Case Report: An in-depth look into apocrine carcinoma of the axilla - a rare case presentation
Dr. Suhit Naseri, Samarth Shukla, Dr. Sourya Acharya, Sunita Vagha, Rehan Zahid, Dr. Suhit Naseri

TL;DR
This case report describes a rare instance of apocrine carcinoma in a 48-year-old man's axilla, highlighting the challenges in diagnosis and treatment due to the disease's rarity.
Contribution
The paper presents a new clinical case of apocrine carcinoma, contributing to the limited literature on this rare condition.
Findings
The patient was diagnosed with primary apocrine carcinoma after surgical excision of a right axillary mass.
The case highlights the difficulty in distinguishing apocrine carcinoma from other similar conditions due to overlapping histological features.
There are no established treatment standards for apocrine carcinoma due to its rarity and lack of clinical studies.
Abstract
Apocrine carcinoma is an extremely rare malignant cutaneous neoplasm that usually arises in areas with a high density of apocrine glands. Diagnosis can be challenging as tumours share histological and immunophenotypic characteristics with them. At first evaluation, the disease is often assumed to be benign. There have been approximately 100 reports of apocrine neoplasms in the literature. A 48-year-old male presented with a right axillary mass which increased in size over a period of 2 years. The patient was reported to have had ayurvedic therapy, but his swelling remained unchanged. Axillary lymph nodes were palpable. USG axilla suggested a well-defined fungating solid isoechoic lesion. USG neck did not reveal any abnormality. The mass was surgically excised as a whole by removing the overlying skin with margins and lymph node excision. The patient was diagnosed with primary apocrine…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2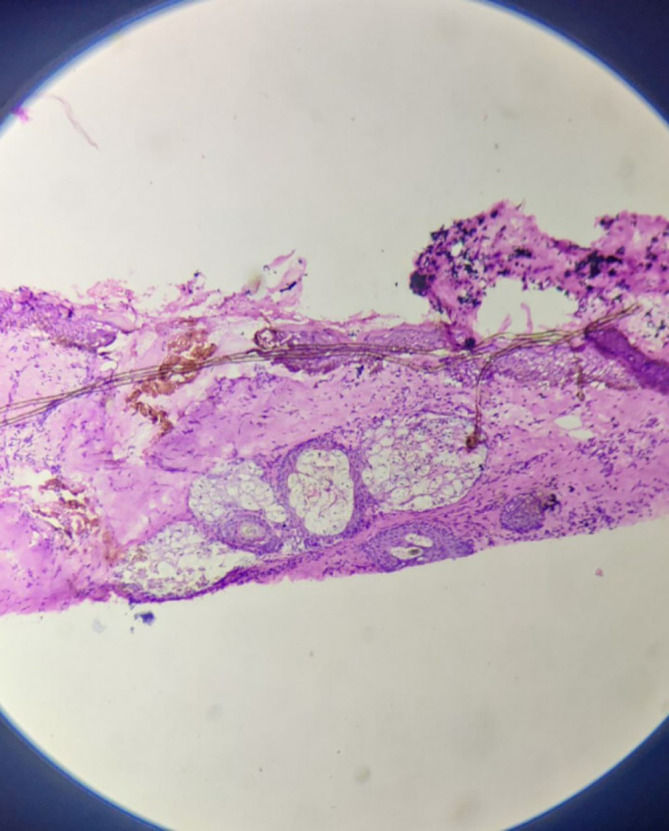 Figure 3
Figure 3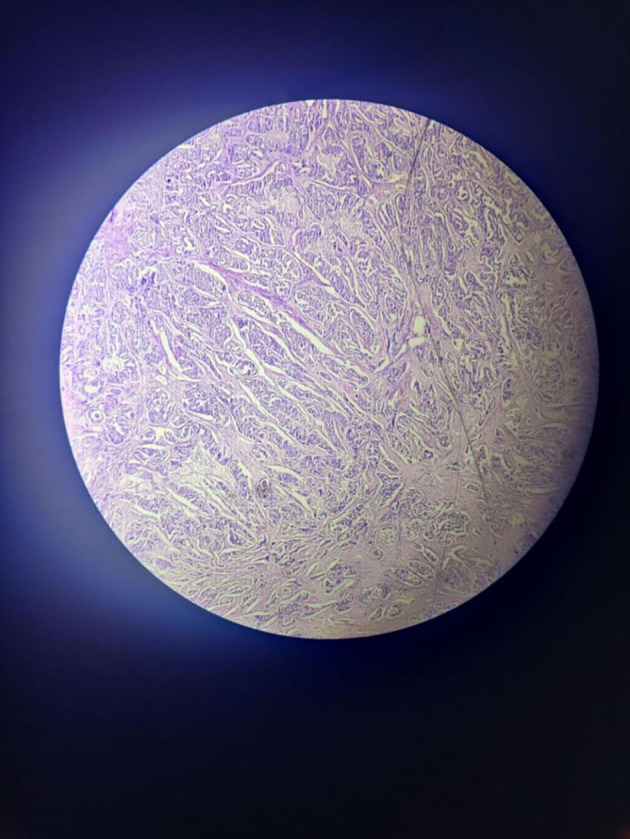 Figure 4
