Attitudes toward an HPV vaccine for condyloma acuminata and willingness to undergo vaccination among STD clinic attendees in China: Focus on STI prevention with HPV vaccine
Anqi-Liu, Jiali-Quan, Lingxian-Qiu, Yue-Huang, Wujian-Ke, Huachun-Zou, Ting-Wu, Xuqi-Ren

TL;DR
This study explores attitudes and willingness toward HPV vaccination for condyloma acuminata among STD clinic attendees in China, finding high acceptance and the importance of knowledge in reducing vaccine hesitancy.
Contribution
The study provides new insights into HPV vaccine acceptance for CA in China, highlighting factors like awareness and knowledge that influence willingness to vaccinate.
Findings
85.8% of participants accepted the HPV vaccine for CA, with higher acceptance among those who had heard of CA.
Participants who knew about HPV-CA connections and vaccines had better attitudes toward the vaccine.
Over half of participants expected the vaccine price to be under $90.
Abstract
Condyloma acuminata (CA) is a common, and recurrent sexually transmitted disease (STD) that greatly contributes to direct health care costs and has a substantial psychosocial impact. Human papillomavirus (HPV) vaccination (containing L1 protein for HPV types 6 and 11) effectively controls CA. We investigated attitudes toward the HPV vaccine for CA and willingness to undergo vaccination among STD clinic attendees in China. Attendees at STD clinics at two selected hospitals in Guangdong and Jiangsu Provinces from May to September 2017 were requested to complete a self-administered questionnaire for this cross-sectional study. The participants’ median age was 28 years (IQR: 24.0–34.0), and the sex ratio was balanced; 63.5% were from Guangdong, 36.5% were from Jiangsu, and 44.5% had a history of CA. The vaccine acceptance rate was high among the participants (85.8%,235/274) to whom the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
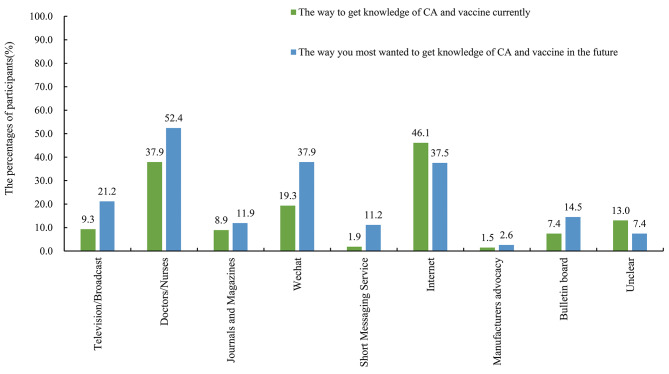 Figure 1
Figure 1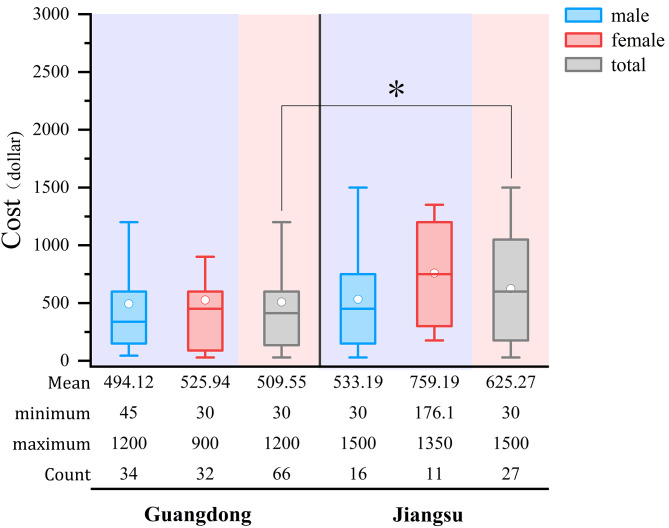 Figure 2
Figure 2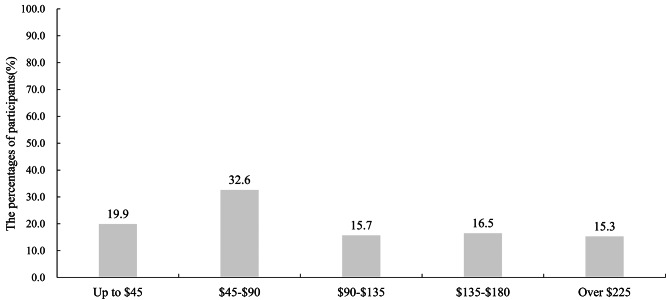 Figure 3
Figure 3- —Xiamen Innovax Biotech Co., Ltd.
- —Jiangsu Provincial Research Hospital
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical Cancer and HPV Research · Genital Health and Disease · Reproductive tract infections research
Introduction
Human papillomavirus (HPV) is known to be associated with various cancers, especially cervical cancer. In 2018, 13% of cancer cases worldwide were attributable to infection, and HPV infection accounted for 31% of all infection-related incident cancer cases [1]. Cervical cancer is the most common HPV-attributable cancer, accounting for 80%; over 95% of cervical cancer cases from HPV infection [2]. China is one of the countries in great part responsible for the cases, with approximately 0.11 million cases [2]. Therefore, many people in China associate HPV with cervical cancer, however, HPV also causes condyloma acuminata (CA, also known as anogenital warts or genital warts). Despite cancer being a priority, we are also concerned about the neglected disease burden caused by CA [3]. Notably, CA is potentially an important co-factor in HIV transmission [4, 5].
