Sex-Related Differences Between Patients Undergoing Surgery for Acute Type A Aortic Dissection
Baku Takahashi, Keiji Kamohara, Hiroyuki Morokuma, Junji Yunoki

TL;DR
This study found sex-related differences in patients undergoing surgery for aortic dissection, including age, symptoms, and surgical outcomes.
Contribution
The study identifies sex-specific differences in acute type A aortic dissection patients and suggests a sex-based management strategy.
Findings
Females were older and had longer time from onset to surgery compared to males.
Males had better long-term survival rates than females at 10 years.
Sex was not an independent predictor of early death after surgery.
Abstract
Introduction This study aimed to evaluate the sex-specific characteristics and surgical outcomes in patients with acute type A aortic dissection (ATAAD). Materials and methods We reviewed the surgical records of patients who underwent ATAAD repair at our institution between 2004 and 2020 (n=213). Results Of the 213 patients, 100 (46.9%) were male, and 113 (53.1%) were female. Males were younger than females (62.5 vs. 72.9 years, p<0.0001). Females had more nonspecific symptoms (p=0.04), more frequently developed ATAAD before noon (45.0% vs. 53.1%, p=0.01), and had a significantly longer time from onset to surgery (425.1 vs. 595.8 min, p=0.03). The ascending aorta was replaced more frequently in females than in males (54.5% vs. 72.8%, p<0.01). No significant difference was observed in the in-hospital mortality rate between males and females (9.0% vs. 10.6%, p=0.69). The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
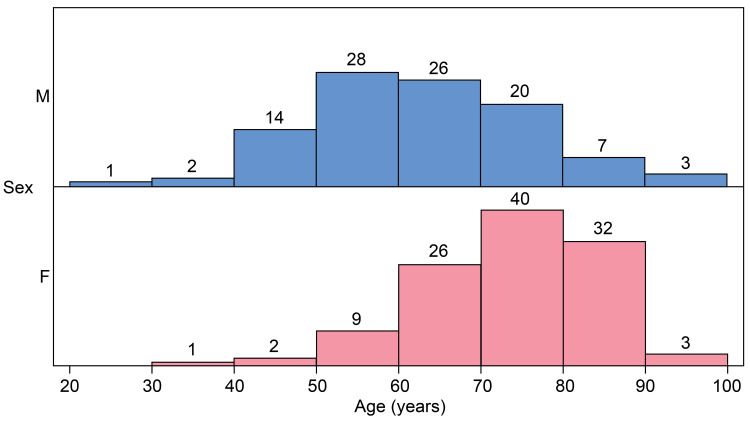 Figure 1
Figure 1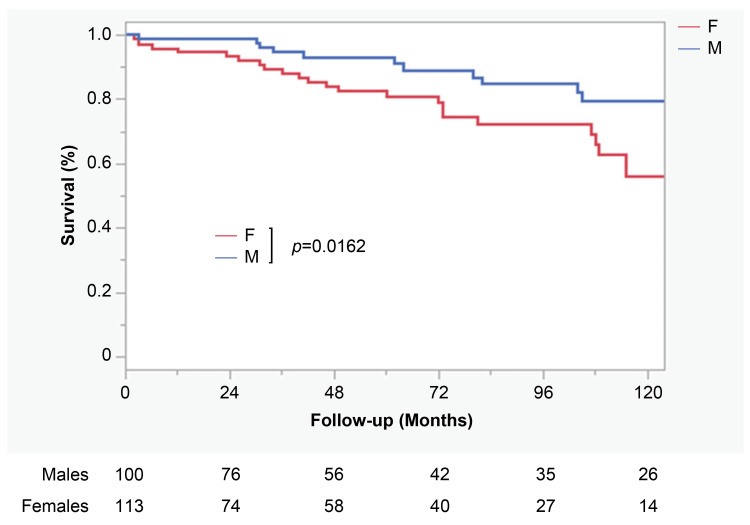 Figure 2
Figure 2| Total cohort (n=213) | |||
| Admission variables | Males | Females | p-value |
| Number of patients (%) | 100 (46.9) | 113 (53.1) | |
| Patient age (y) | 62.5 ± 13.4 | 72.9 ± 10.7 | <0.0001 |
| Hypertension, n (%) | 65 (65.0) | 91 (80.5) | 0.0106 |
| Diabetes, n (%) | 7 (7.0) | 5 (4.4) | 0.4159 |
| Chronic AF, n (%) | 1 (1.0) | 5 (4.4) | 0.2183 |
| History of CAD, n (%) | 6 (6.0) | 6 (5.3) | 0.8274 |
| History of CVD, n (%) | 8 (8.0) | 19 (16.8) | 0.0537 |
| History of open-heart surgery, n (%) | 8 (8.0) | 0 | 0.0020 |
| Creatinine on admission (mg/dL) | 1.2 ± 1.1. | 1.2 ± 1.4 | 0.9955 |
| Hemodialysis, n (%) | 1 (1.0) | 4 (3.5) | 0.3738 |
| Chronic lung disease, n (%) | 14 (14.0) | 1 (0.9) | 0.0002 |
| Marfan syndrome, n (%) | 1 (1.0) | 0 | 0.4695 |
| Initial symptom of chest/back pain, n (%) | 73 (73.0) | 68 (60.2) | 0.0483 |
