Association of Gout with Head and Neck Cancer: Longitudinal Follow-Up Studies Using a National Health Insurance Database in South Korea
So Young Kim, Il Hwan Park, Chun Sung Byun, Hyo Geun Choi, Mi Jung Kwon, Ji Hee Kim, Joo-Hee Kim, Chang Wan Kim

TL;DR
This study found that gout is linked to a higher risk of head and neck cancers, but the connection varies depending on the cancer type.
Contribution
The study provides new insights into the site-specific association between gout and head and neck cancer risk using a large national database.
Findings
Gout was associated with a 12% higher odds of head and neck cancer overall.
Oral cavity, oropharynx, and larynx cancers showed significantly higher odds in gout patients.
Nasal cavity/sinus, nasopharyngeal, and salivary gland cancers had lower odds in gout patients.
Abstract
Objective: Previous studies have reported controversial results on the association between gout and the risk of cancer. This study aimed to investigate the relationship between gout and the incidence of head and neck cancer (HNC). Methods: The data of participants who underwent health checkups in 2009 were analyzed using the National Health Insurance Database in South Korea. A total of 14,348 HNC patients and 57,392 control participants were analyzed for a prior history of gout. Overlap weighting was applied, and odds ratios (ORs) of gout for HNC patients were analyzed. The overlap-weighted model adjusted for demographic, socioeconomic, and lifestyle factors and comorbidities. HNC sites were classified as oral cavity cancer, oropharyngeal cancer, nasopharyngeal cancer, hypopharyngeal cancer, nasal cavity/sinus cancer, larynx cancer, or salivary gland cancer, and the ORs of gout were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
