Predictive Nomogram and Propensity Score Matching in Neuroendocrine Carcinoma of the Tubular Gastrointestinal Tract: A US Population-Based Clinical Outcome Study
Abdul Qahar Khan Yasinzai, Marjan Khan, Abdullah Chandasir, Diego Olavarria-Bernal, Amir Humza Sohail, Agha Wali, Bisma Tareen, Tena Nguyen, Ashley D. Fox, Aman Goyal, Israr Khan, Abdul Waheed, Asif Iqbal, Nabin Raj Karki, Kanak Das, Asad Ullah

TL;DR
This study analyzes clinical outcomes for neuroendocrine carcinomas in the gastrointestinal tract using US population data to identify factors affecting survival.
Contribution
The study introduces a predictive nomogram and uses propensity score matching to evaluate clinical outcomes in a rare cancer type.
Findings
Women had a better 5-year survival rate compared to men.
Surgery was associated with the highest 5-year survival rate.
Age over 65 and distant metastasis were linked to worse survival outcomes.
Abstract
Neuroendocrine carcinomas (NECs) of the tubular gastrointestinal tract are rare and associated with worse clinical outcomes. Data from 10,387 patients were collected from the SEER database with a median age of 63 years. The most common primary tumor site was the small intestine. women had a superior 5-year survival rate. Age > 65 years, descending colon and anorectal sites were associated with worse prognosis. Surgical intervention and tumors located in the small intestine and appendix showed a better prognosis. Background: Neuroendocrine carcinomas (NECs) of the tubular gastrointestinal