Exome sequencing reveals biallelic inactivation of KMT2C in cutaneous apocrine carcinoma: A case report and review of the literature
Yui Hirano-Lotman, Yoshihiro Ishida, Yo Kaku, Seishi Ogawa, Kenji Kabashima

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
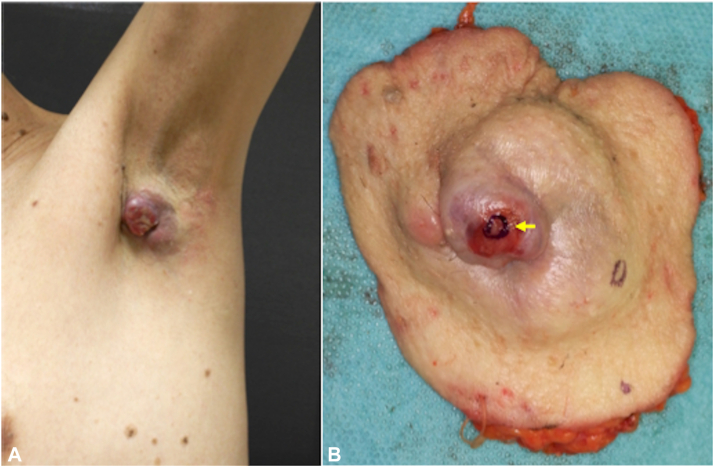 Figure 1
Figure 1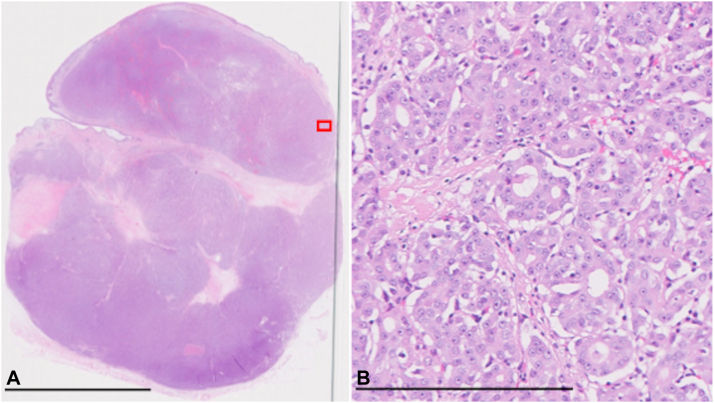 Figure 2
Figure 2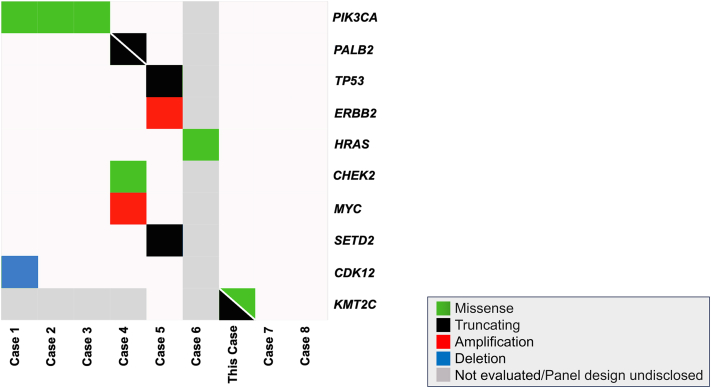 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer and Skin Lesions · Cancer Genomics and Diagnostics · Cancer-related Molecular Pathways
Introduction
Cutaneous apocrine carcinoma (CAC) is a rare adnexal tumor that typically manifests as a subcutaneous nodule or multinodular mass in regions abundant in apocrine glands, such as the axilla. CAC primarily affects individuals in their fifth or sixth decade of life without sexual or ethnic predilection.1 The diagnosis of CAC poses challenges due to histological and immunohistochemical similarities with breast cancer. Given its rarity, the genomic profile of CAC remains unclear. Here, we present the second CAC analyzed by whole-exome sequencing (WES).