CA is a frequently identified clinical symptom of low-risk HPV infection. HPV type 6 (HPV-6) and HPV-11 are associated with approximately 90% of CA cases [6]. The reported incidence of CA in China (0.24–0.29/1000 person years) is lower than that in the general population worldwide (1.6–2.9/1000 person years). However, the true disease burden associated with CA in China, is seriously underestimated due to incomplete disease surveillance and registration systems [7–9]. Furthermore, CA often recurs after initial remission is achieved and requires repeated treatments, with recurrence rates ranging from 6–77% [10]. Although CA is the most frequent benign lesion and is not life-threatening, it is a common problem with a considerable impact on health-care costs; additionally, CA is a source of tremendous psychological pressure and declining patient quality of life [3, 11, 12]. CA is worthy of further attention in high-risk STD populations.
Vaccination has become an effective preventive tool for precancerous lesions and CA. As of September 2023, 64% WHO member states have incorporated the HPV vaccine into their national immunization schedules. Predominantly, these are high-income and upper-middle-income countries; however, many of the world’s most populous nations have not yet included the HPV vaccine in their immunization regimes, with only 12% of females and 6% of males having received the first dose as of 2022 [13]. Despite the increased introduction of the HPV vaccine in low-income and lower-middle-income countries (LLMICs) with the support of Gavi, a persistent global shortage of the HPV vaccine has led to concerns that supply may not meet the increasing worldwide demand. Furthermore, while some nations have embraced a gender-neutral vaccination policy, targeting both boys and girls, the LLMICs primary emphasis continues to be on vaccinating girls aged 9–10 years, a practice that contrasts with the broader age range targeted in developed countries.
HPV vaccines were introduced in mainland China in 2016 [14]. A bivalent vaccine (2vHPV, Cervarix®), and a quadrivalent vaccine (4vHPV, Gardasil^®^), were approved in July 2016 and April 2017, respectively. A 9-valent HPV vaccine (9vHPV, Gardasil^®^9) was licensed in May 2018. The domestic bivalent Innovax’s (Cecolin^®^) and Walvax’s HPV vaccines (Walrinvax^®^) were approved in December 2019 and March 2022, respectively. Each of the five vaccines is licensed for different age ranges at initial, with Cervarix^®^ recommended for ages of 9–25, Gardasil^®^ recommended for ages 20–45, Gardasil^®^9 recommended for ages 16–26, and the two domestic bivalent HPV vaccines are recommended for individuals aged 9–45 and 9–30, respectively. While currently all the HPV vaccines have been proved safe for use in women aged 9–45 years in China (excluding Walrinvax^®^) and have not yet been included in the National Immunization Programme [15]. Immunization of women aged 9–26 is the priority in Chinese guidelines. The current supply of HPV vaccine is insufficient to cover the target population to prevent cancer; thus, there are insufficient vaccines available for the implementation of vaccination to address CA, especially the quadrivalent (Gardasil^®^) and the nonvalent (Gardasil^®^9) HPV vaccines, the only two licensed HPV vaccines that protect against CA [14]. The unaffordable price (595) has largely limited vaccine uptake by individuals in high-risk populations. Hence, an affordable HPV-6/11 vaccine for preventing CA will be applicable to the population at high risk for STDs and may be a potential method to improve the disease burden associated with CA in the future.
At present, one HPV 6/11 bivalent vaccine candidate has specifically been designed to protect against genital warts and other HPV 6/11-related diseases. This vaccine has been preliminarily proven to be well tolerated and demonstrated robust immunogenicity in a phase 1 clinical study (NCT02405520) and is currently being evaluated in a phase 2 clinical trial (NCT02710851) [16]. Despite being in the early stages of validation, the introduction of such a vaccine could potentially contribute to a lower prevalence of CA in high-risk sexually transmitted infections (STIs) populations. The question arises, however, we are interested in exploring whether a vaccine specifically for the prevention of CA is needed when there is already an HPV vaccine for the prevention of both cancer and CA, and whether STD clinic attendees (who are at high risk for STIs, but have a lower chance of receiving quadrivalent or nonvalent HPV vaccines) will be the target potential population? In general, the purpose of this study was to investigate the attitudes toward HPV vaccination for CA and the willingness to undergo vaccination among STD clinic attendees in China.
Materials and methods
Design and participants
A cross-sectional survey covering the knowledge of, attitude toward, and willingness to undergo the HPV vaccine for CA was conducted at the Dermatology Hospital of Southern Medical University and the Affiliated Hospital of Nantong University from May to September 2017. Both centers were visited by people with STIs requiring treatment or who suspected they had an STI. We recruited all individuals who visited the two STD clinics from May to September 2017. STD clinic attendees aged 18 years or older were consecutively included after consent and were asked to complete a self-administered questionnaire designed by a research team comprising physicians and public health and sociology experts, and revised after a pre-survey evaluation in January 2017.
Data collection and questionnaire
The questionnaire covering knowledge, attitude, and practices (KAP) regarding CA and HPV vaccines/cervical cancer vaccines, included information on sociodemographic characteristics, sexual behaviors, history of infection with HPV, HIV and syphilis, the individual’s self-perception on their knowledge of CA and the HPV vaccines/cervical cancer vaccines, and the acceptance of the HPV vaccine for CA and their behavioral willingness regarding vaccination.
The study protocol was reviewed and approved by the Ethics Committees of Guangdong Provincial Dermatology Hospital, Guangzhou, China on November 21, 2016 (approval number: GDDHLS-2016112102). After informed consent was obtained, all eligible participants completed the paper questionnaire independently in a private consulting room, and assistance was provided if required. The questionnaire took approximately 10 min to complete. The collected data were input separately by two different researchers and checked by a third researcher to ensure accuracy.
