.
The survey consisted of 28 questions which captured both quantitative and qualitative data. The research questions and outcomes were developed using the experience of the authors with jiujitsu and interactions with the surveyed population through years of jiujitsu training. Questions which asked specifically about symptoms of CAD were formulated by finding common symptoms in medical literature and peer-reviewed articles. The study collected largely baseline grappling information about the participants such as how long they trained, how often they spar, favorite submission, how frequently they are choked, etc. The full survey is included in Appendix A. The survey did not collect identifiable information from participants, and duplicate prevention was conducted using tools in the Qualtrics software (IP address tracking and geographic location when completing the survey). The survey was built using branching and skip logic. The skip logic was also used to enforce the study’s inclusion/exclusion criteria. If an individual’s answer for a screening criteria did not meet eligibility criteria, they would be routed to the end of the survey. Participants who did not read/consent for the study, were under the age of 18, never trained jiujitsu, or had incomplete responses were not eligible for enrollment.
Once enrollment closed, the de-identified data was exported from Qualtrics into a CSV file. The data exported consisted of individuals who both met and did not meet eligibility criteria; therefore, all non-eligible participants were removed prior to data analysis. Data was then analyzed using Microsoft Excel (Microsoft Corporation, Redmond, Washington, United States) to calculate the mean and standard deviation for the variables included in this study. SAS OnDemand for Academics (SAS Institute Inc., Cary, NC, USA) was used to analyze differences in the study data using a one sample t-test. Differences were considered significant if p-value was less than 0.05. Variables were broken down into two groups, risk vs no-risk, or data above variable mean vs data below variable mean (i.e., participants who had been choked unconscious vs had not been choked unconscious or participant >37 years of age vs ≤37 years of age). Once participants were organized into their respective groups, each variable was analyzed to determine if any statistically significant relationships existed.
The survey consisted of one open-ended question in which the athlete described a jiujitsu term called train brain. As there was only one open ended question, there was not adequate data for formal qualitative analysis. However, the qualitative data was exported and analyzed in an Excel file. The data was coded independently by three authors and any inconsistencies between authors were revised. The qualitive data was analyzed using three themes, cognitive/physical impairment, pain, or cognitive/physical improvement.
Results
The Qualtrics survey was distributed from July 2022 through August 2022 and yielded 573 responses. Out of the 573 responses, 51 participants did not meet eligibility criteria and were therefore excluded from the study. A total of 521 responses were included for analysis. Due to an error when publishing the survey, the question regarding gender was not published for the first 102 participants. The data from these participants were included in analysis as the primary endpoint for this study was to describe the training habits of jiujitsu athletes as a whole, not gender specific. This left a total of 419 participants who answered the gender question of which 355 (84.7%) were male. For the rest of the questions, all 521 participants answered. The average age of participants was 37.1 years and trained an average of four years. An average participant trained four times a week and would drill techniques for an average of 40 minutes per class. Ninety-nine percent (n = 520) of the study participants participated in sparring and sparred for an average of 30 minutes per class. A total of 412 (79.1%) participants reported being choked at least once per class, and 435 (83.4%) choked someone at least once per class. A total of 173 (33.2%) participants had been choked unconscious, while 189 (36.3%) participants had choked someone unconscious. A total of 290 (55.7%) participants experienced symptoms similar to CAD within 24 hours after training. Of those who experienced these symptoms, 170 (58.6%) experienced them less than 10 times. A full breakdown of the demographic information can be found in Table 1.
Moreover, 521 participants answered questions regarding their favorite submission. However, 20 participants submitted an answer which did not address the question. Out of the 501 participants included in this analysis, 312 (62.3%) indicated that a choke is their favorite submission. Upper extremity submissions were the second favorite submission with 155 (30.9%) participants. The full submission data is available in Figures 1-3.
Favorite submission involving a choke holdChoke submission listed in other category: von flue (1), smother choke (1), side choke (1), peruvian necktie (3), mount smother (1), mandible choke (1), lapel/collar choke (5), gogoplata (2), clock choke (3), brabo choke (1), and baseball bat choke (5)
Favorite submission involving upper extremity
Favorite submission involving lower extremity
Data was initially analyzed to determine if any of the variables differed in the number of participants who experienced symptoms consistent with CAD. To evaluate this, each variable was divided into two groups, less than or equal to the average or greater than the average (i.e., training length <= 4 years vs training length > 4). Once separated into their respective groups, odds ratios and 95% confidence intervals (CIs) were calculated in SAS. Age was the only variable which had a significant difference between groups. Participants who were 37 years of age or younger were 1.5337 (95% CI: 1.0827-2.1727) times the odds of a participant over 37 to experience symptoms consistent with CAD.