Case report
A 66-year-old man was referred to our hospital with a painless subcutaneous mass in the left axilla (Fig 1, A). The mass, noticed 18 months prior, had gradually enlarged to approximately 5 cm in diameter. There was no family history of cancer, including breast cancer. A punch biopsy revealed adenocarcinoma located in the dermis, not involving the epidermis. Positron emission tomography scan detected left axillary lymph node metastases. Ultrasonography and magnetic resonance imaging did not detect accessory breast tissue in the bilateral axilla. A wide local excision with a 2-cm margin and left axillary lymph node dissection were performed (Fig 1, B). Histological examination revealed an infiltrating multinodular lesion with lymphovascular invasion located in the dermis and subcutaneous fat. There was no in situ lesion in the epidermis (Fig 2, A). The tumor was a poorly and moderately differentiated adenocarcinoma containing ductal and glandular structures. Atypical glandular cells displayed abundant eosinophilic cytoplasm. There were eosinophilic secretions in the glandular lumens (Fig 2, B). Immunohistochemically, the tumor cells were positive for AE1/AE3, GCDFP-15, ER (100%), PR (>95%), AR (100%), and HER2 (score2+), and negative for CK7, CK20, INSM1, and PSA. HER2 gene amplification was not detected with fluorescence in situ hybridization. Ki-67 index was 15.8%. A thorough histological examination of the surgical specimen did not detect precursor lesions or ectopic mammary tissue. The tumor was diagnosed as CAC. Seven of the 14 dissected axillary lymph nodes were positive for tumor cells. Adjuvant radiotherapy was administered with a total dose of 50 Gy in 25 fractions. During a 9-month follow-up, the patient showed no evidence of recurrence or metastases.Fig 1. Clinical photographs of cutaneous apocrine carcinoma. A, A 5 cm erythematous mass was present at the right axilla. B, The tumor was surgically removed with a 2-cm margin. A sample was excised from the surgical specimen, as indicated by the yellow arrow.Fig 2. Histological findings of the primary tumor of the right axilla. A, An overview of the central part of the tumor. The scale bar indicates 10 mm (×10). B, A high magnification view of the red rectangular area in (A). The scale bar indicates 250 μm (×400).
To clarify the mutational profile of CAC, we performed a WES analysis of the tumor dissected with laser-capture microdissection. The tumor mutational burden was 1.4 mutations/megabase. We detected 2 somatic mutations in KMT2C: a missense mutation, p.A4433P, and a nonsense mutation, p.Y2094X. Additionally, chromosome 5 gain and loss of heterozygosity of chromosome 11p were observed, but no gene mutations were identified in the affected regions. No other pathogenic mutations were detected.
Discussion
Genomic profiling of CAC meeting the 2018 World Health Organization classification criteria1 is limited to 8 cases (Fig 3, Table I).2, 3, 4, 5, 6, 7, 8 Among these, one utilized WES, identifying an ERBB2 amplification, a pathogenic TP53 mutation, and a likely pathogenic SETD2 mutation.5 The tumor was microsatellite stable, and the tumor mutational burden was 4 mutations/megabase.5 The remaining 7 cases employed targeted sequencing to analyze CACs; PIK3CA mutations were reported in 3 cases, PALB2 mutations were identified in 1 case, and an HRAS mutation in another case.2, 3, 4^,^6 No pathogenic mutations were detected in the other 2 cases.7^,^8 Notably, no recurrently mutated genes exist except for PIK3CA, suggesting an incomplete mutational landscape of CAC.Fig 3. The mutational landscape of cutaneous apocrine carcinoma. Mutation profiles of 9 cutaneous apocrine carcinoma cases, analyzed by whole-exome/targeted sequencing, are shown. Diagonal lines indicate multiple mutations.Table