Clonal spread of trimethoprim-sulfamethoxazole–resistant Stenotrophomonas maltophilia isolates in a tertiary hospital
Ömür Mustafa Parkan, Hüseyin Kiliç, Emine Alp, Demet Timur, Aycan Gündoğdu, Özlem Ünaldi, Rıza Durmaz

TL;DR
This study found that trimethoprim-sulfamethoxazole-resistant Stenotrophomonas maltophilia isolates in a hospital are clonally related, suggesting possible cross-transmission.
Contribution
The study identifies clonally related S. maltophilia isolates and links sul1 gene in class 1 integrons to trimethoprim-sulfamethoxazole resistance.
Findings
Trimethoprim-sulfamethoxazole resistance in S. maltophilia is associated with the presence of sul1 and intI1 genes.
Twenty-four isolates were clonally related, with five trimethoprim-sulfamethoxazole-resistant isolates sharing a common clone.
No environmental source of S. maltophilia was identified despite clonal spread among patients.
Abstract
The aims of this study were to: (i) determine antibiotic susceptibility of clinical Stenotrophomonas maltophilia isolates, (ii) investigate the presence of different classes of integrons and sul genes responsible for sulphonamide resistance, (iii) assess the molecular epidemiology of the isolates by determining their clonal relatedness, and (iv) investigate the potential sources of infection by collecting environmental samples when necessary. 99 S. maltophilia isolates from clinical specimens of hospitalized patients were screened by PCR for sul1, sul2, sul3 genes, and integron-associated integrase genes: intI1, intI2, and intI3. PFGE was used to determine the clonal relatedness of the isolates. Susceptibility rates for trimethoprim-sulfamethoxazole, levofloxacin, and ceftazidime were 90.9%, 91.9%, and 53.5% respectively. All trimethoprim-sulfamethoxazole–resistant isolates were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
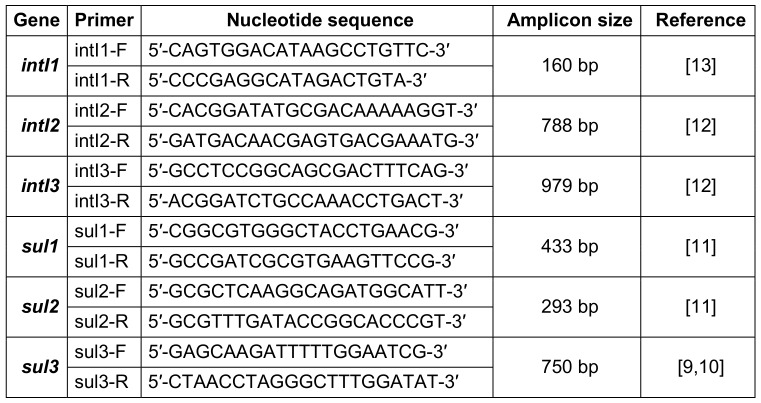 Figure 1
Figure 1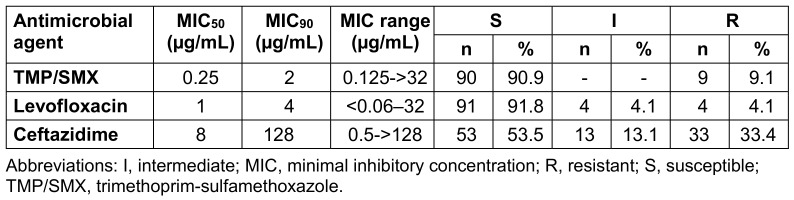 Figure 2