| Shock, n (%) | 19 (19.0) | 34 (30.1) | 0.0617 |
| Tamponade, n (%) | 13 (13.0) | 22 (19.5) | 0.2035 |
| Cardiopulmonary arrest before admission, n (%) | 3 (3.0) | 4 (3.5) | 1.0000 |
| AR ≥ moderate, n (%) | 9 (9.0) | 6 (5.3) | 0.2935 |
| Acute neurological complication, n (%) | 10 (10.0) | 13 (11.5) | 0.7240 |
| Malperfusion syndrome, n (%) | 4 (4.0) | 10 (8.9) | 0.1540 |
| Patients referred, n (%) | 70 (70.0) | 84 (74.3) | 0.4803 |
| Diagnosed at our hospital, n (%) | 60 (60.0) | 71 (62.8) | 0.6716 |
| Time from admission to surgery, min | 197.0 ± 167.9 | 183.1 ± 158.6 | 0.5360 |
| Time from onset to surgery, min | 425.1 ± 257.1 (n=97) | 595.8 ± 768.7 (n=100) | 0.0391 |
| Onset (am) | 45 (45.0) (n=97) | 60 (53.1) (n=100) | 0.0101 |
| Season, n (%) | 0.1144 | ||
| Spring | 26 (26.0) | 25 (22.1) | |
| Summer | 21 (21.0) | 12 (10.6) | |
| Fall | 24 (24.0) | 37 (32.7) | |
| Winter | 29 (29.0) | 39 (34.5) | |
| IMH, n (%) | 13 (13.0) | 22 (19.5) | 0.363 |
| Neck vessel dissection, n (%) | 34 (34.0) | 38 (33.6) | 0.9449 |
| Innominate dissection, n (%) | 39 (50.0) | 41 (47.7) | 0.766 |
| RCC dissection, n (%) | 26 (33.3) | 29 (33.7) | 0.9581 |
| RC dissection, n (%) | 8 (10.3) | 7 (8.1) | 0.6386 |
| LCC dissection, n (%) | 21 (26.9) | 22 (25.6) | 0.8453 |
| LC dissection, n (%) | 15 (19.2) | 6 (7.0) | 0.019 |
| Dissection extent, n (%) | 0.0045 | ||
| Ascending | 3 (3.9) | 4 (4.7) | |
| Arch | 6 (7.7) | 15 (17.4) | |
| Descending | 7 (9.0) | 20 (23.3) | |
| Abdominal | 21 (26.9) | 22 (25.6) | |
| Iliac | 41 (52.6) | 23 (26.7) | |
| Unknown | 0 | 2 (2.3) | |
| Entry, n (%) | 0.0018 | ||
| Ascending | 43 (43.0) | 76 (67.3) | |
| Arch | 36 (36.0) | 28 (24.8) | |
| Descending | 11 (11.0) | 3 (2.7) | |
| Unknown | 10 (10.0) | 6 (5.3) | |
| Total cohort (n=213) | |||
| Admission variables | Males (n=100) | Females (n=113) | p-value |
| AAR or hemiarch replacement | 55 (55.0) | 83 (73.5) | 0.0049 |
| Partial arch replacement | 2 (2.0) | 4 (3.5) | 0.6866 |
| Total arch replacement | 43 (43.0) | 26 (23.0) | 0.0019 |
| Artery cannulation site | |||
| Axillary artery | 3 (3.0) | 8 (7.1) | 0.1794 |
| Femoral artery | 63 (63.0) | 76 (67.3) | 0.5150 |
| Axillary and femoral artery | 34 (34.0) | 27 (23.9) | 0.1035 |
| Ascending aorta | 1 (1.0) | 0 | 0.4695 |
| Entry closure | 80 (79.2) | 105 (92.1) | 0.0065 |
| Frozen elephant trunk | 22 (22.0) | 10 (8.9) | 0.0073 |
| Aortic root plasty or replacement | 13 (13.0) | 3 (2.7) | 0.0043 |
| Concomitant procedures | 12 (12.0) | 20 (17.7) | 0.2453 |
| CABG | 7 (7.0) | 13 (11.5) | 0.2607 |