Statistical analysis
Descriptive statistics were used to compile the participants’ demographic characteristics and their sexual behaviors, history of STIs, and knowledge of CA and HPV vaccines (cervical cancer vaccines) and attitude toward the HPV vaccine for CA. A chi-square test was used to compare categorical variables and test the differences between males and females based on these items. The crude odds ratio (OR) was first proposed in a univariate analysis. The univariate logistic regression analysis began with a full set of sociodemographic, sexual behaviors, history of STIs, knowledge of CA and HPV vaccines /cervical cancer vaccines, and attitude toward the HPV vaccine for CA, and behavioral willingness regarding vaccination to evaluate the associations with the willingness to undergo vaccination and attitudes toward the HPV vaccine for CA. Other variables with a P value < 0.05 and a dummy variable P value < 0.2 in the univariate models were entered into a multivariate logistic regression model to explore factors associated with the HPV vaccine for CA acceptance. The adjusted odds ratio (AOR) and the corresponding 95% confidence intervals (CI) were calculated to assess the results of the regression model. Data regarding the average costs per visit were normally distributed, and the results were analyzed using Student’s t test; otherwise, the rank sum test was used. Statistical analyses were conducted using SAS 9.4, with the significance threshold of a P value of 0.05.
Attitude toward the HPV vaccine for CA: The attitude section of the questionnaire included 3 questions on the individual’s view on the HPV vaccine for CA safety and effectiveness and their willingness to recommend vaccination; the questions were on a six-point scale for assessing individual attitudes (5 points - Strongly Agree, 4 points - Agree, 3 points - Neutral, 2 points - Disagree, 1 point - Strongly Disagree, 0 points - Unclear). Participants were considered to have a positive attitude toward the HPV vaccine for CA when they scored more than 9 points on the 3 attitude questions.
Result
Demographic characteristics, sexual behaviors, and history of STIs
After excluding 40 incomplete questionnaires, 274 (87.3%) participants were included in the study, among whom 174(63.5%) were from Guangdong and 100(36.5%) were from Jiangsu. The detailed baseline information of the included participants was summarized in Table 1, including the sociodemographic characteristics, sexual behaviors, and history of STIs. The participants were distributed evenly by sex (55.5% vs. 44.5%), and the median age was 28 years old (IQR: 24.0–34.0). Furthermore, 88.0% of participants were heterosexual. Approximately half of the participants were married (55.8%), while 80.4% had fixed sexual partners over the past 12 months. The prevalence of CA among the STD clinic attendees was 44.5% (122/274). In 122 STD clinic attendees with a history of CA, 69.7% (85/122) currently had CA, and 56.6% (69/122) had a history of recurrent CA, with an interval of 1–3 months (65.7%) in about two-thirds of them. Furthermore, 11.0% of participants self-reported that they were living with HIV, and 4.7% had been previously diagnosed with syphilis.
Table 1. Sociodemographic characteristics, sexual behaviors, and STIs history in STD clinic attendeesVariableSexTotalχ^2^ P Female%Male% Sociodemographic characteristics SiteGuangzhou104(68.4)70(57.4)174(63.5)3.56170.0591Jiangsu48(31.6)52(42.6)100(36.5)Age18 ~ 25 years57(37.5)39(32.0)96(35.0)1.95670.375926 ~ 40 years85(55.9)70(57.4)155(56.6)> 40 years10(6.6)13(10.7)23(8.4)Educational attainmenthigh school or below62(40.8)49(40.2)111(40.5)0.12830.9379Bachelor degree85(55.9)68(55.7)153(55.8)Master degree and higher5(3.3)5(4.1)10(3.3)Marital statusSingle51(33.6)53(43.4)104(38.0)2.81370.2449Married91(59.9)62(50.8)153(55.8)Separation / Divorce10(6.6)7(5.7)17(6.2)Monthly salary (RMB)^^≦ 2,00026(17.7)11(9.2)37(13.9)10.96090.01192,000–4,99967(45.6)44(36.7)111(41.6)5,000–9,99932(21.8)46(38.3)78(29.2)≧ 10,00022(15.0)19(15.8)41(15.4) Different sexual behaviors Self-identified sexual orientationMSM0(0.0)28(23.0)28(10.2)/< 0.0001Heterosexual151(99.3)90(73.8)241(88.0)Bisexual0(0.0)0(0.0)0(0.0)Unsure1(0.7)4(3.3)5(1.8)Fixed sexual partners in the past 12 