Figure 2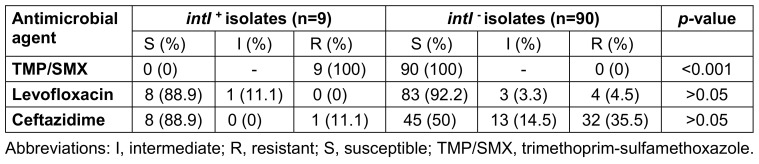 Figure 3
Figure 3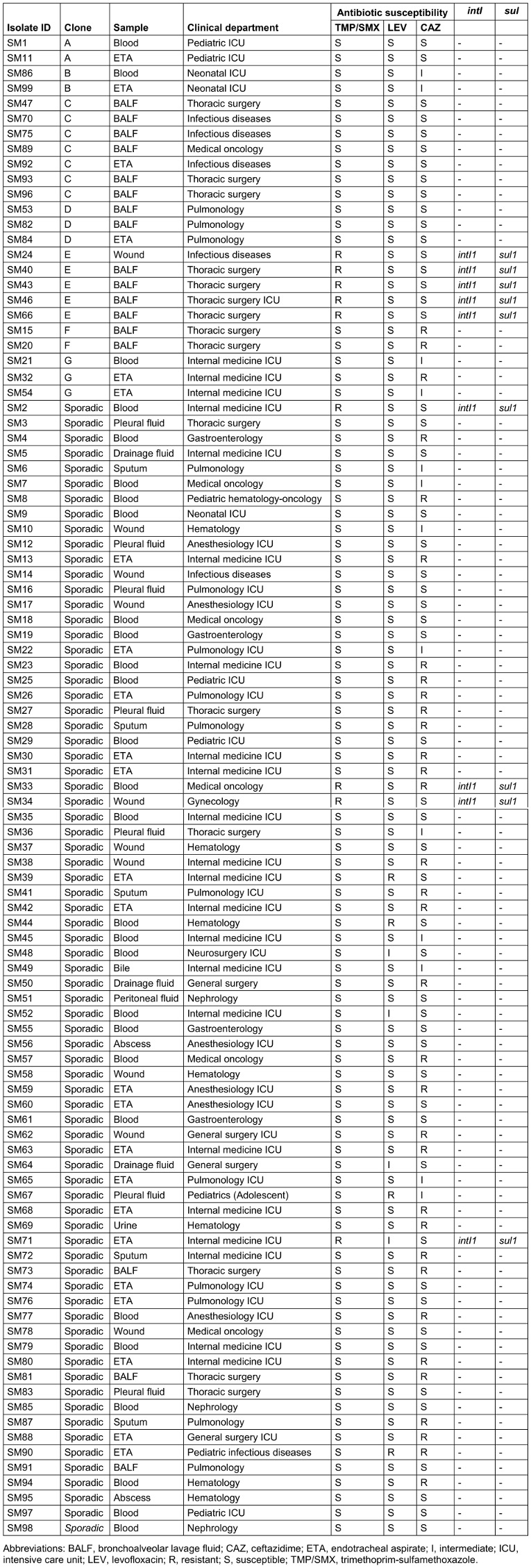 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfections and bacterial resistance · Oral and gingival health research · Blood disorders and treatments
Introduction
Stenotrophomonas maltophilia is a ubiquitous microorganism commonly found in nature and hospitals, especially in humid environments [1]. It is difficult to treat infections caused by S. maltophilia because of its hereditary resistance to many antibiotics. It can also acquire new resistance mechanisms through horizontal gene transfer or mutations [2]. Trimethoprim-sulfamethoxazole (TMP/-SMX) is the first antimicrobial agent of choice in treatment; however, studies conducted worldwide have reported varying rates of resistance to this antibiotic [3], [4]. The sul1 gene carried by class 1 integrons and the sul2 gene associated with insertion sequence common region (ISCR) elements were found to be associated with TMP/SMX resistance in S. maltophilia; surveillance studies are recommended since TMP/SMX resistance has the potential to increase through mobile genetic elements [5]. As they cause problems in treatment, epidemiological typing of nosocomial pathogens, especially multi-resistant microorganisms, allows monitoring of the spread of these agents [6]. In addition to determining antibiotic resistance patterns for the control of nosocomial infections due to S. maltophilia, typing of isolates with molecular epidemiological studies is also important [7]. This study aimed to: (i) determine the susceptibility of clinical S. maltophilia isolates to TMP/SMX, levofloxacin, and ceftazidime, (ii) investigate the presence of integrons and sul genes, (iii) evaluate the molecular epidemiology by using pulsed-field gel electrophoresis (PFGE), and (iv) investigate the potential sources of infection by collecting environmental samples when necessary.