| AVR | 1 (1.0) | 0 | 0.4695 |
| Peripheral bypass | 3 (3.0) | 3 (2.7) | 1.0000 |
| Others | 2 (2.0) | 7 (6.2) | 0.1778 |
| Operative time | 447.4 ± 157.6 | 398.4 ± 122.1 | 0.0114 |
| CPB time (min) | 220.7 ± 71.7 | 194.9 ± 54.9 | 0.0033 |
| CA time | 41.6 ± 15.1 | 39.6 ± 8.9 | 0.2247 |
| ACP, n (%) | 68 (68.0) | 77 (68.1) | 0.9824 |
| ACP time | 50.0 ± 46.9 | 37.7 ± 38.7 | 0.0366 |
| Rectal minimum temperature | 22.7 ± 2.9 | 23.0 ± 2.7 | 0.4414 |
| Intraoperative RBC units | 9.2 ± 11.5 | 9.4 ± 6.9 | 0.8604 |
| Intraoperative FFP units | 17.9 ± 13.1 | 17.2 ± 12.5 | 0.7100 |
| Intraoperative platelets units | 16.3 ± 10.9 | 15.0 ± 9.7 | 0.3954 |
| Total cohort (n=213) | |||
| Admission variables | Males (n=100) | Females (n=113) | p-value |
| Reoperation for bleeding | 6 (6.0) | 5 (4.4) | 0.6042 |
| New-onset CVD | 10 (10.0) | 15 (13.3) | 0.4587 |
| Reintubation | 8 (8.0) | 12 (10.6) | 0.5130 |
| Tracheostomy | 8 (8.0) | 17 (15.0) | 0.1109 |
| Requiring transient dialysis | 10 (10.1) | 10 (9.2) | 0.8209 |
| Requiring permanent dialysis | 0 | 2 (1.8) | 0.4987 |
| Sepsis | 4 (4.0) | 4 (3.5) | 1.0000 |
| Malperfusion | 3 (3.0) | 10 (8.9) | 0.0751 |
| ICU stay, d | 6.0 ± 6.3 | 8.8 ± 11.3 | 0.0299 |
| Ventilator >3 d | 43 (43.0) | 48 (42.5) | 0.9387 |
| Hospital stay, d | 35.8 ± 40.5 | 40.0 ± 60.3 | 0.5587 |
| 30-day mortality | 7 (7.0) | 6 (5.3) | 0.6071 |
| In-hospital mortality | 9 (9.0) | 12 (10.6) | 0.6923 |
| Multivariable analysis | |||
| Admission variables | Odds ratio | 95% Confidence interval | p-value |
| For all patients | |||
| Age | 1.10 | 1.02-1.1 | 0.0157 |
| Preoperative acute neurological complication | 7.74 | 1.28-46.6 | 0.0255 |
| Malperfusion syndrome | 12.0 | 1.96-73.8 | 0.0072 |
| Operation time | 1.01 | 1.00-1.02 | 0.0002 |
| Male | 0.96 | 0.18-5.21 | 0.9645 |
| For males | |||
| Preoperative acute neurological complication | 12.5 | 1.23-122.1 | 0.0302 |
| Operative time | 1.01 | 1.01-1.02 | 0.0003 |
| For females | |||
| Malperfusion syndrome | 32.9 | 6.46-163.4 | <0.0001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic Disease and Treatment Approaches · Aortic aneurysm repair treatments · Cardiac, Anesthesia and Surgical Outcomes
Introduction