months^^Yes133(88.7)84(70.0)217(80.4)14.72430.0001No17(11.3)36(30.0)53(19.6)Temporary sexual partners in the past 12 months^^Yes31(22.5)53(44.9)84(32.8)14.54400.0001No107(77.5)65(55.1)172(67.2)Number of sexual partners in the past 12 months^^<591(68.4)85(72.7)176(70.4)11.37590.0034≧ 52(1.5)11(9.4)13(5.2)040(30.1)21(18.0)61(24.4)Frequency of condom use during sex with fixed partner in the past 12 months^¶^Every time24(20.3)24(21.9)40(20.9)2.68800.4423Always23(19.5)21(28.8)44(23.0)Sometimes53(44.9)27(37.0)80(41.9)Never18(15.2)9(12.2)27(14.1)Frequency of condom use during sex with temporary partner in the past 12 months ^ξ^Every time4(17.4)20(40.0)24(32.9)4.85810.1825Always6(26.1)14(28.0)20(27.4)Sometimes8(34.8)10(20.0)18(24.7)Never5(21.7)6(12.0)11(15.1)Addictive drugs or substances in the past 12 months^^Yes1(0.7)2(1.7)3(1.1)/0.5925No143(99.3)118(98.3)261(98.9)Sexual intercourse under the influence of alcohol in the past 12 months^^Yes19(12.6)32(26.7)51(18.8)8.68120.0032No132(87.4)88(73.3)220(81.2)Frequency of drinking in the past 12 months^^Constantly7(4.6)24(19.8)31(11.4)23.3827< 0.0001Sometimes68(45.0)64(52.9)132(48.5)No drinking76(50.3)33(27.3)109(40.1)Frequency of smoking in the past 12 months^^No smoking144(95.4)66(54.6)210(77.2)65.4037< 0.00011–5 per day5(3.3)17(14.1)22(8.1)Over 5 per day2(1.3)38(31.4)40(14.7) History of STIs History of CAYes60(39.5)62(50.8)122(44.5)3.52720.0604No92(60.5)60(49.2)152(55.5)How many times did you have CA in the past 1 year^δ^013(25.0)7(11.7)20(17.9)5.29890.151215(9.6)6(10.0)11(9.8)229(55.8)34(56.7)63(56.3)≧ 35(9.6)13(21.7)18(16.1)Current status of CA^^^δ^Yes40(70.2)45(75.0)85(72.7)0.34240.5584No17(29.8)15(25.0)32(27.4)Recurrent history of CA^δ^Yes31(60.8)38(65.5)69(63.3)0.26170.6090No20(39.2)20(34.5)40(36.7)Interval of recurrence^§^1-3months20(69.0)24(63.2)44(65.7)/0.17094-6months2(6.9)4(10.5)6(9.0)7-9months1(3.5)2(5.3)3(4.5)10-12months0(0.0)5(13.2)5(7.5)others6(20.7)3(7.9)9(13.4)HIV testing status^^Have never tested before46(35.4)28(26.4)74(31.4)2.22540.3287HIV-negative71(54.6)65(61.3)136(57.6)Living with HIV13(10.0)13(12.3)26(11.0)History of syphilis ^^Have never tested before54(42.5)36(34.0)90(38.6)6.97610.0306No71(56.0)61(57.6)132(56.7)Yes2(1.6)9(8.5)11(4.7)*Data partially missing^¶^Statistics were calculated based on 217 STD clinic attendees who had fixed sexual partners in the past 12 months^ξ^Statistics were calculated based on 84 STD clinic attendees who had temporary sexual partners in the past 12 months^δ^Statistics were calculated based on 122 STD clinic attendees who had a history of CA^§^Statistics were calculated based on 69 STD clinic attendees who had a recurrent history of CA
Among the participants, males had a higher salary than females (χ2 = 10.9609, p = 0.0119). In addition, male STD clinic attendees were more likely than female STD clinic attendees to have engaged in risky sexual behaviors in the past 12 months, such as having temporary sexual partners (χ2 = 14.5440, p = 0.0001), having over 5 sexual partners (χ2 = 11.3759, p = 0.0034), and participating in sexual intercourse under the influence of alcohol (χ2 = 8.6812, p = 0.0032). Additionally, male STD clinic attendees were more likely than females to engage in unhealthy life behaviors, such as frequent drinking (χ2 = 23.3827, p < 0.0001) and smoking (χ 2 = 65.4037, p < 0.0001). Compared with female STD clinic attendees, male STD clinic attendees were more likely to have been diagnosed with syphilis. (χ2 = 6.9761, p = 0.0306). There were no significant sex-based differences in self-reported HIV testing status or history of CA.
Self-perception on knowledge of CA and HPV vaccines
Table 2 showed the participants’ self-perception on their knowledge of CA and HPV vaccines. Approximately 72.3% of STD clinic attendees knew about CA and 42.0% of them had heard about the HPV vaccines /cervical cancer vaccines, with the internet being the main source of this information (around 46.1%), followed by the doctors (37.9%), WeChat (19.3%), and television/broadcast (9.3%) (Fig. 1). However, a sizable proportion of CA disease-aware STD clinic attendees still had poor knowledge of the disease; 39.4–52.2% of STD clinic attendees lacked knowledge of the transmission routes, symptoms and risks associated with CA or of the treatments available for CA.