Methods
Bacterial isolates
S. maltophilia isolates from clinical specimens of patients in Erciyes University Faculty of Medicine Hospitals over a 16-month period were evaluated. Clinical specimens were inoculated on BD Columbia agar with 5% sheep blood (BBL™, Becton Dickinson, Heidelberg, Germany) and eosin-methylene blue (EMB) agar (Oxoid, Basingstoke, UK) for culture. The blood culture samples were incubated in the BacT/ALERT^®^ 3D automated blood culture system (bioMérieux, Durham, NC, USA). The bottles with a positive signal were subcultured on BD Columbia agar with 5% sheep blood and EMB agar. Environmental samples were incubated in tryptic soy broth (Oxoid Ltd., Basingstoke, UK) at 37° C for 48 hours before they were subcultured on BD Columbia agar with 5% sheep blood and EMB agar. The BD Phoenix™ automated identification system (Becton Dickinson, Sparks, MD, USA) was used to identify the isolated microorganisms. A single S. maltophilia isolate from each patient was included in the study.
Antimicrobial susceptibility tests
The broth microdilution method was used for ceftazidime and levofloxacin, and the Etest (gradient diffusion) method was used for TMP/SMX to determine the susceptibility of S. maltophilia isolates. Clinical and Laboratory Standards Institute (CLSI) criteria were used to evaluate the results [8].
Broth microdilution
The broth microdilution method was performed by preparing two-fold concentrations of antibiotics in cation-adjusted Mueller-Hinton broth (Oxoid, Basingstoke, UK) in accordance with CLSI recommendations [8]. The bacterial suspension was inoculated with a final inoculum concentration of 5×10^5^ CFU/mL. Pseudomonas aeruginosa strain ATCC^®^ 27853 was used for quality control. After 20 hours of incubation at 35°C, the lowest antibiotic concentration with no visible growth was determined as the minimal inhibitory concentration (MIC).
Etest (gradient diffusion)
This was carried out on cation-adjusted Mueller Hinton agar (Merck, Darmstadt, Germany) medium in accordance with the recommendations of the manufacturer (bioMérieux, Marcy l’Etoile, France). Escherichia coli strain ATCC^®^ 25922 was used for quality control.
Investigation of integron-associated intI and sul genes
DNA was extracted from the isolates grown in pure culture, using the PureLink™ Genomic DNA Mini Kit (Invitrogen, Carlsbad, CA, USA) in accordance with the manufacturer’s recommendations. The primer pairs described previously were used for PCR and are shown in Table 1 (Tab. 1) [9], [10], [11], [12], [13]. AmpliTaq Gold^®^ 360 Master Mix (Applied Biosystems, Foster City, CA, USA) and Labcycler instrument (SensoQuest, Göttingen, Germany) were used for PCR.
Integron-associated intI1, intI2, and intI3 genes
All isolates were tested for integron-associated integrase genes for three different classes of integrons according to the following PCR protocol: an initial denaturation of 94°C for 4 min, followed by 35 cycles comprising a denaturation step of 94°C for 1 min, an annealing step of 56°C for 1 min, and an extension step of 72°C for 1 min. This cycling step was followed by a final extension time of 72°C for 10 min.
Sul1 and sul2 genes
All isolates were tested for sul1 and sul2 genes according to the following PCR protocol: initial denaturation of 95°C for 6 min, followed by 37 cycles consisting of a denaturation step of 95°C for 30 s, an annealing step of 62°C for 45 s, and an extension step of 72°C for 1 min. This cycling step was followed by a final extension time of 72°C for 7 min.