The effects of sex differences on surgical outcomes have been widely deliberated. In the field of cardiac surgery, female sex is an independent risk factor for mortality in coronary artery bypass surgery [1,2] and mitral valve surgery [3,4]. Acute type A aortic dissection (ATAAD) is a life-threatening thoracic cardiac condition. Studies investigating sex differences in ATAAD have reported various findings, with many indicating no significant disparity in mortality rates between males and females and none identifying sex as a risk factor for mortality [5-9]. Some recent reports have indicated that the mortality rate is higher for males [10], whereas others have indicated that females have higher rates [11]; thus, no definitive conclusions have been reached yet.
Considering that the mortality rate of ATAAD increases by 1%-2% per hour, up to two days after onset [12], understanding the sex-specific differences during the period from symptom onset to surgery and the influencing initial symptoms becomes imperative for diagnosis. Furthermore, it would be beneficial for surgeons to understand the differences in the type, extension of the dissection, and location of the primary entry because the surgical procedures can vary depending on these findings [13-15]. However, few studies have delved into these aspects, and previous studies were limited by shorter follow-up periods. Thus, this study aimed to clarify the sex-specific differences in preoperative patient characteristics and both short- and long-term outcomes of ATAAD at our institution, making it the first study to report the differences between males and females in the period from onset to surgery and the location of primary entry in ATAAD.
Materials and methods
Study design and participant selection
In this retrospective study, we enrolled patients with ATAAD who underwent surgery at Saga University Hospital (Saga, Japan) between January 2004 and December 2020. One patient diagnosed with iatrogenic ATAAD was excluded. All data were collected from medical records and telephone surveys.
Surgery
Our surgical strategy for ATAAD has been described [16]. All operations were performed using a median sternotomy with standard cardiopulmonary bypass (CPB). The attending surgeons determined the cannulation sites and numbers. Brain protection was performed with antegrade and/or retrograde cerebral perfusion under hypothermic conditions, at the discretion of the attending surgeons. The primary entry was mostly resected, and the extent of the aortic surgery was individualized based on patient-specific considerations.
Statistical analysis
The JMP software (version 16.0; SAS Institute, Cary, NC, USA) was used for all statistical analyses. Differences between groups for continuous data were expressed as mean ± standard deviation using unpaired student’s t-test. Categorical variables were expressed as frequencies and percentages using the χ^2^ test or Fisher’s exact test.