Figure 4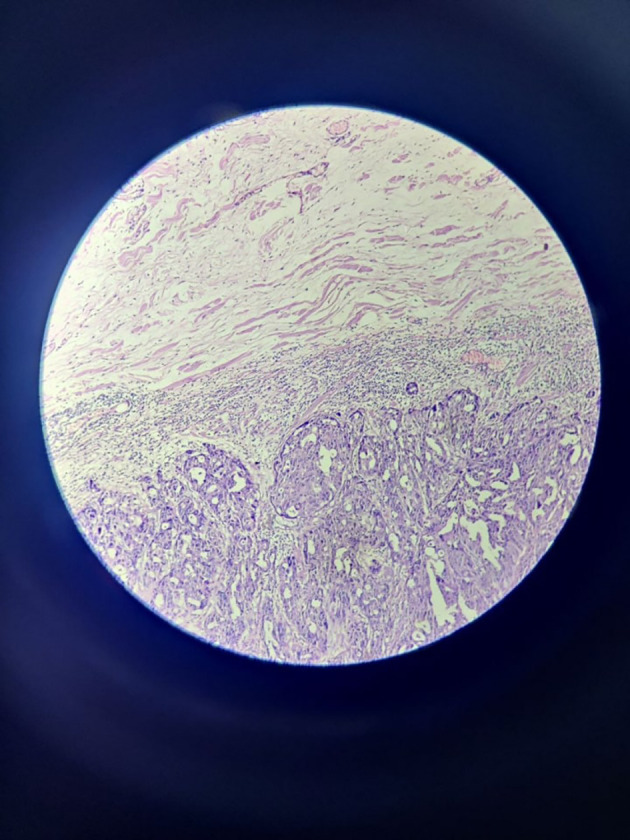 Figure 5
Figure 5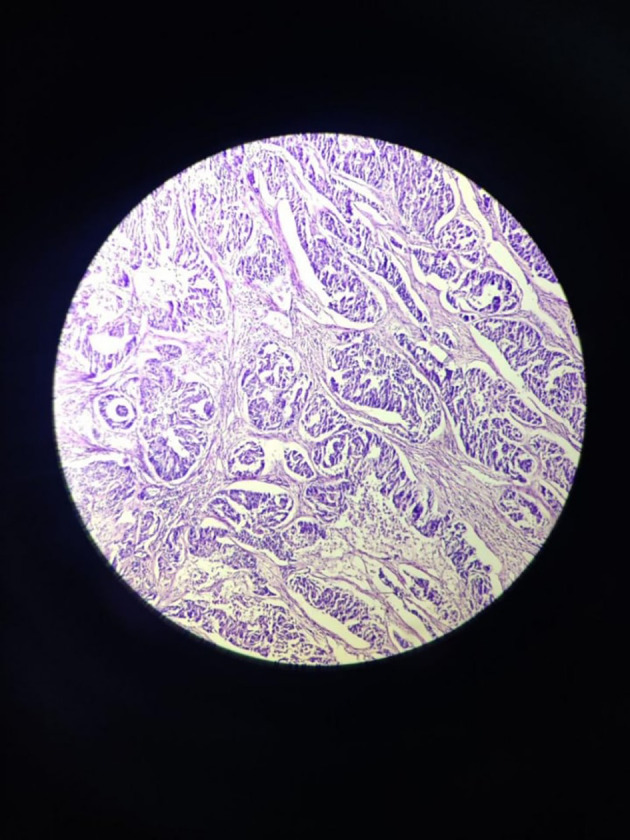 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer and Skin Lesions · Breast Lesions and Carcinomas · Nonmelanoma Skin Cancer Studies
Introduction
Apocrine carcinoma of the axilla is a seldom-seen form of breast cancer that originates in the axillary sweat glands. This disease has been reported to be an invasive ductal carcinoma subtype, the most prevalent form of breast cancer among women. From a surgical perspective, apocrine carcinoma of the axilla may present as a palpable mass or a non-palpable abnormality on imaging studies, such as mammography or ultrasound. Treatment typically involves surgical excision of the tumor with clear margins, which may be followed by radiation therapy and/or systemic chemotherapy depending on the stage and biology of the cancer. From a pathological standpoint, Large, pleomorphic cells with an abundance of eosinophilic cytoplasm and prominent nucleoli are seen in axillary apocrine carcinomas. Apocrine carcinoma of the axilla is uncommon, but it can still be a clinically relevant diagnosis that has to be treated promptly and effectively to provide the patient the best chance of survival.
Case report
In 2022, a case of a 48-year-old male of South Asian descent, working as a carpenter with an axillary mass presented to the surgery department with a lump in the axilla ( Figure 1) diagnosed as primary apocrine carcinoma after surgical excision. The patient presented with a right axillary mass with inflammation of the overlying skin, with occasional serosanguinous discharge which was associated with mild pain in the affected axilla. The patient was reported to have had ayurvedic therapy, but his swelling remained unchanged. The patient had no family history of malignancy. A physical evaluation and USG for both breasts did not find any abnormalities. USG of the right axilla suggested a well-defined solid isoechoic lesion with multiple microcalcifications with prominent vascularity. The mass increased in size over a period of 1 year and measured 8×8×2.3 cm.