Sul3 gene
All isolates were tested for sul3 gene according to the following PCR protocol: an initial denaturation of 95°C for 5 min, followed by 35 cycles comprising a denaturation step of 95°C for 40 s, an annealing step of 62°C for 40 s, and an extension step of 72°C for 1 min. This cycling step was followed by a final extension time of 72°C for 5 min.
Sequence analysis of the PCR products
PCR products were purified by using ExoSAP-IT^®^ PCR Product Cleanup Reagent (Affymetrix, Santa Clara, CA, USA). The BigDye^®^ Terminator v3.1 Cycle Sequencing Kit (Applied Biosystems, Foster City, CA, USA) was used in the cyclic sequencing reaction of purified PCR products. Two separate cyclic sequencings were performed according to the manufacturer’s recommendations, using forward and reverse primers for each sample. After the cyclic sequencing reaction, precipitation was performed with 2 µL of 125 mM EDTA, 2 µL of 3 M sodium acetate, and 50 µl of 100% ethanol. Samples were sequenced using an ABI 3500xL Genetic Analyzer (Applied Biosystems, Foster City, CA, USA). The DNA sequences were evaluated by comparing them with sequences in the National Center for Biotechnology Information (NCBI) database using the BLAST^®^ sequence analysis tool (http://blast.ncbi.nlm.nih.gov/Blast.cgi).
PFGE analysis
PFGE was carried out as previously described, with some modifications [14]. Bacterial suspensions equivalent to McFarland standard turbidity 4 in cell suspension buffer (100 mM Tris, 100 mM EDTA, pH 8.0) were prepared from pure cultures. 1,000 µL of the bacterial suspensions were centrifuged at 15,000×g for 2 min. After discharging the supernatant, 1,000 µL of cell suspension buffer and 25 µL of proteinase K were added to the pellet and mixed. Bacterial suspensions were mixed with 1% low melting point agarose (Bio-Rad Laboratories, Hercules, CA, USA) containing 1% sodium dodecyl sulfate and filled into the plug molds. The solidified agarose plugs were placed in tubes containing 5 mL of cell lysis buffer (50 mM Tris, 50 mM EDTA, pH 8.0, 1% sarcosine) and 25 µL proteinase K and kept in a shaking water bath set at 55°C for 2 h. After lysis, the buffer was discharged and the tubes were filled with 10 mL of sterile ultrapure water, then washed for 15 min in a shaking water bath at 55°C. The same procedure was performed once again with ultrapure water, then repeated three times using TE buffer (10 mM Tris, 1 mM EDTA, pH 8.0). A piece measuring 4×5.5 mm was cut from each plug. The cut pieces were placed in microcentrifuge tubes containing 100 µL of restriction buffer (FastDigest^®^, Fermentas, Vilnius, Lithuania) and incubated at 37°C for 10 min. After the restriction buffer in the tubes was removed with a micropipette, 2.5 µL of restriction enzyme SpeI (FastDigest^®^, Fermentas, Vilnius, Lithuania), 10 µL of restriction buffer, and 87.5 µL of nuclease-free sterile distilled water were added to each tube and incubated at 37°C for 1 h. For electrophoresis, 1% PFGE-grade agarose (Amresco, Solon, OH, USA) was prepared and the CHEF-DRII system (Bio-Rad Laboratories, Nazareth, Belgium) was used. The running temperature was set at 14°C under the following conditions: switch times ranging from 5 to 30 s, angle 120°, field strength 6 V/cm for 16 h; and switch times ranging from 1 to 5 s, angle 120°, field strength 6 V/cm for 4 h. Gel Logic 2200 Imaging System (Kodak, Rochester, NY, USA) was used to photograph the DNA bands. The images were analyzed using BioNumerics version 7.5 (Applied Maths, Sint-Martens-Latem, Belgium). Cluster analysis was performed using the unweighted pair group method with mathematical averaging (UPGMA) algorithm, and the molecular relatedness of the isolates was determined using the Dice coefficient, with 1.5% tolerance and 1% optimization. Isolates with ≥90% similarity were considered to be in the same clone and were named with a letter.