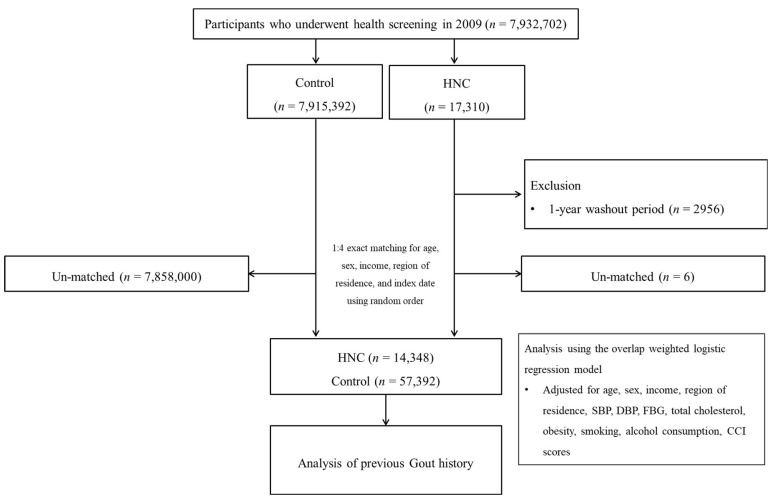 Figure 1
Figure 1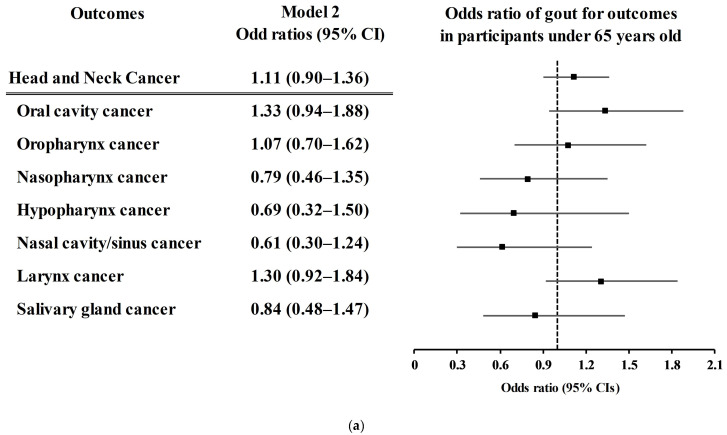 Figure 2
Figure 2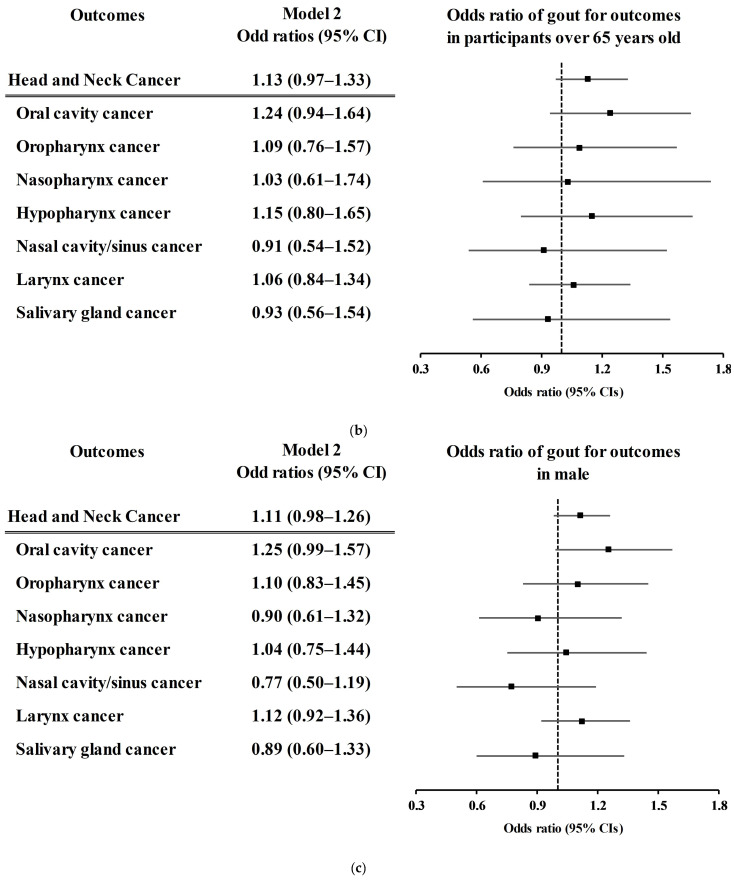 Figure 3
Figure 3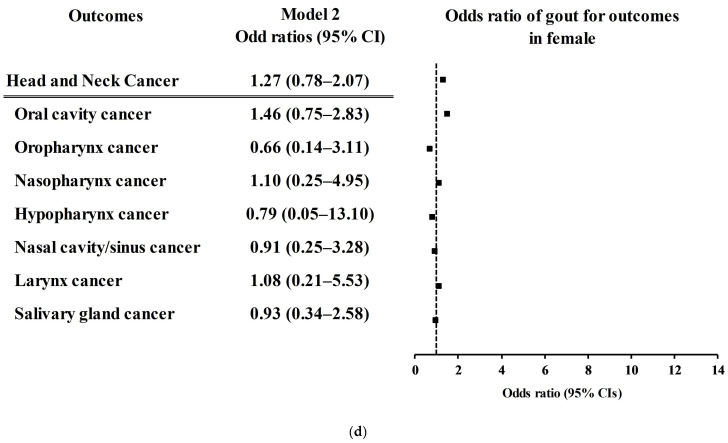 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGeochemistry and Geologic Mapping · Hydrocarbon exploration and reservoir analysis · Geological and Geophysical Studies
1. Introduction
Gout is a painful inflammatory arthritis caused by the formation of monosodium urate crystals in articular and nonarticular structures [1]. Approximately 1–4% of the worldwide population suffers from gout [2]. The prevalence of gout is greater in men than in women, with an estimated sex ratio of 3:1–10:1, and increases with age [2]. Long-term hyperuricemia can lead to the deposition of monosodium urate crystals, which in turn promote the activation of the NOD-like receptor protein 3 inflammasome and provoke gout flare [3]. Chronic inflammatory status and arthritis in gout patients may increase susceptibility to other diseases. Patients with gout have many comorbidities, such as hypertension, chronic kidney disease, and metabolic syndrome [2,4]. The bidirectional impact of uric acid, both antioxidant and pro-oxidant, can impose the risk of subsequent comorbidities in addition to the effect of inflammasome cascades initiated by monosodium urate crystals.