Table 2. Self-perception on knowledge of CA and vaccines in STD clinic attendeesVariableSexTotalχ^2^ P Female%Male% Self-perception on knowledge of CA Ever heard of CAYes103(67.8)95(77.9)198(72.3)3.44830.0633No49(32.2)27(22.1)76(27.7)Know the route of transmission of CA^ξ^Yes62(60.2)58(61.0)120(60.6)0.01530.9017No41(39.8)37(39.0)78(39.4)Know the symptoms of CA^ξ^Yes60(58.3)54(56.8)114(57.6)0.04020.8410No43(41.8)41(43.2)84(42.4)Know the risks of CA^ξ^Yes54(52.4)52(54.7)106(53.5)0.10600.7448No49(47.6)43(45.3)92(46.5)Know the treatments of CA^ξ^Yes49(47.6)45(47.4)94(47.5)0.00080.9770No54(52.4)50(52.6)104(52.5)Ever heard of HPV infectionYes101(69.7)78(65.6)179(67.8)0.50550.4771No44(30.3)41(34.4)85(32.2)Ever heard of the connection between HPV and CAYes85(59.0)72(61.0)157(59.9)0.10690.7438No59(41.0)46(39.0)105(40.1) Self-perception on knowledge of HPV vaccines Ever heard of HPV vaccine /cervical cancer vaccineYes75(49.3)40(32.8)115(42.0)7.61600.0058No77(50.7)82(67.2)159(58.0)HPV vaccine can prevent CA^^^¶^Yes44(59.5)29(72.5)73(64.0)1.91730.1662No30(40.5)11(27.5)41(36.0)Know the vaccination procedure^¶^Yes26(35.1)10(25.0)36(31.6)1.23440.2666No48(64.9)30(75.0)78(68.4) Behavioral willingness for vaccination Have any of your friends or family members received the HPV vaccines^^Yes29(21.5)17(14.9)46(18.5)1.77100.1833No106(78.5)97(85.1)203(81.5)Have you proactively learned about CA^^Yes65(48.2)52(44.4)117(48.4)0.34570.5566No70(51.8)65(55.6)135(53.6)Have you proactively learned about HPV vaccine^^Yes44(32.6)33(28.2)77(30.6)0.56860.4508No91(67.4)84(71.8)175(69.4)Have you received education about CA^^Yes28(20.7)25 (21.4)53(21.0)0.01480.9031No107(79.3)92 (78.6)199(79.0)Have you proactively discussed CAor the vaccine with others^^Yes32(23.7)28(23.9)60(23.8)0.00180.9662No103(76.3)89(76.1)192(76.2) Data partially missing^ξ^Statistics were calculated based on 198 STD clinic attendees who had heard of CA^¶^Statistics were calculated based on 115 STD clinic attendees who had heard of the HPV vaccine
Fig. 1. The sources of CA and vaccine knowledge. The x axis listed difference sources of knowledge. The y axis represents the percentages of participants getting knowledge with these sources. Participants were allowed to select multiple options when answering questions about their current sources of knowledge on CA and vaccines and their preferred future sources of information on the same topics
Although 67.8% of them had heard of HPV infection, 40.1% were unaware of the connection between CA and HPV. STD clinic attendees seemingly had poor behavioral willingness toward the HPV vaccine; only 18.5% of the STD clinic attendees evaluated in this study had friends or family members who had received the HPV vaccines/cervical cancer vaccines, and 21.0–30.6% had proactively obtained knowledge regarding HPV vaccination, receiving related education or discussing with others.
Among the participants, female STD clinic attendees were more likely than male STD clinic attendees to hear of HPV vaccines/cervical cancer vaccines (χ2 = 7.6160, p = 0.0058). In addition, there was no significant difference between males and females in regards to knowledge of CA and HPV vaccines/cervical cancer vaccines and behavioral willingness toward vaccination.
Factors associated attitudes toward the HPV vaccine for CA and willingness to undergo vaccination
A high willingness to undergo the HPV vaccine for CA was observed (85.8%, 235/274), in our study, and no sex differences were present (male vs. female: 87.7% vs.84.2%). However, only 95 (34.7%) of 274 participants had a positive attitude toward the HPV vaccine for CA. Tables 3 and 4 showed the factors associated with attitudes toward the HPV vaccine for CA and willingness to undergo vaccination for CA. The univariate logistic regression analysis revealed that, among STD clinic attendees, the 9 variables “Age”, “Self-identified sexual orientation”, “Sexual intercourse under the influence of alcohol in the past 12 months”, “History of CA”, “HIV testing status”, “Ever heard of CA”, “Ever heard of HPV infection”, “Ever heard of HPV vaccines/cervical cancer vaccine”, and “Have you proactively learned about CA” were later evaluated in the multivariate logistic regression analysis to predict STD clinic attendees’ willingness to receive the HPV vaccine for CA. A similar procedure was also applied to attitudes toward the HPV vaccine for CA among STD clinic attendees.
Table 3. Willingness to undergo CA vaccination and attitudes toward CA vaccination in STD clinic attendees with different characteristicsVariableWillingness to CA vaccinationCrude odds ratioPositive attitude to CA vaccinationCrude odds ration (%)*OR (95%CI) P n (%)^#^OR (95%CI) P