Statistical analysis
Fisher’s exact test was used to evaluate differences in the prevalence of intI between antibiotic-resistant isolates. A p-value less than 0.05 was considered statistically significant.
Results
S. maltophilia isolates
A total of 99 S. maltophilia isolates from various clinical specimens were included in the study. 52.5% of the patients were male; the median age was 59 (range: 0–89). While 47.5% of the patients were hospitalized in intensive care units (ICUs), 35.4% were hospitalized in non-surgical clinics (14.2% hematology and oncology, 7.1% pulmonology, 5.1% infectious diseases, 9% other), and 17.1% in surgical clinics (14.1% thoracic surgery, 2% general surgery, 1% gynecology). 46.5% of the clinical samples were respiratory tract samples [24.2% endotracheal aspirate (ETA), 17.2% bronchoalveolar lavage fluid (BALF), 5.1% sputum]. This was followed by blood (28.3%), wound (10.1%), pleural fluid (7.1%), drainage fluid (3%), abscess (2%), urine (1%), peritoneal fluid (1%) and bile (1%).
Antimicrobial susceptibility profiles
Of the 99 S. maltophilia isolates, 90.9% were susceptible to TMP/SMX, 91.9% to levofloxacin, and 53.5% to ceftazidime. The susceptibility of the isolates to antibiotics is shown in Table 2 (Tab. 2).
Presence of integron-associated intI1, intI2, and intI3
In nine isolates (9.1%), intI1 was detected by PCR. All isolates were negative for intI2 and intI3. When evaluated together with the antibiotic susceptibility results, it was found that the intI1 gene was present in all TMP/SMX resistant isolates, and a statistically significant relationship was found between the presence of intI1 and TMP/SMX resistance (p<0.001). No such relationship was found between ceftazidime and levofloxacin resistance and intI1 positivity (Table 3 (Tab. 3)).
Presence of sul1, sul2, and sul3
In nine isolates (9.1%), sul1 was detected by PCR. These nine isolates were found to be identical to the isolates with intI1 and resistant to TMP/SMX. No isolates were positive for sul2 and sul3 by PCR.
Sequence analysis of the PCR products
Sequence analysis of the PCR products confirmed that the bands detected by PCR in nine isolates were intI1 and sul1.
PFGE analysis
According to PFGE analysis, 75 of the isolates were sporadic and 24 were found to be clonally related (similarity ≥90%). The clonally related isolates were collected in seven different clones (A–G), each containing 2–7 isolates (Table 4 (Tab. 4)).
Environmental samples
Environmental samples were collected from fiberbronchoscopes and washer-disinfectors, due to the detection of clustering in BALF samples in PFGE analysis. There was no growth of S. maltophilia in the cultures. However, P. a**eruginosa, Pseudomonas putida, and Enterococcus faecium were detected in the channel of one of the bronchoscopes; Achromobacter xylosoxidans was detected on the inner surface and in the rinse water of the washer-disinfector. No microorganism growth was observed in the samples taken after appropriate cleaning and disinfection processes.
Discussion
S. maltophilia is a multi-drug-resistant microorganism that can be isolated from many water-related environmental sources inside and outside hospitals and causes nosocomial infections with an increasing incidence [1]. S. maltophilia infections are more common in patients in ICUs than in the general population [4]. In a study evaluating S. maltophilia isolates collected from 24 participating university hospitals in Europe, it was reported that 41.5% of the isolates were obtained from ICU patients [15]. It has been reported that this rate can reach up to 70% [16]. In this study, 47.5% of the isolates were from patients hospitalized in ICUs. This can be explained by the fact that ICU patients have many risk factors reported for S. maltophilia infections, such as immunodeficiency, malignancy, chronic lung diseases, mechanical ventilation, indwelling catheters and similar devices, as well as the use of broad-spectrum antibiotics [17].