ISummary of cutaneous apocrine carcinomas analyzed by whole-exome/targeted sequencingCaseAuthorAge/sexSiteDrivergeneTypeAmino acidchangeMethod1Sasaki-Saito et al268 MAxillaPIK3CAMissensep.E726KFoundationOne CDxCDK12Deletion2Sasaki-Saito et al272 MAxillaPIK3CAMissensep.H1047RFoundationOne CDx3Imajima et al353 MAxillaPIK3CAMissensep.E545KFoundationOne CDx4Mäkelä et al445 M-PALB2Frameshiftp.L531fs∗30FoundationOne CDxFrameshiftp.F557fs∗18CHE**K2Missensep.I157TMYCAmplification5Nowicka-Matus et al565 MScrotumTP53Splicing (c.376-2A>G)Whole-exome sequencingSETD2Stopgainp.Q2292∗ERBB2Amplification6Scaranti et al642 FScalpHRASMissensep.G13RGeneRead custom DNA damage panel7DeCoste et al772 FScalpNoneTruSight Oncology 500 assay8Hibler et al860 MScalpNoneMSK-IMPACTThis case66 MAxillaKMT2CMissensep.A4433PWhole-exome sequencingStopgainp.Y2094X
We identified a missense and a nonsense mutation of KMT2C (Fig 3, Table I). KMT2C, which encodes an lysine methyltransferase, is frequently mutated in various human cancers, including bladder, lung, breast, endometrial, and head and neck cancers.9 The gene is also mutated in skin cancer as well as extramammary Paget disease.10 The most common mutation types in KMT2C are nonsense, followed by missense.11 Notably, the missense mutation was located in the plant homeodomain domain of KMT2C, a region where missense mutations of KMT2C are significantly enriched.11 Although the missense mutation we identified was not registered in the catalogue of somatic mutations in cancer database, these findings suggest that the missense mutation we observed is likely pathogenic. Considering the known role of KMT2C as a tumor suppressor gene in various tumor types, these 2 mutations likely result in the biallelic inactivation of KMT2C.11
In conclusion, our WES analysis has revealed a potential driver gene previously unreported in CAC and contributes to building the mutational landscape of CACs.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kazakov D.V.Argenyi Z.B.Brenn T.Apocrine carcinoma Elder D.E.Massi D.Scolyer R.A.Willemze R.WHO Classification of Skin Tumours 4th ed 2018 IARC Press 174175
- 2Sasaki-Saito N.Goto K.Aoki M.Apocrine carcinoma with marked sebocyte-like cytological features: a report of two cases J Cutan Pathol 512023929810.1111/cup.1453937743579 · doi ↗ · pubmed ↗
- 3Imajima T.Ito M.Shinohara Y.Favorable response to combined androgen blockade for metastatic cutaneous apocrine carcinoma: a case report Int J Surg Oncol 52020 e 1051 e 105510.1097/IJ 9.0000000000000105 · doi ↗
- 4MäkeläR.HärmäV.Badra Fajardo N.Ex vivo analysis of DNA repair targeting in extreme rare cutaneous apocrine sweat gland carcinoma Oncotarget 1220211100110910.18632/oncotarget.2796134084283 PMC 8169071 · doi ↗ · pubmed ↗
- 5Nowicka-Matus K.Salkus G.Sønderkær M.Scrotal Paget's Disease associated with human epidermal growth factor receptor 2-overexpressing metastatic apocrine carcinoma with complete response to paclitaxel, trastuzumab, and pertuzumab JCO Precis Oncol 72023 e 230017310.1200/PO.23.0017337595182 · doi ↗ · pubmed ↗
- 6Scaranti M.Nava Rodrigues D.Banerji U.Deep and sustained radiological response after MEK-RAF inhibition in HRAS mutant apocrine carcinoma of the scalp Eur J Cancer 122201991110.1016/j.ejca.2019.08.02331600639 · doi ↗ · pubmed ↗
- 7De Coste R.C.Carter M.D.Barnes P.J.Independent primary cutaneous and mammary apocrine carcinomas with neuroendocrine differentiation: report of a case and literature review J Cutan Pathol 4820211397140310.1111/cup.1408534152024 · doi ↗ · pubmed ↗
- 8Hibler B.P.Barker C.A.Hollmann T.J.Rossi A.M.Metastatic cutaneous apocrine carcinoma: multidisciplinary approach achieving complete response with adjuvant chemoradiation JAAD Case Rep 3201725926210.1016/j.jdcr.2017.03.00628580412 PMC 5447563 · doi ↗ · pubmed ↗