Sociodemographic characteristics SexMale107(87.7)1.33(0.67,2.68)0.411744(36.1)1.12(0.68,1.84)0.6641Female128(84.2)ref51(33.6)refSiteGuangzhou152(87.4)1.42(0.71,2.81)0.321973(42.0)2.56(1.46,4.49)0.0010Jiangsu83(83.0)ref22(22.0)refAge18 ~ 25 years89(92.7)5.56(1.72,18.01)0.004243(44.8)1.85(0.70,4.92)0.214426 ~ 40 years130(83.9)2.28(0.85,6.10)0.102245(29.0)0.94(0.36,2.43)0.8903> 40 years16(69.6)ref7(30.4)refEducational attainmenthigh school or below92(82.9)ref26(23.4)refBachelor degree134(87.6)1.46(0.73,2.90)0.284865(42.5)2.42(1.40,4.16)0.0015Master degree and higher9(90.0)1.86(0.22,15.55)0.56744(40.0)2.18(0.57,8.32)0.2542Marital statusSingle94(90.4)ref48(46.2)refMarried126(82.4)0.50(0.23,1.08)0.075942(27.5)0.44(0.26,0.75)0.0022Separation/Divorce15(88.2)0.80(0.16,4.01)0.78385(29.4)0.49(0.16,1.48)0.2037Monthly salary (RMB)≦ 2,00033(89.2)ref13(35.1)ref2,000–4,99991(82.0)0.55(0.18,1.73)0.308429(26.1)0.65(0.29,1.45)0.29455,000–9,99968(87.2)0.82(0.24,2.83)0.758430(38.5)1.15(0.51,2.61)0.7306≧ 10,00037(90.2)1.12(0.26,4.84)0.878218(43.9)1.45(0.58,3.61)0.4302 Different sexual behaviors Self-identified sexual orientationMSM27(96.4)4.74(0.63,36.00)0.132415(53.6)2.41(1.09,5.31)0.0291Heterosexual205(85.1)ref78(32.4)refUnsure3(60.0)0.26(0.04,1.63)0.15172(40.0)1.39(0.23,8.51)0.7195Fixed sexual partners in the past 12 monthsYes188(86.6)1.33(0.59,3.00)0.498173(44.6)0.71(0.39,1.32)0.2834No44(83.0)ref22(41.5)refTemporary sexual partners in the past 12 monthsYes75(89.3)1.48(0.66,3.33)0.338336(42.9)1.64(0.96,2.81)0.0724No146(84.9)ref54(31.4)refNumbers of sexual partners in the past 12 months<5156(88.6)2.11(0.98,4.56)0.056868(38.6)1.50(0.80,2.82)0.2030≧ 510(76.9)0.90(0.22,3.77)0.88845(38.5)1.49(0.43,5.19)0.5282048(78.7)ref18(29.5)refAddictive drugs or substances in the past 12 monthsYes2(66.7)ref1(33.3)refNo225(86.2)3.13(0.28,35.36)0.357390(34.5)1.05(0.09,11.76)0.9670Sexual intercourse under the influence of alcohol in the past 12 monthsYes49(96.1)4.95(1.15,21.27)0.031423(45.1)1.72(0.93,3.20)0.0850No183(83.2)ref71(32.3)refFrequency of drinking in the past 12 monthsConstantly26(81.3)1.09(0.53,2.25)0.817013(41.9)1.59(0.70,3.62)0.2659Sometimes114(86.4)0.90(0.30,2.67)0.841947(35.6)1.22(0.71,2.09)0.4706No drinking93(85.3)ref34(31.2)refFrequency of smoking in the past 12 monthsNo smoking179(85.2)ref71(33.8)ref1–5 per day18(81.8)0.78(0.25,2.46)0.670510(45.5)1.63(0.67,3.96)0.2792Over 5 per day36(90.0)1.56(0.52,4.69)0.429514(35.0)1.05(0.52,2.14)0.8842 History of STIs History of CAYes111(91.0)2.28(1.08,4.79)0.029848(39.3)1.45(0.88,2.39)0.1461No124(81.6)ref47(30.9)refHIV testing statusHave never tested before60(64.6)ref20(27.0)refHIV-negative122(89.7)2.03(0.91,4.54)0.083154(39.7)1.78(0.96,3.30)0.0678Living with HIV24(92.3)2.80(0.59,13.26)0.194514(53.9)3.15(1.25,7.95)0.0152History of syphilis ^¶^Have never tested before75(83.3)ref29(32.2)refNo119(90.2)1.81(0.83, 4.00)0.137451(38.6)1.32(0.75,2.33)0.3290Yes11(100.0)4.72(0.23, 95.56)0.31186(54.6)2.52(0.71,8.96)0.1519^¶^Firth penalized maximum likelihood estimation (willingness to CA vaccination)*n (%):number of those willing to receive CA vaccination (the number of those willing to receive CA vaccination/ the total number of individuals in each category)^#^n (%): number of those having positive attitude to CA vaccination (number of those having positive attitude to CA vaccination / the total number of individuals in each category)
Table 4. Vaccination willingness and attitudes of STD clinic attendees with different awareness levels of CA and vaccinesVariableWillingness toCA vaccinationCrude odds ratioPositive attitude to CA vaccinationCrude odds ration (%)*OR (95%CI) P n (%)^#^OR (95%CI) P
self-perception on knowledge of CA Ever heard of CAYes178(89.0)2.97(1.48,5.95)0.002274(37.4)1.56(0.88,2.79)0.1309No57(75.0)ref21(27.6)refEver heard of HPV infectionYes162(90.5)2.74(1.34,5.60)0.005674(41.3)2.29(1.28,4.10)0.0053No66(77.7)ref20(23.5)refEver heard of the connection between HPV and CAYes140(89.2)1.82(0.90,3.69)0.097270(44.6)2.87(1.64,5.02)0.0002No86(81.9)ref23(21.9)ref self-perception on knowledge of HPV vaccines Ever heard of HPV vaccine/cervical cancer vaccineYes107(93.0)3.24(1.43,7.34)0.004957(49.6)3.13(1.87,5.24)< 0.0001No128(80.5)ref38(23.9)ref Behavioral willingness for vaccination Have any of your friends or family members receivedthe HPV vaccinesYes44(95.7)3.80(0.88,16.58)0.074023(50.0)2.38(1.24,4.57)0.0090No173(85.2)ref60(29.6)refHave you proactively learned about CAYes109(93.2)3.10(1.34,7.17)0.008350(42.7)2.22(1.30,3.78)0.0035No110(81.5)ref34(25.2)refHave you proactively learned about HPV vaccineYes71(92.2)2.16(0.85,5.47)0.104439(50.7)2.96(1.69,5.19)0.0001No148(84.6)ref45(25.7)refHave you received education about CAYes49(92.5)2.09(0.70,6.23)0.186124(45.3)1.92(1.03,3.56)0.0396No170(85.4)ref60(30.2)refHave you proactively discussed CA or the vaccine with othersYes56(93.3)2.49(0.84,7.40)0.100431(51.7)2.8(1.54,5.09)0.0007No163(84.9)ref53(27.6)ref*n (%): number of those willing to receive CA vaccination (the number of those willing to receive CA vaccination/ the total number of individuals in each category)^#^n (%): number of those having positive attitude to CA vaccination (number of those having positive attitude to CA vaccination / the total number of individuals in each category)
In the multivariate analysis, among STD clinic attendees, those who had heard of CA demonstrated an over three-fold higher willingness to receive the HPV vaccine for CA (AOR = 3.14, 95% CI: 1.29–7.63, p = 0.0114). Additionally, the multivariate logistic regression model analysis indicated that STD clinic attendees who were aware of the relationship between HPV and CA (AOR = 2.56, 95% CI: 1.31-5.00, p = 0.0060), had heard of the HPV vaccines/ cervical cancer vaccines (AOR = 1.90, 95% CI: 1.02–3.54, p = 0.0444) and had proactively discussed CA or the vaccine with others (AOR = 1.95, 95% CI: 1.00-3.79, p = 0.0488) had better attitudes toward the HPV vaccine for CA.