Clinical image of right axillary mass with inflammation.
Seven axillary lymph nodes were isolated, the largest lymph node was measured to be 4×2×1.5 cm.
Grossly ( Figure 2), the tumour mass was white, firm in consistency and measured 4×4×3.5 cm. On the cut section, solid, homogenous blackish areas were identified with the involvement of overlying skin.
Gross image of excised specimen of axillary mass with a lymph node.
Microscopically, sections from superior, anterior and posterior margins showed unremarkable squamous lining epithelium with unremarkable deeper tissue and adnexal structure with few distended ducts of histopathology. Section from the inferior margin ( Figure 3) was positive for infiltration by malignant epithelial cells. Sections also show fibro-collagenous areas with minimal scattered inflammatory infiltrate. Sections from the tumour were also positive for perineural and lymphovascular invasion.
High power view of inferior surgical margin on frozen section – positive for infiltration by malignant cells.
Section from all seven lymph nodes shows histopathological features suggestive of metastatic deposits of epithelial malignancy.
The epidermis is visible in some portions of the tumour, which has a dermis with mostly papillary cystic architecture. Focal inflammation with numerous benign apocrine glands were noted.
The tumour with papillary architecture ( Figures 4– 6) was found to have fibrovascular cores lined by eosinophilic epithelial cells. The patient’s case was discussed in the hospital’s interdisciplinary tumour board and he was considered for adjuvant radiotherapy. A thorough follow-up plan was advised to the patient, but he did not follow through.
Tumor mass – scanner.
Tumor mass 10× – low power view.
Tumor mass - 40× – high power view.