After revealing the significant difference based on age, additional analysis was conducted to evaluate potential causes for why younger athletes were more likely to experience symptoms. A one sample t-test was conducted to determine if there was a specific variable which significantly differed between age groups. Each variable was separated into two groups depending on age. A flow chart describing how each variable was categorized can be found in Figure 4. Two new variables were created by combing data from two existing variables. The new variables were training time per class (drilling time + sparring time) and time training per week (training days per week + training time per class).
Flow chart which describes how the descriptive statistics were conducted
Five variables were found to have differed significantly based on age: how long they have been training (p-value = <0.0001), number of training sessions per week (p-value = 0.0177), time drilling per class (p-value = 0.0009), training time per class (p-value = 0.005), and time training per week (p-value = 0.0001). Athletes that were 37 years of age or younger have been training for fewer years (4.7 years vs 8.8 years) but train more days per week (4.03 times per week vs 3.76 time per week), drill for a longer amount of time (46.8 minutes per class vs 38.3 minutes per class), attend longer classes (81.12 minutes vs 72.3 minutes), and train for a longer period of time per week (338.5 minutes vs 274.6 minutes). While not statistically significant individuals, 37 or younger sparred for longer each class (35.7 minutes per class vs 33 minutes per class). A full review of descriptive statistics can be found in Table 2.
Qualitative data
In jiujitsu, athletes may experience fogginess, forgetfulness, headaches, etc. after a training session. In some gyms, this term has been referred to as “train brain.” This term does not appear in a literature search. Therefore, a question was developed to ask individuals who experienced train brain to describe it. There was a total of 77 participants who answered they had experienced train brain. Of the 74 responses, 69 were used for analysis, five responses were excluded from analysis due to lack of information. As previously mentioned, since there was only one question, there was not adequate data for formal qualitative analysis. However, the information from the open-ended question was independently coded by three of the authors. From these codes, three themes were created and applied to the responses. Any discrepancies were discussed by the authors, and if a conscious could not be achieved, the data was omitted. The themes were cognitive/physical impairment, cognitive/physical improvement, and pain. Fifty-eight participants were assigned to the cognitive/physical impairment theme. Several examples from this theme are “bit foggy, hard to find words after training, a little light headed,” “disoriented,” “can’t think, put together sentences," just foggy and tired,” “fogginess, trouble "finding words," trouble concentrating, headache,” along with others. Ten participants were assigned to the cognitive/physical improvement theme. Several examples from this theme are "when you focus only on training and nothing else,” “when everything clicked and made sense. You finish training exhausted but emotionally high,” “endorphins from the workout feel so good that all anxieties are gone for a bit. Even though the body is sore, there is a sense of calm and achievement in the brain,” along with others. Lastly, one participant was assigned to the pain them. Several of their responses were “headaches, neck pain.” All of the qualitative data responses can be found in Appendix B. The qualitative data showed that out of those participants who experienced train brain, 84.1% described it as an impairing event.
Discussion
Given the rapid increase in the popularity of jiujitsu, there is little literature to suggest the physiological effects of choke holds. There are several manuscripts which describe the injury profile of jiujitsu. However, none of them describe internal carotid or vertebral artery dissection [16,17]. CAD is the most common causes of stroke in individuals under 45, with 25% of ischemic strokes being caused by CAD [19]. However, this number may be underreported due to difficulty with diagnosis and potential transient nature [20]. Symptoms consistent with CAD such as dizziness, headache, and neck pain were reported by 55% of the participants. While it is highly unlikely that each of 290 participants who experienced these symptoms suffered CAD, it does raise the question about potential cervical artery disease in jiujitsu athletes. Without clinical workup, we cannot conclude what caused their symptoms. This study did not ask if any of the participants received care for their symptoms. Due to the potential transient nature of vascular injury, jiujitsu athletes may not seek care and attribute their symptoms to more common reasons such as dehydration or trauma [21]. Along with dehydration, other less severe causes of these symptoms could be simple ischemia, vasospasm, microemboli, transient global amnesia (TGA), concussion, and others. There is no literature to suggest the uninsurance rate in jiujitsu athletes. Likewise, most athletes work a job to help fund their training and competitions, making it hard to decipher the average income for jiujitsu athletes. Potentially due to jiujitsu being a combat sport, lack of health insurance, distrust of the medical system, or financial strain, some athletes tend to only seek medical care if it is absolutely necessary [21]. Even if an athlete presented to the emergency room for these symptoms, one in 30 athletes will be misdiagnosed [20].