S. maltophilia is mainly associated with respiratory tract infections [17]. Among the pneumonia agents isolated from invasive respiratory tract specimens of patients hospitalized in 53 centers in the USA and Europe, S. m**altophilia was the sixth and ninth most frequently isolated microorganism, respectively [18]. Gulmez and Hascelik [7], in their study on 205 S. maltophilia isolates from 188 patients, isolated this microorganism with a frequency of 40%, 21.5%, and 13.2% from respiratory tract, blood, and pus samples, respectively. Juhasz et al. [16] reported that the most common sites of isolation for S. maltophilia in 100 patients with confirmed infection were ETA (31%), BALF (30%), blood (25%), and sputum (7%). In this study, S. maltophilia was most frequently isolated from respiratory tract samples (ETA 24.2%, BALF 17.2%, sputum 5.1%) and second-most frequently from blood samples (28.3%), which supports these findings.
The inherited resistance mechanisms of S. maltophilia to many antimicrobials cause problems in treatment. TMP/SMX is still accepted as the first-choice antimicrobial agent [3], [4], [17]. Analyzing the SENTRY Antimicrobial Surveillance Program data, Gales et al. [19] reported that the TMP/SMX susceptibility rates of 6467 S. maltophilia isolates collected globally between 1997–2016 showed little change over the years and was 95.6% overall. They reported the levofloxacin susceptibility as 81.5%. According to the data of the same surveillance program for the years 2014–2019, TMP/SMX, levofloxacin, and ceftazidime susceptibilities were reported as 95%, 79.6%, and 24%, respectively [20]. In comparison with these data, the susceptibility rate for TMP/SMX was lower (90.9%) and levofloxacin and ceftazidime susceptibility rates were higher (91.8% and 53.5%, respectively) in this study.
Determinating the resistance mechanisms of nosocomial pathogens and the identifying mobile genetic elements that play role in the transmission of resistance are important in terms of taking effective measures against these microorganisms. Most of the TMP/SMX resistance genes are located on transferable genetic elements. The sulfonamide resistance gene sul1 and the dfr genes responsible for trimethoprim resistance are often associated with class 1 integrons; sul2 and sul3, which are other sulfonamide resistance genes, were found to be mostly associated with plasmids and transposons [21]. Toleman et al. [5] investigated intI1, sul1, sul2, sul3, dfr genes, and ISCR elements in a total of 55 isolates, 25 of which were resistant to TMP/SMX and 30 of which were susceptible, collected from around the world, and detected sul1 in association with class 1 integrons in 17 of the TMP/SMX resistant isolates. sul2 was also shown in nine of the TMP/SMX resistant isolates, six of which were associated with ISCR2. Song et al. [22] tested 120 S. maltophilia isolates collected from three different university hospitals in Korea and found class 1 integrons in 17 of 28 sul1 positive isolates. However, ISCR2 and sul2 were not detected, and TMP/SMX resistant isolates were reported to carry sul1 and class 1 integrons significantly more frequently than did susceptible isolates. Kaur et al. [23] investigated intI1, intI2, intI3, sul1, and sul2 in 106 clinical isolates, and intI1 was detected in nine isolates, five of which were TMP/SMX resistant. They also reported that intI2 and intI3 were not found in any of the isolates. The co-existence of sul1 and sul2 genes was reported in two of the TMP/SMX resistant isolates, while the remaining 22 isolates carried either sul1 (10 isolates) or sul2 (12 isolates). In our study, intI1 and sul1 were detected together in all nine TMP/SMX resistant isolates, and these genes were not found in susceptible isolates. TMP/SMX MIC was >32/608 µg/mL for eight of the nine isolates, and 8/152 µg/mL for the remaining isolate. A significant relationship was found between TMP/SMX resistance and the presence of intI1, but a similar relationship could not be shown for ceftazidime and levofloxacin resistance. These results, in line with the findings of other researchers, indicate that the sul1 gene located in the 3'-conserved region of class 1 integrons has an important role in TMP/SMX resistance in S. maltophilia isolates. This situation poses a threat to the spread of resistance to TMP/SMX as a result of horizontal gene transfer and underlines that TMP/SMX resistance should be monitored together with its molecular mechanisms.