Healthcare costs for diagnostics and treatment for CA among STD clinic attendees and willingness to pay for the HPV vaccine for CA
A total of 93 STD clinic attendees with CA participated in the section on healthcare costs. Figure 2 showed the average cost for CA per visit according to different regions and sexes. The mean cost associated with diagnostics and treatment for CA per visit was 625.27).
Fig. 2. The costs for per visit of STD clinic attendees. *p < 0.05. The median lines in each box represents the average cost in each group; the lower and upper lines of the box represent the lower and upper values of 95% confidence interval of average cost; the lines beyond the boxes represents the range of cost in each group. The blue, red and grey boxes represent the group of females, male and overall STD clinic attendees respectively
Additionally, Fig. 3 revealed the acceptable payment ranges for HPV vaccination among participants, over half of the participants (52.5%) expected the vaccination to cost less than $90.
Fig. 3. The acceptable range of payment for HPV vaccination. The x axis represents the acceptable range of payment for HPV vaccination. The y axis represents percentage of participants
Discussion
To the best of our knowledge, studies addressing how STD clinic attendees (both females and males) in China view the HPV vaccine for CA are rare. Here, we aimed to investigate willingness and attitude toward the HPV vaccine for CA among STD clinic attendees, and found that willingness and attitude toward the HPV vaccine for CA were positively associated with knowledge.
In our study, the HPV vaccine for CA willingness among STD clinic attendees in Guangdong and Jiangsu was high (85.8%,235/274), and participants were willing to adopt protective behaviors against CA. Under half of the STD clinic attendees (34.7%) had a positive attitude toward the HPV vaccine for CA. The results revealed that awareness of CA was significantly related to willingness to undergo the HPV vaccine for CA among STD clinic attendees. STD clinic attendees who were aware of the HPV vaccine and the relationship between HPV and CA, and had proactively discussed CA or the vaccine with others were more likely to have positive attitudes toward the HPV vaccine for CA. This finding implied that the knowledge of CA and related education was essential for vaccination willingness and positive attitudes, consistent with the findings of previous studies [17–19]. Although a relevant stable marital status and sexual behavior among participants were showed (55% of them were married and 80% of them had fixed sexual partners), the rate of individuals who had a history of CA was high (almost 50%) in our study, which might explain the observed high willingness towards vaccination.
Even among STD clinic attendees at high risk for CA, although most (72.3%) had heard of CA and 67.8% had heard of HPV infection, 40.1% still were unaware of the connection between CA and HPV. The proportion of STD clinic attendees heard of HPV infection (67.8%) was higher than that found among university students in China (51.1%) [17], but lower than that of males recruited at a sexual health clinic in Italy (74.9%) [20], and significantly lower than that in MSM populations in Western countries (73–93%) [20–22]. Notably, although the participants were attendees of two STD clinics and a considerable proportion of them reported a history of CA (44.53%), the proportion of STD clinic attendees aware of the connection between CA and HPV (59.9%) was consistent with that of studies conducted on university students in China (54.0–67.5%) [17, 23, 24]. This result indicates that most STD clinic attendees have limited knowledge of the association between CA and HPV. The self-perception on knowledge of CA and HPV vaccines in STD clinic attendees was in a middle level. Other studies have shown that the more individuals know about HPV manifestations, signs, and forms of prevention, the better their health outcomes will be [25]. Educational programs can potentially broaden knowledge of the association between HPV and CA in the future, and improve knowledge of CA transmission routes, symptoms, risks, and treatments [26].
Our study data showed that patients with CA have a large financial burden of medical care, with the mean cost associated with diagnostics and treatment for CA per visit in Guangdong and Jiangsu being 625.27 respectively. A real-world cost analysis of England showed that lifetime costs per patient diagnosed with anogenital warts was equal to £872 (£884 and £856 for men and women, respectively) [27]. In Peru, given a population of 18.4 million adults between 18 and 60 years of age and a CA prevalence of 2.28%, the annual cost of treating CA was 25.1 million USD (uncertainty interval 16.9, 36.6) [28]. The cost per case of managing CA in Morocco, including recurrence, was estimated at €207–272 for women and €206–233 for men and the total annual cost of medical consultations for CA in Morocco ranged from €310,828 − 404,102 [29]. The annual incidence of CA in Mexico was estimated to be 547,200 cases, with an annual cost of 195 million USD, it also suggested that CA had a significant impact on public health [[30](#CR30)].In our study, over half of STD clinic attendees expected the vaccination to cost less than 90.