Discussion
Apocrine carcinoma is an extremely uncommon adnexal malignancy with limited data on histologic prognostic factors and patient outcomes. ^ 1 ^ The axilla and adjacent medial upper arm are the most typical sites for apocrine carcinoma. ^ 2 ^ The tumour, which derives from pleuripotent adenexal cells capable of eccrine and follicular development, had first been discovered by Goldstein in 1982. ^ 3 ^ Reddish-purple subcutaneous nodules and solid or cystic masses are common characteristics of these tumours. Skin ulceration may be a comorbid condition, and they are frequently locally advanced when diagnosed. This tumour has a sluggish rate of growth, is locally invasive, and has the potential to spread to nearby lymph nodes, the lungs, the liver, the bone, and the brain. ^ 4 ^ At the time of diagnosis, lymph node metastases were present in over fifty per cent of all reported individuals suffering from apocrine carcinoma. The recommended treatment for these lesions is wide local excision. ^ 5 ^ Apocrine gland carcinomas and eccrine carcinomas are the two primary subtypes of sweat gland carcinomas. Apocrine carcinomas appear as hard, rubbery, cystic, solitary or numerous, non-tender masses with red to purple overlaying skin. Eccrine gland carcinomas lack distinguishing clinical characteristics, rendering gross examination diagnosis nearly difficult. They often only affect older individuals and present as quasi-tender, subcutaneous nodules. ^ 6 ^ Although the tumour often arises de novo, it can potentially result from previously present benign tumours like apocrine hyperplasia or apocrine adenoma. ^ 7 ^
Wide local excision is the preferred method of management of primary cutaneous ductal apocrine carcinoma. In addition to excision, chemotherapy as well as radiotherapy have been utilised, but they haven’t significantly reduced mortality or morbidity among patients with either localised or metastatic disease. The total number of reported instances and the amount of follow-up data that currently exists, both seem insufficient for determining the prognosis. Therefore, there is a need for further case accumulation.
Conclusion
The rare tumour referred to as apocrine carcinoma has a characteristic but non-specific histological appearance. For determining the prognosis and formulating particular therapy recommendations, the reported cases and follow-up data appear to be insufficient. Hence, additional cases needs to be collected.
Consent
Written informed consent for publication of their clinical details and clinical images was obtained from the patient.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Robson A Lazar AJF Ben Nagi J : Primary cutaneous apocrine carcinoma: a clinico-pathologic analysis of 24 cases. Am. J. Surg. Pathol. 2008;32(5):682–690. 10.1097/PAS.0b 013e 3181590 ba 4 18347508 · doi ↗ · pubmed ↗
- 2Dhawan SS Nanda VS Grekin S : Apocrine adenocarcinoma: case report and review of the literature. J. Dermatol. Surg. Oncol. 1990;16(5):468–470. 10.1111/j.1524-4725.1990.tb 00066.x 2341662 · doi ↗ · pubmed ↗
- 3Goldstein DJ Barr RJ Santa Cruz DJ : Microcystic adnexal carcinoma: a distinct clinicopathologic entity. Cancer. 1982;50(3):566–572. 10.1002/1097-0142(19820801)50:3<566::aid-cncr 2820500330>3.0.co;2-q 7093897 · doi ↗ · pubmed ↗
- 4Hollowell KL Agle SC Zervos EE : Cutaneous apocrine adenocarcinoma: defining epidemiology, outcomes, and optimal therapy for a rare neoplasm. J. Surg. Oncol. 2012;105(4):415–419. 10.1002/jso.22023 21913192 · doi ↗ · pubmed ↗
- 5Chamberlain RS Huber K White JC : Apocrine gland carcinoma of the axilla: review of the literature and recommendations for treatment. Am. J. Clin. Oncol. 1999;22(2):131–135. 10.1097/00000421-199904000-00005 10199445 · doi ↗ · pubmed ↗
- 6Mitts DL Smith MT Russell L : Sweat gland carcinoma: a clinico-pathological reappraisal. J. Surg. Oncol. 1976;8(1):23–29. 10.1002/jso.2930080104 1249938 · doi ↗ · pubmed ↗
- 7Miyamoto T Hagari Y Inoue S : Axillary apocrine carcinoma with benign apocrine tumours: a case report involving a pathological and immunohistochemical study and review of the literature. J. Clin. Pathol. 2005;58(7):757–761. 10.1136/jcp.2004.019794 15976347 PMC 1770727 · doi ↗ · pubmed ↗