CD34‐TdT‐B‐ALL masquerading as Burkitt lymphoma
Manu Juneja, Andrew Wei, Kylie Mason, Tamia Nguyen, John F Seymour, Surender Juneja

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
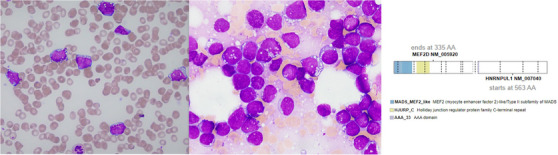 FIGURE 1
FIGURE 1- —Melbourne Research, University of Melbourne 10.13039/501100000987
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphoma Diagnosis and Treatment · Chronic Myeloid Leukemia Treatments · Chronic Lymphocytic Leukemia Research
1
A 23‐year‐old female presented with widespread petechiae and oral mucosal bleeding. There was no palpable lymphadenopathy or hepatosplenomegaly. Complete blood count included haemoglobin 77 g/L (normal 115–155), white cell count 20.4 × 10^9^/L (4.0–12.0), “blasts” 10.6 (52%), neutrophils 3.3 × 10^9^/L (2.0–8.0), platelets 11 × 10^9^/L (150–400). Peripheral blood morphology demonstrated monomorphic immature mononuclear cells with deeply basophilic cytoplasm and numerous small cytoplasmic vacuoles (Figure 1, left image; 1000x magnification) and markedly elevated serum lactate dehydrogenase (14358 IU; 120–250), suggestive of Burkitt leukaemia/lymphoma. Blood was analysed using standard methods as outlined by the ICSH (International Committee for Standardization in Haematology). Immunophenotyping demonstrated CD10+, CD19+ CD20+, CD22+,CD24+, CD34‐, CD38+, CD45+ (dim) and CD58+ with cytoplasmic lambda light chain restriction (without surface light chain expression) consistent with a B‐cell lymphoma or pre‐B ALL. Bone marrow was markedly hypercellular with 83% neoplastic cells with identical morphology (Figure 1, middle image; 1000x magnification). Immunohistochemistry was negative for TdT and CD34. Chromosomal studies identified an unbalanced t(5;8)(q13;p21) resulting in the loss of part of the long arm of chromosome 5, and deletion of 9p by microarray. Fluorescent in‐situ hybridisation did not identify MYC rearrangements typical of Burkitt lymphoma. Targeted molecular studies identified NRAS and BRAF variants and whole genome and transcriptome analysis demonstrated a MEF2D::HNRNPUL1 rearrangement (Figure 1, right image). Prior to molecular results being available, the patient was commenced on R‐CODOX‐M/R‐IVAC, achieving complete remission. With full diagnostic information available, consolidation delivered an ALL regimen. This case highlights how, despite a thorough investigation by all appropriate modalities including morphology, immunophenotyping and cytogenetics, the final correct diagnosis may be delayed until the determination of the molecular profile. Further complicating this case, B‐ALL with MEF2D has only recently been described under the category of B‐lymphoblastic leukaemia/lymphoma with other defined genetic abnormalities (WHO, 2022).
Microscopy of peripheral blood (1000x) (left), bone marrow (1000x) (middle) and schematic of in‐frame MEF2D::HNRNPUL1 fusion transcript (right).
CONFLICT OF INTEREST STATEMENT
The authors declare no conflict of interest.
PATIENT CONSENT STATEMENT
Patient has moved overseas so consent is not feasible. Patient's details are adequately anonymised.
CLINICAL TRIAL REGISTRATION
N/A
ETHICS STATEMENT
All patient treatment protocols in our institution are agreed to by the Institutional Ethics Committee.