A Kaplan-Meier survival curve and log-rank test assessed the rate of freedom from death. Binomial logistic regression analysis was performed to determine the independent predictors of in-hospital mortality. The variables used for the multivariate model were the clinical variables listed in Tables 1, 2, in addition to male and female sex, which were identified using a forward stepwise approach with a cut-off p-value for inclusion and exclusion of 0.1. p-values <0.05 were considered significant for all analyses.
Results
Preoperative data
Of the 213 patients with ATAAD who were included in the study, 100 (46.9%) were males and 113 (53.1%) were females. Female patients were significantly older than male patients (62.5 ± 13.4 vs. 79.2 ± 10.7 years; p<0.001) (Figure 1). Hypertension was significantly more common in females, whereas chronic respiratory failure and a history of cardiac surgery were more frequently observed in males. Although no significant difference was observed, females were more likely to present with shock than males (19.0% vs. 30.1%, p=0.0617). Females were less likely to develop ATAAD in the summer than males (21.0% vs. 10.6%, p=0.1144). Limited data showed that the onset of symptoms before noon was more common in females than in males (45.0% vs. 53.1%, p=0.0101). Females had significantly less thoracic back pain at onset than males (73% vs. 60.2%, p=0.0483). They also had a significantly longer time from disease onset to surgery than males (p=0.0391). However, the transfer rate did not differ between males and females.
Relationship between age and sex in acute type A aortic dissectionM: males, F: females.
Imaging findings
Approximately 80% of males had dissections extending to the abdominal aorta, whereas half of females had dissections remaining in the thoracic aorta (p=0.0045). Although no difference was noticed between dissection of the brachiocephalic, right common carotid, right subclavian, and left common carotid arteries, the left subclavian artery was more frequently dissected in males (19.2% vs. 7.0%, p=0.019). Additionally, no significant difference was observed in false lumen thrombosis between the two groups (13.0% vs. 19.5%, p=0.363). The primary entry point in the ascending aorta was more common in females (43.0% vs 67.3%; p=0.0018).
Intraoperative data
Significant differences in aortic procedures were observed between the sexes. Females underwent ascending aortic replacement more often (55.0% vs. 73.5%, p=0.0049), whereas total arch replacement was more frequently performed in males (43.0% vs. 23.0%, p=0.0019). The frozen elephant trunk technique was used more frequently in males than in females (22.0% vs. 8.9%, p=0.0073). Furthermore, males were more likely to undergo aortic root interventions than females (13.0% vs. 2.7%, p=0.0043). Surgery and cardiopulmonary bypass times were significantly longer in male patients, although the circulatory arrest time was similar in both sexes. Entry closure was more common in females than in males (79.2% vs. 92.1%, p=0.0065), and there were no differences in the number of intraoperative blood transfusions (Table 2).
Postoperative data
No significant difference was observed in in-hospital mortality rates between sexes (9.0% vs. 10.6%, p=0.6923). The incidences of neurological complications and sepsis were similar in females and males; however, malperfusion was more common in females (3.0% vs. 8.9%, p=0.0751). As seen in Table 3, males had shorter ICU lengths of stay (6.0 ± 6.3 vs. 8.8 ± 11.3 days, p=0.0299). In the logistic regression analysis, the risk factors for in-hospital mortality were age (odds ratio (OR), 1.10; 95% confidence interval (CI), 1.02-1.10; p=0.0157), preoperative neurological complications (OR, 7.74; 95% CI, 1.28-46.6; p=0.0255), malperfusion syndrome (OR, 12.0; 95% CI, 1.96-73.8; p=0.0072), and operation time (OR, 1.01; 95% CI, 1.00-1.02; p=0.0002). Male sex did not influence in-hospital mortality (OR, 0.96; 95% CI, 0.18-5.21; p=0.9645). Risk factors specific to males were preoperative neurological complications (OR, 12.5; 95% CI, 1.23-122.1; p=0.0302) and operative time (OR, 1.01; 95% CI, 1.01-1.02; p=0.0003). As highlighted in Table 4, a risk factor specific to females was malperfusion syndrome (OR, 32.9; 95% CI, 6.46-163.4; p<0.0001). The unadjusted long-term survival was significantly higher in males than in females (p=0.0162). At 10 years, males had significantly better long-term survival rates in the unadjusted cohort (79.4% vs. 55.9%, p=0.02) (Figure 2).