Several previous studies have reported the risk of cancer in patients with gout [5,6,7]. According to a nationwide health claim cohort study, patients with gout had a 1.053-fold greater risk of overall cancer (95% confidence intervals [CI] = 1.031–1.077) [5]. On the other hand, a few previous studies have reported no association between gout and the risk of cancer [8]. There was an additional risk of gastric cancer in the overall population and in secondary groups according to demographic factors and comorbidities [8]. Indeed, the risk of cancer related to the presence of gout is heterogeneous according to the type of cancer [5].
A prior study demonstrated that there was no association between gout and head and neck cancer (HNC). However, no prior study has analyzed the relationship between gout and HNC according to the site of cancer. In addition, because the risk of HNC is elevated in populations who smoke and consume alcohol, these lifestyle factors should be included in the analysis [9].
We hypothesized that the incidence of HNC could be greater in patients with gout. To test this hypothesis, we analyzed health claim data from patients with HNC in Korea with a previous history of gout. In addition, because there may be a specific association with gout according to the type of HNC, this study analyzed the HNC type and prior history of gout in each HNC subtype.
2. Methods
2.1. Ethics
The present study was permitted by the ethics committee of Hallym University (2021-02-004). The ethics committee exempted the requirement of written informed consent. This study was based on the National Health Insurance Database (NHID) in South Korea [10]. The NHID contains sociodemographic characteristics, health care utilization, dates of birth and death, and health screening.
2.2. Exposure and Outcomes
The history of gout was defined with the diagnosis of gout (ICD-10: M10) ≥ 2 times [11].
The history of head and neck cancer (HNC) (ICD-10: C00-C14, C300, C31–C32) with special certification for cancer (codes V193 and V194) was regarded as the history of HNC in this study.
In this study, we used ICD-10 codes to investigate the sites of the following eight types of head and neck cancer (HNC): oral cavity cancer (C00–C06), oropharynx cancer (C09–C10), nasopharynx cancer (C11), hypopharyngeal cancer (C12–C13), nasal cavity/sinus cancer (C300 and C31), laryngeal cancer (C32), and salivary gland cancer (C07–C08).
2.3. Participant Selection
For this study, we obtained a customized dataset of adults who underwent a health checkup in 2009 from the NHID in South Korea (n = 7,932,702). HNC participants were selected from the whole Korean population in the NHID from 2009 through 2021 (n = 17,310). The participants without history of HNC between 2009 and 2021 were control participants (n = 7,915,392). The HNC participants who were diagnosed in 2009 were removed (n = 2956). HNC participants and control participants were 1:4 matched for age, sex, income, and region of residence. Ultimately, 14,348 HNC participants and 57,392 control participants were enrolled in this study (Figure 1).
2.4. Covariables
This study included covariables of demographic, socio-economic, and lifestyle factors and comorbidities. Age was classified into 12 groups [12]. Tobacco smoking, alcohol consumption, and obesity according to BMI (body mass index, kg/m^2^) were categorized as described in our previous study [13]. Systolic blood pressure (SBP, mmHg), diastolic blood pressure (DBP, mmHg), fasting blood glucose (mg/dL), and total cholesterol (mg/dL) were measured parameters in the National Health Insurance system.
The Charlson Comorbidity Index (CCI) score was calculated [14,15]. This study excluded cancer and metastatic cancer patients from the CCI.
2.5. Statistics
The propensity score (PS) was estimated using multivariable logistic regression. HNC participants and control participants were applied the probability of PS and the probability of 1-PS, respectively. Overlap weighting was calculated [16,17].
The propensity score overlap-weighted logistic regression model was applied to estimate the overlap-weighted odds ratios (ORs) of gout for HNC patients. Additionally, the overlap-weighted ORs of gout for the site of HNC were analyzed. The age and sex subgroups were analyzed.
A p-value < 0.05 was considered as statistical significance. All analyses were conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
3. Results
Overall, 5.11% (733/14,348) of the HNC group and 4.66% (2674/57,392) of the control group had a previous history of gout (Table 1). The distributions of BMI group and smoking status; measurements of systemic blood pressure, diastolic blood pressure, fasting blood glucose, and total cholesterol; and CCI score differed between the HNC group and the control group. Thus, overlap-weighting adjustment was conducted. After overlap-weighting adjustment, 5.10% (577/11,300) of the HNC group and 4.60% (520/11,300) of the control group had a history of gout (sd = 0.02).