As previously mentioned, there have been several case reports and one case series of jiujitsu athletes suffering CAD after training [8]. While the patient demographics differed between the cases, each participant reported being in a choke hold prior to their symptom onset [8]. There is literature which suggests that there is an association between sportive chokes and CAD [22]. As a choke hold is placed, whether in drilling or in sparring, it will compress the internal carotid arteries leading to decreased blood flow to the middle cerebral artery and eventual unconsciousness [23]. The compression of the carotid arteries can lead a pressure of 400 mmHg over the carotid bifurcation [23]. If a choke hold is placed correctly, meaning large occlusion of internal carotid arteries, the flow reaches a minimum flow rate in the internal carotid artery and middle cerebral arteries 1.3 and 9.5 seconds, respectively [23]. Simply put, a well-placed choke places a large amount of stress to the internal carotid arteries.
Although there is a large amount of stress placed on the vessels with a well-placed choke, the duration of the choke is relatively short lived as the average time to unconsciousness is nine seconds [23]. An area of concern are chokes that are not placed in the right anatomical position. If a choke is not placed over the correct anatomical position, it would decreased the compression of the internal carotids leading to a choke which is inadequate for unconsciousness. This is more common in an amateur mixed martial arts and regional jiujitsu tournaments, but even in professional fighting, there have been instances of athletes being in chokes for 30 seconds or longer [24]. There are instances of jiujitsu practitioners reporting being in choke holds for upward of three minutes without tapping [25]. Athletes will continue to hold the submission in the hope their opponent will eventually tap or pass out [25]. The partial compression of the carotid vessels could lead to high velocity turbulent flow in those vessels. This could be problematic as turbulent flow in the carotids could cause plaque dislodgement leading to embolic stroke. Additionally, atherosclerotic disease of the internal carotid arteries is a risk factor for dissection without the added stress of a choke [19]. Rarely, if the pressure is placed directly to the carotid bodies, it can cause cardiac dysrhythmias leading to cardiac arrest and death [26].
Compression of the blood vessels allows for the accumulation of vasodilatory metabolites which when released cause an immediate dilation of the vasculature. While this dilation is not affected by the duration of the compressive forces, it does increase when there are repetitive compressive forces are applied [27]. Our study showed that athletes are subjected repetitive compressive forces multiple times per class during the drilling portion and during the sparring portion. As athletes train on average 3.9 times per week, they are subjected to these vasodilatory effects often. There is no literature which evaluates vascular changes in jiujitsu athletes during a training session. There have been studies which evaluated the physiology of choke holds, but none have been in jiujitsu athletes [28].
Due to the location of the vasculature in the neck, the internal jugular vein would be compressed along with the internal carotid. As it takes less pressure to compress a vein than an artery, the internal jugular vein would compress prior to the internal carotid artery. Our data showed that jiujitsu athletes choked on average 1.7 times per class and trained an average of 3.9 classes per week. This would minimally lead to partial/total internal jugular and internal carotid occlusion 6.6 times per week. Our average participant could have been choked an estimated 1,414.4 times throughout their jiujitsu career. However, our data asked specifically how many time athletes were submitted per class. This would not account for being placed in chokes during the drilling portion of the class or ill-placed chokes they may have escaped during sparring. Meaning our data likely underreports the total amount of times an athlete has been choked. Over time, the repetitive stress placed from chokes could cause damage to the vessel wall leading to stenosis or venous insufficiency. The latter of which has been associated with episodes of TGA with strenuous activity [29]. TGA is defined as an acute onset of temporary anterograde amnesia and can be precipitated by the aforementioned strenuous activity or choking incidents [30]. Symptoms of TGA may consist of disorientation, forgetfulness, or inability to retain new information [30,31]. Our qualitative data revealed that some participants experienced forgetfulness, disorientation, and the inability to retain new information after a hard training session.