Currently, all available HPV vaccines are only accessible to recommended-age females in China, so the affordability and accessibility of HPV vaccination are the priority challenges in the STD high-risk populations, especially among men. Therefore, another kind of HPV vaccine that targets solely HPV 6/11 for preventing CA, could play a role in addressing the issue of inadequate supplies and high price of current licensed HPV vaccines, to meet potential requirements of specific populations. Meanwhile, it should also be noted that an HPV-6/11 vaccine for CA may convey the message against STI, which might stigmatize and influence the acceptability of such a vaccine. It was encouraging that acceptance of the HPV vaccine for CA was high in our survey of STD clinic attendees and previous survey of MSM [31].
CA is a kind of benign lesion that is largely ignored among diseases caused by HPV infection (typically cancer); however, it could also lead to a decline in quality of life in the long term and has caused an unignorable disease burden in some populations. This study revealed that the willingness to be vaccinated and positive attitudes towards the HPV vaccine for CA are significantly linked to knowledge among STD clinic attendees, a very important group at high risk for STIs and HIV infection in China, to provide clues for future methods to address CA-associated health issues.
Limitations
First, in this study, a preliminary exploration was conducted, but the deeper factors influencing the self-perception on knowledge of CA, acceptability of the HPV vaccine for CA and the impact of education on health were not considered. Second, although self-perception regarding knowledge of CA and HPV vaccines/ cervical cancer vaccines among STD clinic attendees was at a middle level, they were willing to accept the HPV vaccine for CA for a reasonable price. We think that an HPV-6/11 vaccine targeting CA might supplement existing HPV prevention strategies, potentially addressing the varied needs of different populations more effectively. However, more studies involving the implementation issues are warranted to be conducted, including but not limited to the cost-effectiveness analysis. Finally, the survey was conducted in 2017 (over 7 years ago) and the results of the survey may differ from the current situation, however, this difference may be very limited. For instance, the existing supply of several HPV vaccines remains in shortage; although the clinical guidelines for the treatment of CA in China in 2021 suggest that the quadrivalent and nonavalent vaccines containing HPV 6 and 11 are recommended for the prevention of CA, the current HPV vaccination strategy available in China until 2024 remains to prevent cervical cancer and not to recommend vaccination for the male population [32]. Over the past several years, people have been exhausted from coping with the COVID-19 pandemic, and the initiatives to pursue issues related to other infectious diseases were neglected and lacked (especially relatively benign lesions, such as CA). Therefore, although our study has some limitations in terms of timeliness, we believe that our results are valuable to CA prevention and control policy-makers in China.
Conclusions
The willingness to undergo vaccination and attitudes toward the HPV vaccine for CA were positively associated with knowledge, and educational programs can have the potential to solve the barriers to the HPV vaccine for CA willingness and attitudes in the future, especially among individuals at high risk for STDs with negative attitudes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1De Martel C Georges D Bray F Ferlay J Clifford GM Global burden of cancer attributable to infections in 2018: a worldwide incidence analysis Lancet Glob Health 202082 e 1809010.1016/S 2214-109X(19)30488-731862245 · doi ↗ · pubmed ↗
- 2Arbyn M Weiderpass E Bruni Lde SanjoséS Saraiya M Ferlay J Estimates of incidence and mortality of cervical cancer in 2018: a worldwide analysis Lancet Glob Health 202082 e 19120310.1016/S 2214-109X(19)30482-631812369 PMC 7025157 · doi ↗ · pubmed ↗
- 3Park IU Introcaso C Dunne EF Human papillomavirus and genital warts: a review of the evidence for the 2015 Centers for Disease Control and Prevention Sexually Transmitted Diseases Treatment Guidelines Clin Infect Dis 201561 Suppl 8S 8495510.1093/cid/civ 81326602622 · doi ↗ · pubmed ↗
- 4Giuliano AR Botha MH Zeier M Abrahamsen M Evan der Glashoff RH High HIV, HPV, and STI prevalence among young Western Cape, South African women: EVRI HIV prevention preparedness trial J Acquir Immune Defic Syndr 20156822273510.1097/QAI.000000000000042525415290 PMC 4378717 · doi ↗ · pubmed ↗
- 5Siqueira JD Curty G Xutao D Hofer CB Machado ES Seuánez HN Composite Analysis of the Virome and Bacteriome of HIV/HPV co-infected women reveals proxies for Immunodeficiency Viruses 201911542210.3390/v 1105042231067713 PMC 6563245 · doi ↗ · pubmed ↗
- 6Dareng EO Adebamowo SN Famooto A Olawande O Odutola MK Olaniyan Y Prevalence and incidence of genital warts and cervical human papillomavirus infections in Nigerian women BMC Infect Dis 20191912710.1186/s 12879-018-3582-y 30616634 PMC 6323853 · doi ↗ · pubmed ↗
- 7Patel H Wagner M Singhal P Kothari S Systematic review of the incidence and prevalence of genital warts BMC Infect Dis 2013133910.1186/1471-2334-13-3923347441 PMC 3618302 · doi ↗ · pubmed ↗
- 8Yue X Gong X Li J Teng F Jiang N Men P Epidemiological features of condyloma acuminatum in national sexually transmitted disease surveillance sites in China from 2008 to 2016 Chin J Dermatology 2017505321510.3760/cma.j.issn.0412-4030.2017.05.003 · doi ↗