The odds of previous gout were 1.10-fold greater in the HNC group than in the control group according to the crude model (95% CI = 1.01–1.20, p = 0.024; Table 2). After overlap weighting, the odds of having gout for HNC patients were 1.12-fold greater in the HNC group (95% CI = 1.04–1.20, p = 0.002). Among the subtypes of HNC, oral cavity cancer had the greatest association with gout history (OR = 1.25, 95% CI = 1.16–1.34; p < 0.001). Oropharynx cancer and larynx cancer were also strongly associated with previous gout (OR = 1.08, 95% CI = 1.01–1.15, p = 0.029 for oropharynx cancer and OR = 1.12, 95% CI = 1.06–1.20, p < 0.001 for larynx cancer). On the other hand, nasal cavity/sinus cancer had the lowest odds of being related to a previous history of gout (OR = 0.78, 95% CI = 0.72–0.84; p < 0.001). Nasopharyngeal cancer and salivary gland cancer were also weakly associated with a previous history of gout (OR = 0.89, 95% CI = 0.83–0.96; p = 0.003 for nasopharyngeal cancer; OR = 0.88, 95% CI = 0.81–0.96; p = 0.002 for salivary gland cancer).
The associations of each type of HNC with previous gout history according to age and sex subgroup were analyzed (Figure 2 and Tables S1–S7). There was no association of previous gout history with the incidence of overall HNC, oral cavity cancer, oropharynx cancer, nasopharynx cancer, hypopharynx cancer, nasal cavity/sinus cancer, larynx cancer, or salivary gland cancer in any of the age or sex subgroups (Figure 2 and Tables S1–S7).
4. Discussion
A previous history of gout was related to a higher incidence of HNC in the Korean population. Oral cavity cancer had the strongest association with previous gout history, followed by laryngeal cancer and oropharynx cancer. On the other hand, nasal cavity/sinus cancer had a lower incidence in gout patients, followed by nasopharynx cancer and salivary gland cancer. This study improved upon previous findings by revealing an association between a history of prior gout and HNC, especially for each type of HNC.
Previous studies have shown that gout patients have a greater incidence of various types of cancer [5,18,19]. In a longitudinal population cohort study, patients with gout demonstrated an increased risk of esophageal cancer, stomach cancer, colon cancer, liver cancer, pancreatic cancer, lung cancer, ovarian cancer, renal cancer, and bladder cancer [5]. Another follow-up cohort study reported high hazard ratios for prostate cancer, bladder cancer, and renal cancer in patients with gout [19]. The potential risk of HNC in gout patients has shown mixed results in previous studies [5,18,19]. In a prospective cohort study, the incidence ratio of oral and pharyngeal cancer was 1.48–1.92 in patients with gout, although the confidence intervals were wide [18]. However, other longitudinal cohort studies did not show a high risk of HNC in patients with gout [5]. Because smoking and alcohol consumption are potent risk factors for HNC, the effects of these factors on the association between gout and HNC should be considered [20]. In the present study, we considered lifestyle factors, including smoking, alcohol consumption and socioeconomic factors, which are known to increase the risk of HNC [21,22].
Hyperuricemia in gout patients can mediate the high incidence of HNC in gout patients [23]. A meta-analysis demonstrated that the pooled risk for cancer incidence was 1.08 (95% CI = 1.04–1.12), and the risk of cancer mortality was 1.15 (95% CI = 1.05–1.26) [23]. A prospective study revealed that high serum uric acid increased the risk of mortality from cancer (adjusted hazard ratio = 1.41, 95% CI = 1.22–1.62) [24]. Hyperuricemia can be attributed to the high nucleic acid turnover and proliferation of cancer cells [24]. Moreover, chronic systemic inflammation in gout patients can impose a burden on the subsequent incidence of cancer.