There are certain movements in jiujitsu which lead to a large amount of pressure on the cervical and thoracic spine. Over time, the cumulative effects of this pressure can lead to degenerative disc disease and cervical spine injury [32]. Additionally, there are rare instances of serious cervical spine injury during training, such as subluxation of a vertebral body [33]. The added stress to the cervical spine may lead to osteophyte formation, disc herniation, or loss of vertebral height. All of which can lead to displacement of the vertebral arteries. In addition to the increased risk of stroke, spondylosis increases the risk of vertebral artery dissection in the general population, which may compound the risk to jiujitsu athletes [33]. Displacement of the vertebral arteries leads to a change in blood flow leading to an increased risk of posterior circulation (PC) stroke [34]. Dissections of the vertebral arteries typically occur due to manipulation, trauma, or positional (hyperextension or stretching) of the neck [22]. Neck injuries are common in jiujitsu which would increase the risk of vertebral artery dissection in athletes [18]. There are currently no studies which evaluate the long-term effects this stressor has on vessel walls or the cardiovascular system.
Limitations
Due to oversight, for the first 102 respondents of the survey, we did not collect gender information nor did we ask if participant sought care for their symptoms. The goal of this study was to determine how frequently chokes occur in the sport of jiujitsu and the question was originally omitted. Once this oversight was noticed, the survey was updated with a gender question. As previously mentioned, the goal of this study was to explore choke holds, and therefore, this did not impact the integrity of the study. This survey asked athletes to describe their training regiment which may have led to potential recall bias from the participants. Another possible limitation associated with our study is that the familywise error rate across analysis was not controlled. We did not believe the “universal null hypothesis” for the two groups applied to our particular study. Additionally, we consider this research to be preliminary and encourage further replication.
Conclusions
Our study collected training demographics to give better insight on how jiujitsu athletes train. The data revealed that athletes train an average of four times a week with an average class length of 77.7 minutes (34.4-minute sparring, 43.3-minute drilling) for an average of four years. During a typical week of training, our individuals were choked an average of 1.7 times per class and choked someone an average of 3.4 times per class. Meaning, the average participant in our study has been choked an estimated 1,414.4 and choked someone 2,828.8 times throughout their jiujitsu career. Given the fact that our study population is young (37 years of age), they will have years of stress placed on their cervical vasculature. Our study showed that athletes who were 37 years or younger had a 1.5337 times the odds of experiencing symptoms similar to CAD than those older than 37. Our analysis showed athletes that were 37 years of age or younger have been training for fewer years (4.7 years vs 8.8 years) but train more days per week (4.03 times per week vs 3.76 time per week), drill for a longer amount of time (46.8 minutes per class vs 38.3 minutes per class), attend longer classes (81.12 minutes vs 72.3 minutes), and train for a longer period of time per week (338.5 minutes vs 274.6 minutes) than those older than 37. Similarly, 55.7% of our study participants had experienced symptoms consistent with a cervical artery dissection. While unlikely the 290 participants experienced dissection, it does raise the question about potential cervical vessel disease. The long-term effect of this added stress should be explored. Future studies should be aimed at using imagining techniques to evaluate for potential stenosis, venous valve insufficiency, arteriosclerosis, and mapping of the cervical vasculature.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The UFC fighter who tapped out first 1 2024 Hockensmith R 2023 https://www.espn.com/mma/ufc/story/_/id/38827608/art-jimmerson-one-glove-ufc-1
- 2What is Brazilian Jiu-Jitsu (BJJ)? 1 2024 2023 https://renzogracieacademy.com/about/what-is-brazilian-jiu-jitsu-bjj/
- 3IBJJF Rule Book 1 2024 2024 https://ibjjf.com/books-videos
- 4How often should I train BJJ (Beginner here) 1 2024 2017 http:////www.reddit.com/r/bjj/comments/6e 66gw/how_often_should_i_train_bjj_beginner_here/
- 5What happens in a typical BJJ class? 1 2024 2017 https://escapologybjj.com/what-happens-in-a-typical-bjj-class/
- 6Ryan Hall Accidentally Got Choked To Sleep With Von Flue Choke 1 2024 Ryan Hall 2020 https://www.youtube.com/watch?v=SDG 0ccy YI 48
- 7Kid's Jiu Jitsu Instructor Accidentally Gets Choked Out In Front Of Class 1 2024 2018 https://www.youtube.com/watch?v=e Kr 17h 2n Hb M
- 8Internal carotid artery dissection in Brazilian jiu-jitsu J Cerebrovasc Endovasc Neurosurg 1 2024 Demartini Z Jr Rodrigues Freire M Lages RO Francisco AN Nanni F Maranha Gatto LA Koppe GL 111116192017 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 5678212/.2915247110.7461/jcen.2017.19.2.111PMC 5678212 · doi ↗ · pubmed ↗