The problems arising in the treatment of S. maltophilia infections due to resistance problems increase the importance of epidemiological characterization of clinical strains. Various molecular typing methods, especially PFGE, were used to investigate the epidemiology of infections and nosocomial outbreaks due to this microorganism. In a study conducted in Spain, 132 clinical isolates from 105 hospitalized patients and seven environmental isolates were typed by using PFGE, and high genetic diversity was observed among isolates, despite originating from a single hospital. Five clones were identified that were claimed to be responsible for cross-transmission among patients, and it was noted that one S. maltophilia isolate from a fiberbronchoscope showed the same PFGE pattern as a clone containing respiratory isolates [24]. Neela et al. [25] typed 63 isolates in a tertiary hospital for one year and detected 59 different PFGE patterns. It was emphasized that there may be cross-transmission between wards due to the Isolation of strains with the same band profile from clinical samples of patients in different units. It was also underlined that continuous epidemiological monitoring is required besides antibiotic resistance surveillance, due to the potential for such spreads to occur with resistant isolates. Similarly, high genetic diversity was found among S. maltophilia isolates in our study and other studies using PFGE [26], [27]. This suggests the possibility that S. maltophilia may have been acquired from different sources as a result of its broad environmental distribution. Genetic diversity is also reported in studies using other molecular epidemiological methods, such as ERIC-PCR, rep-PCR, and MLST [7], [16], [28], [29], [30].
In this study, seven clones (A–G), each containing 2–7 isolates, were identified by PFGE analysis. This reveals the possibility of cross-transmission between patients or that these microorganisms were acquired from a common source, and underlines the importance of infection control measures in preventing the spread of multiresistant pathogens. This view was supported by studies reporting that the spread of S. maltophilia was limited with the help of the measures taken [31], [32], [33]. The increase in antibiotic resistance as a result of the clonal spread of resistant strains and subsequent treatment difficulties are serious problems in the treatment of infectious diseases. In this study, five of the nine TMP/SMX resistant isolates were in the same clone (clone E). The first isolate in this clone was from a wound sample of a patient in the infectious diseases clinic, and the other four were isolated from the bronchoalveolar lavage samples of patients in the thoracic surgery unit. The patient with the first isolate neither underwent bronchoscopy nor stayed in the thoracic surgery unit.
S. maltophilia can form biofilm and colonize medical instruments [34]. Cross-transmission and pseudoepidemics related to S. maltophilia have been reported in association with bronchoscopes [24], [35], [36]. In this study, clustering was observed in BALF samples according to PFGE results. The hospital infection control committee was informed and environmental samples were collected from fiberbronchoscopes and washer-disinfectors used by pulmonology and thoracic surgery units. However, there was no growth of S. maltophilia in the cultures. This situation might be due to the removal of S. maltophilia from the devices between the time of isolations from clinical samples and the time of environmental sampling. However, P. aeruginosa, P. putida, A. xylosoxidans, and E. faecium growth were detected in environmental cultures and it was decided to re-evaluate the disinfection process of the fiberbronchoscopes. In the following period, no bacterial growth was observed. This suggests that fiberbronchoscopes may also have been contaminated with S. maltophilia, resulting in pseudo-outbreaks, or infections in patients with predisposing factors.