On the other hand, nasal cavity/sinus cancer, nasopharyngeal cancer, and salivary gland cancer did not have a high incidence in gout patients in this study. The antioxidant effects of uric acid may be linked to the low risk of nasal cavity/sinus cancer, nasopharyngeal cancer, and salivary gland cancer in our cohort [25]. Uric acid scavenges reactive oxygen species (ROS) during its conversion to allantoin [25]. Furthermore, because a considerable portion of gout patients are prescribed allopurinol, the protective effects of allopurinol on cancer can lower the incidence of cancer in gout patients. In addition to lowering urate, allopurinol reportedly inhibits ROS, tumor necrosis factor alpha, and NLRP3 activities [26]. Thus, studies on the effects of gout and gout-related medications on the incidence of cancers can yield mixed results. For nasopharyngeal cancer, seropositivity for Epstein‒Barr virus (EBV) and exposure to some carcinogenic chemicals have crucial impacts on the incidence of this disease [27]. For nasal cavity cancer, exposure through the nasal cavity mucosa to carcinoid chemicals can increase the risk of incidence [28]. Therefore, the impacts of gout on the nasopharynx or nasal cavity can be diluted due to other potent risks, such as seropositivity to EBV and chemical exposure [29].
The present study analyzed data from a large, nationwide cohort. The large size of the study population permitted unbiased selection of the control population. In addition, we applied an overlap-weighted model to attenuate the confounding effects from covariables. However, because this study was based on national health claim codes, patients with subclinical cases or missed diagnoses who did not visit clinics were excluded. It was also possible that diagnostic codes could be registered incorrectly due to insufficient evaluation in clinics. In addition, the pathologic types, staging, and treatment options of HNC could not be included in the analyses [30,31,32]. The types, severity, and management of gout were also not considered in the present study. Although this study used a huge study population, the cases of specific locations of HNC could be too small to show the statistically significant relations. Because this study was based on a Korean population, the current results need to be interpreted with consideration of ethnic and geographic circumstances. Finally, we investigated the previous history of gout before the diagnosis of HNC, and we could not determine the causal relationship between gout and HNC. Further studies are warranted to address these limitations.
5. Conclusions
Patients with gout have greater odds of having HNC. Oral cavity cancer, oropharynx cancer, and larynx cancer were associated with a previous history of gout. On the other hand, nasal cavity/sinus cancer, nasopharyngeal cancer, and salivary gland cancer had lower incidences in gout patients. In the clinic, patients with gout need to be managed considering the potential risk of HNC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dalbeth N. Gosling A.L. Gaffo A. Abhishek A. Gout Lancet 20213971843185510.1016/S 0140-6736(21)00569-933798500 · doi ↗ · pubmed ↗
- 2Singh J.A. Gaffo A. Gout epidemiology and comorbidities Semin. Arthritis Rheum.202050 S 11S 1610.1016/j.semarthrit.2020.04.00832620196 · doi ↗ · pubmed ↗
- 3Liu Y.R. Wang J.Q. Li J. Role of NLRP 3 in the pathogenesis and treatment of gout arthritis Front. Immunol.202314113782210.3389/fimmu.2023.113782237051231 PMC 10083392 · doi ↗ · pubmed ↗
- 4Sandoval-Plata G. Nakafero G. Chakravorty M. Morgan K. Abhishek A. Association between serum urate, gout and comorbidities: A case-control study using data from the UK Biobank Rheumatology 2021603243325110.1093/rheumatology/keaa 77333313843 · doi ↗ · pubmed ↗
- 5Oh Y.J. Lee Y.J. Lee E. Park B. Kwon J.W. Heo J. Moon K.W. Cancer risk in Korean patients with gout Korean J. Intern. Med.20223746046710.3904/kjim.2020.25932872748 PMC 8925955 · doi ↗ · pubmed ↗
- 6Boustany A. Rahhal R. Mitri J. Onwuzo S. Zeid H.K.A. Asaad I. Increased Risk of Colorectal Cancer in Patients with Chronic Tophaceous Gout: A Population-Based Study Arq. Gastroenterol.20236033934410.1590/S 0004-2803.230302023-4337792763 · doi ↗ · pubmed ↗
- 7Kuo C.F. Luo S.F. See L.C. Chou I.J. Fang Y.F. Yu K.H. Increased risk of cancer among gout patients: A nationwide population study Jt. Bone Spine 20127937537810.1016/j.jbspin.2011.09.01122088929 · doi ↗ · pubmed ↗
- 8Kwon M.J. Han K.M. Kim J.H. Kim J.H. Kim M.J. Kim N.Y. Choi H.G. Kang H.S. Association between Gout and Gastric Cancer: A Nested Case-Control Study Using a National Health Sample Cohort J. Pers. Med.20241422910.3390/jpm 1403022938540972 PMC 10971149 · doi ↗ · pubmed ↗