Unadjusted cohort long-term survival rate for all patients with log-rank test comparing males with femalesM: males, F: females.
Discussion
Our findings revealed no significant differences in hospital mortality based on sex when comparing perioperative characteristics and surgical outcomes between females and males undergoing open aortic repair for ATAAD. However, females had significantly lower long-term survival rates than males in the unadjusted cohort. In addition, this study highlighted several important differences between females and males undergoing ATAAD repair; specifically, females were older at the onset of ATAAD and presented with fewer DeBakey type I dissections. They also had a higher incidence of onset before noon, presented more non-specific symptoms, and had a longer duration from onset to surgery. Furthermore, preoperative shock and malperfusion syndrome were more common in females than in males. Overall, female patients underwent more ascending replacements and fewer aortic root replacements.
In the absence of surgical intervention, ATAAD increases mortality by 1%−2%/hour by the second day after onset [12]. Therefore, early diagnosis and treatment should be performed to improve outcomes [17]. Our study revealed that females have a significantly longer time to intervention from onset than males. The reason for this prolonged intervention duration in female patients remains unclear. One plausible explanation could be the difference in the initial symptoms between males and females. Although few studies have focused on differences in symptoms, Nienaber et al. reported that females exhibited nonspecific early symptoms of ATAAD compared to males [18]. Consistent with their findings, our study showed that symptoms other than chest and back pain were significantly more common in females, thus potentially contributing to delayed diagnosis. Emergency and primary care physicians should be aware that approximately 40% of females with ATAAD present with nonspecific symptoms. Furthermore, many offer a rational explanation for the sex difference in onset time. In our study, females were more likely than males to develop ATAAD before noon. Although we did not investigate the specific hours of onset, it is widely acknowledged that clinical outcomes tend to deteriorate during nighttime hours due to a lack of inexperienced staff, or alternatively, hospital access may be adversely affected at night [19,20]. These sex-specific differences can result in prolonged intervention times and a poor preoperative status for female patients, since ongoing ATAAD-induced hemodynamic instability progressively worsens and causes serious complications, such as shock and malperfusion [9]. Our study also identified malperfusion syndrome as a risk factor of in-hospital mortality specific to females. Therefore, efforts aimed to shorten the time until intervention may improve survival rates in females [9,18].
Our findings revealed differences in the location of the primary entry site of ATAAD between males and females, with approximately two-thirds of females having the primary entry site in the ascending aorta. Furthermore, DeBakey type I was more common in males, whereas type II was more common in females. These differences led to increased female ascending aorta replacements using our entry-oriented strategy. Aortic root interventions were performed more frequently in males than in women, which is consistent with the results of a previous study [5-11]. However, such root interventions increase operation and cardiopulmonary bypass times, which can lead to increased mortality [21-23]. In our study, an increased operative time was a male-specific risk factor for early mortality. Current guidelines [24] dictate that aortic interventions are determined by the diameter of the aorta regardless of sex, which may result in disproportionately excessive interventions in males. It would seem favorable to focus more on sex-specific normal aortic diameters [5] and we should make a decision after careful consideration in adopting extensive aortic surgery for males with ATAAD.
Surgical mortality did not differ significantly between the sexes (9.0% vs. 10.6%, p=0.6923). However, our study demonstrated that females had lower long-term survival rates than males in the unadjusted cohort, which is inconsistent with previous reports [6,10,11]. This difference can be attributed to the age of the patient population. Unlike many other studies, our study included many elderly patients, and the multivariate analysis identified age as a risk factor for in-hospital mortality. Prior reports have shown that females develop aortic dissection at an older age than males because of the progression of arteriosclerosis caused by decreased estrogen levels [25,26]. Given this fact, it seems natural that the long-term survival rates were lower in females than in males. Previous studies have shown that surgery can be performed safely in elderly and younger patients with ATAAD [27,28]. Therefore, even though females with ATAAD may be older and exhibit poorer preoperative conditions than males, treatment strategies should not be based on sex considerations.