Conclusions
As an opportunistic pathogen, S. maltophilia can cause nosocomial infections, and its intrinsic antimicrobial resistance limits treatment options. Therefore, it is necessary to monitor the resistance of S. maltophilia to antimicrobials that can be used in treatment, especially TMP/SMX. The findings of our study demonstrated that the sul1 gene, which is carried by class 1 integrons and therefore has the potential for horizontal transmission, plays an important role in TMP/SMX resistance in S. m**altophilia isolates. In order to minimize the spread of resistant pathogens such as S. maltophilia in the hospital setting, there is a need for accurate and complete implementation of infection control measures and sterilization-disinfection procedures. Hence, molecular epidemiological studies are of great importance in the development of preventive strategies by investigating the transmission routes of nosocomial pathogens and in monitoring the effectiveness of infection control measures.
Notes
Funding
This study was supported financially by Erciyes University Scientific Research Projects Unit with the project code TTU-2015-5034.
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Erciyes University (07.02.2014/2014/74). Informed consent was obtained from all individual participants or their legal guardians.
Authors’ ORCID
- Ömür Mustafa Parkan: 0000-0002-1071-4985
- Hüseyin Kiliç: 0000-0003-4885-4112
- Emine Alp: 0000-0003-0189-6008
- Demet Timur: 0000-0002-2475-5956
- Aycan Gündogdu: 0000-0003-2806-8464
- Özlem Ünaldi: 0000-0002-5560-6558
- Riza Durmaz: 0000-0001-6561-778X
Competing interests
The authors declare that they have no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brooke JS Stenotrophomonas maltophilia: an emerging global opportunistic pathogen Clin Microbiol Rev Jan 201225124110.1128/CMR.00019-1122232370 PMC 3255966 · doi ↗ · pubmed ↗
- 2Sánchez MB Antibiotic resistance in the opportunistic pathogen Stenotrophomonas maltophilia Front Microbiol 30Jun 2015665810.3389/fmicb.2015.0065826175724 PMC 4485184 · doi ↗ · pubmed ↗
- 3Looney WJ Narita MMühlemann K Stenotrophomonas maltophilia: an emerging opportunist human pathogen Lancet Infect Dis May 20099531232310.1016/S 1473-3099(09)70083-019393961 · doi ↗ · pubmed ↗
- 4Chang YT Lin CY Chen YH Hsueh PR Update on infections caused by Stenotrophomonas maltophilia with particular attention to resistance mechanisms and therapeutic options Front Microbiol 2Sep 2015689310.3389/fmicb.2015.0089326388847 PMC 4557615 · doi ↗ · pubmed ↗
- 5Toleman MA Bennett PM Bennett DM Jones RN Walsh TR Global emergence of trimethoprim/sulfamethoxazole resistance in Stenotrophomonas maltophilia mediated by acquisition of sul genes Emerg Infect Dis Apr 200713455956510.3201/eid 1304.06137817553270 PMC 2725981 · doi ↗ · pubmed ↗
- 6Deplano A Denis O Rodriguez-Villalobos H De Ryck R Struelens MJ Hallin M Controlled performance evaluation of the Diversi Lab repetitive-sequence-based genotyping system for typing multidrug-resistant health care-associated bacterial pathogens J Clin Microbiol Oct 201149103616362010.1128/JCM.00528-1121813717 PMC 3187349 · doi ↗ · pubmed ↗
- 7Gülmez D Hasçelik G Stenotrophomonas maltophilia: antimicrobial resistance and molecular typing of an emerging pathogen in a Turkish university hospital Clin Microbiol Infect Nov 2005111188088610.1111/j.1469-0691.2005.01257.x 16216102 · doi ↗ · pubmed ↗
- 8The Clinical and Laboratory Standards Institute (CLSI)Performance Standards for Antimicrobial Susceptibility Testing 202232 nd ed.Clinical and Laboratory Standards Institute