Limitations
This study had some limitations. Firstly, this study was conducted at a single center in Japan. The findings of this study cannot be generalized because the expertise of surgeons, the number of people, and the volume of procedures vary depending on the facility. In addition, our study included only patients who survived surgery and excluded those who died before the procedure. This exclusion criterion might introduce a potential bias in our analysis due to an underrepresentation of cases with more severe conditions or higher mortality risks. Lastly, the small sample size may have been insufficient to detect subtle differences.
Conclusions
Several differences were found between females and males who underwent ATAAD repair. Females had more nonspecific symptoms and a longer intervention time than males. Notably, malperfusion syndrome emerged as a specific risk factor for in-hospital mortality in females; thus, shorter interventions are recommended for female patients. Conversely, males underwent more extensive surgeries than females, and prolonged operative time was a risk factor. Caution should be exercised when performing extensive surgeries on male patients. Understanding the sex differences in medical treatments may lead to improved outcomes. Future studies should involve a larger sample size and consider using a large dataset from the whole of Japan.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Female gender is an independent predictor of operative mortality after coronary artery bypass graft surgery: contemporary analysis of 31 Midwestern hospitals Circulation Blankstein R Ward RP Arnsdorf M Jones B Lou YB Pine M 07112200510.1161/CIRCULATIONAHA.104.52513916159840 · doi ↗ · pubmed ↗
- 2Female sex as an independent predictor of morbidity and survival after isolated coronary artery bypass grafting Ann Thorac Surg Ahmed WA Tully PJ Knight JL Baker RA 59679220112160182810.1016/j.athoracsur.2011.02.033 · doi ↗ · pubmed ↗
- 3Sex differences in procedure selection and outcomes of patients undergoing mitral valve surgery Heart Surg Forum Vassileva CM Stelle LM Markwell S Boley T Hazelrigg S 08214201110.1532/HSF 98.2011103021997648 · doi ↗ · pubmed ↗
- 4Gender differences in mortality after mitral valve operation: evidence for higher mortality in perimenopausal women Ann Thorac Surg Song HK Grab JD O'Brien SM Welke KF Edwards F Ungerleider RM 204020448520081849881610.1016/j.athoracsur.2008.02.082 · doi ↗ · pubmed ↗
- 5Gender-related differences in patients with acute aortic dissection type AJ Thorac Cardiovasc Surg Rylski B Georgieva N Beyersdorf F 52853516220213192670910.1016/j.jtcvs.2019.11.039 · doi ↗ · pubmed ↗
- 6Gender differences in patients undergoing surgery for acute type A aortic dissection J Thorac Cardiovasc Surg Fukui T Tabata M Morita S Takanashi S 58158715020152619065510.1016/j.jtcvs.2015.06.031 · doi ↗ · pubmed ↗
- 7Sex-specific risk factors for early mortality and survival after surgery of acute aortic dissection type a: a retrospective observational study J Cardiothorac Surg Friedrich C Salem MA Puehler T Hoffmann G Lutter G Cremer J Haneya A 1451520203255270610.1186/s 13019-020-01189-w PMC 7301454 · doi ↗ · pubmed ↗
- 8Effects of sex on early outcome following repair of acute type A aortic dissection: results from the Nordic Consortium for Acute Type A Aortic Dissection (NORCAAD)Aorta (Stamford) Chemtob RA Hjortdal V Ahlsson A 714720193133054610.1055/s-0039-1687900 PMC 6645907 · doi ↗ · pubmed ↗