tract (GI-NECs) are rare and associated with worse clinical outcomes. This population-based study aims to highlight key demographics, clinicopathological factors, and survival outcomes in the US population. Methods: Data from 10,387 patients with GI-NECs were extracted from the Surveillance,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
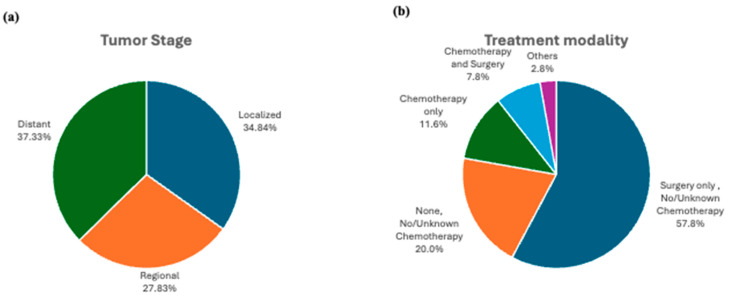 Figure 1
Figure 1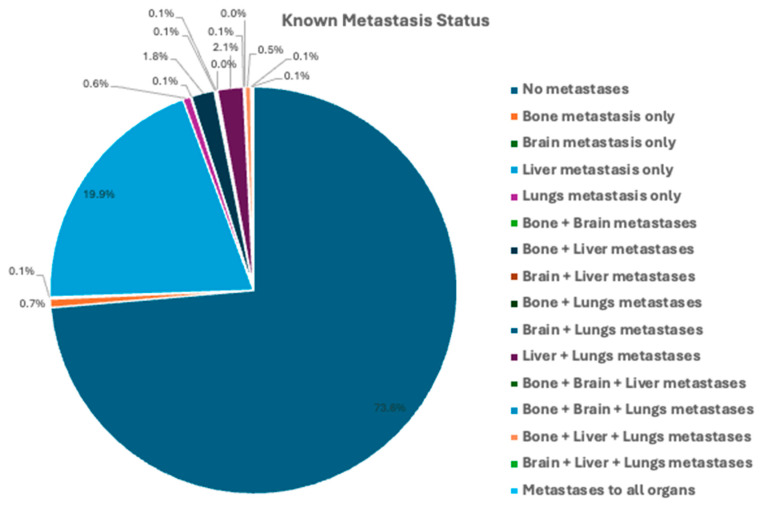 Figure 2
Figure 2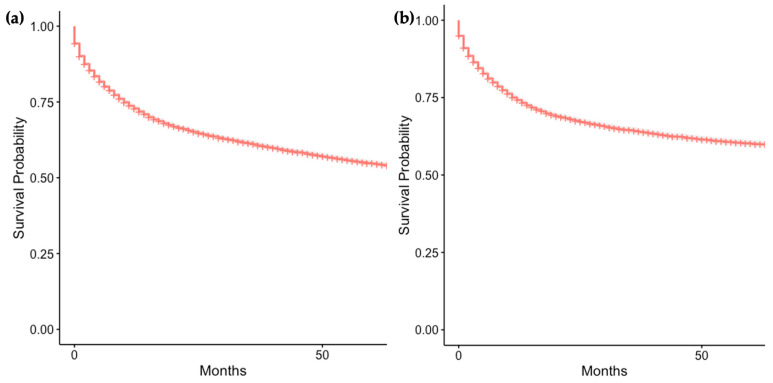 Figure 3
Figure 3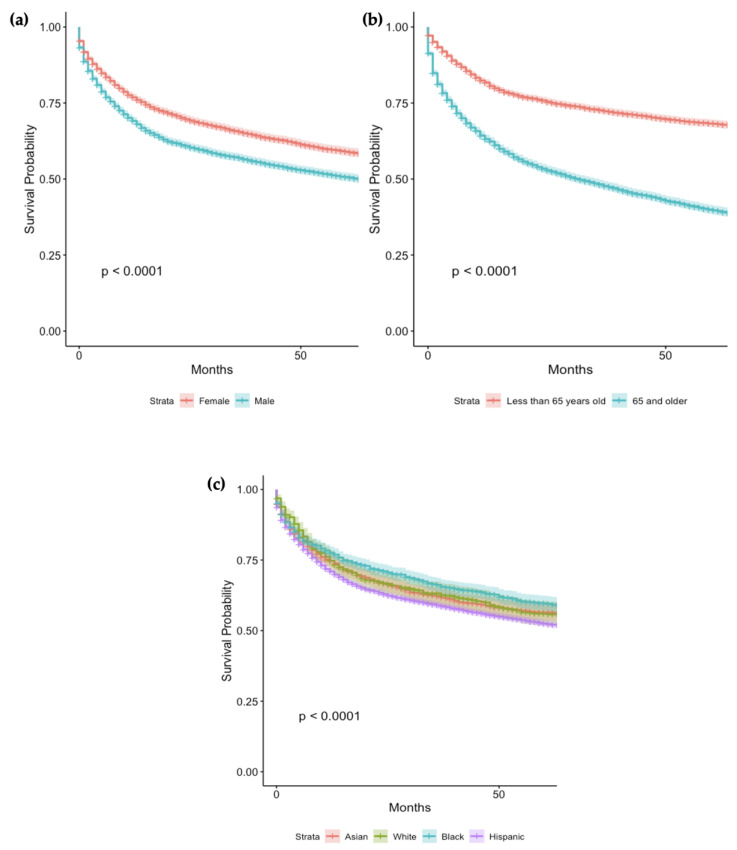 Figure 4
Figure 4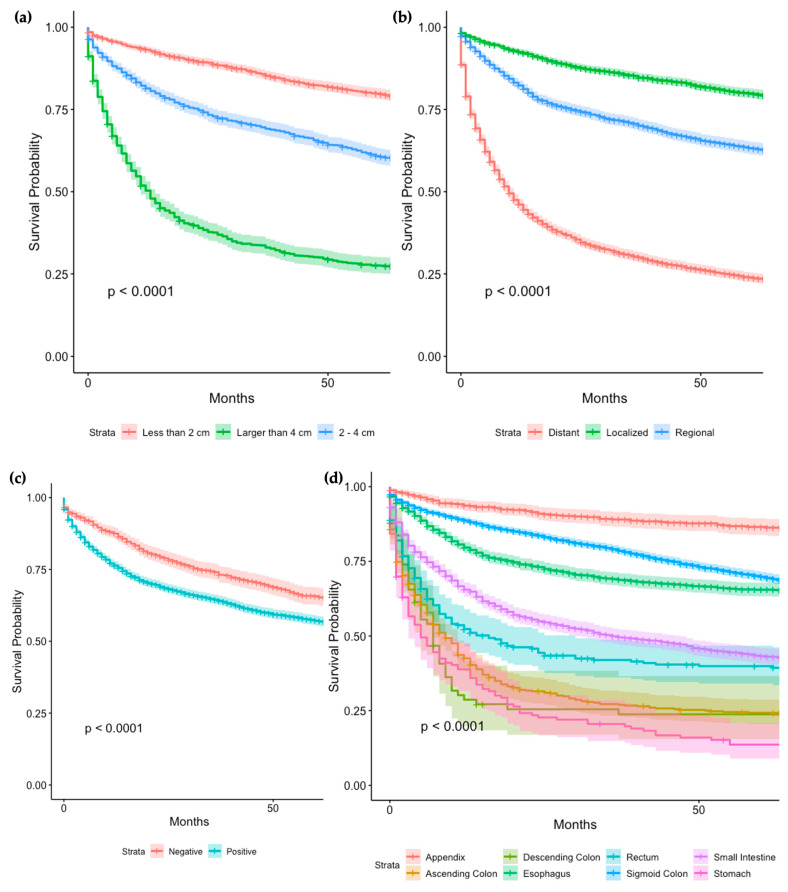 Figure 5
Figure 5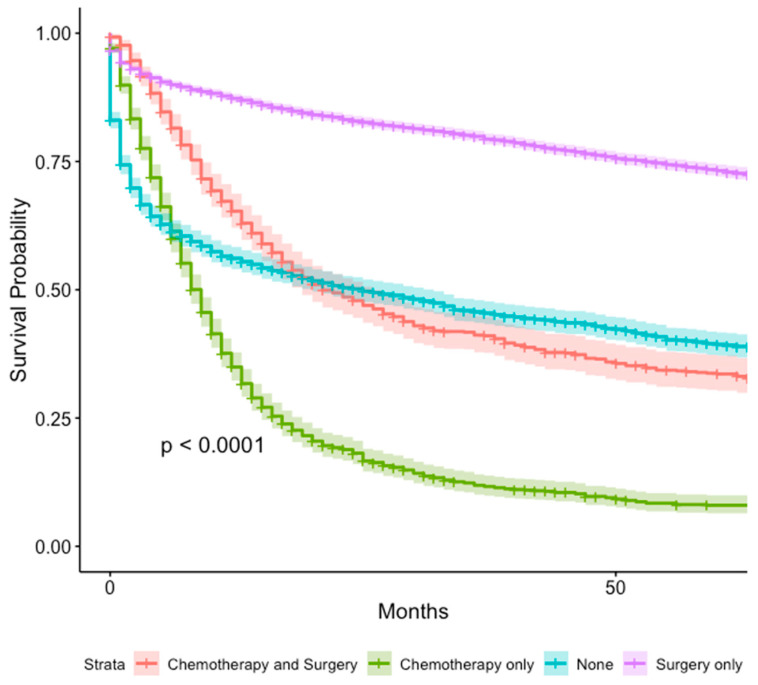 Figure 6
Figure 6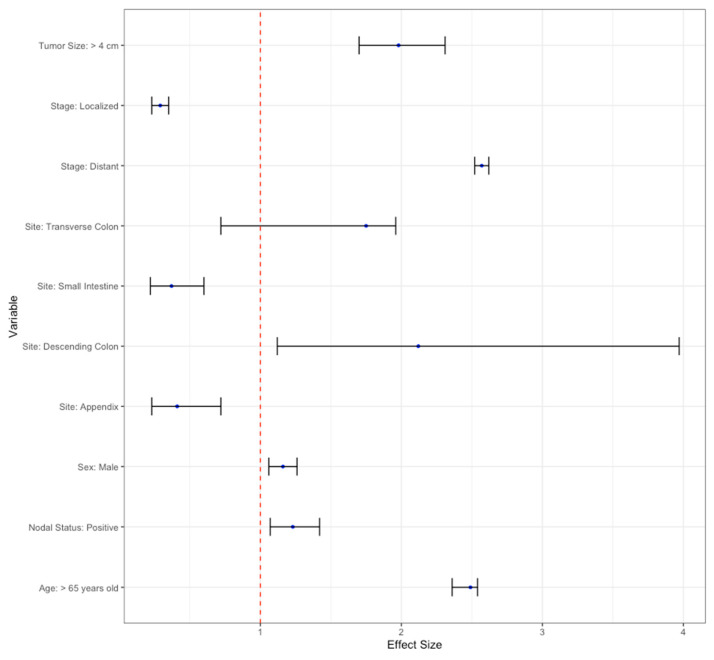 Figure 7
Figure 7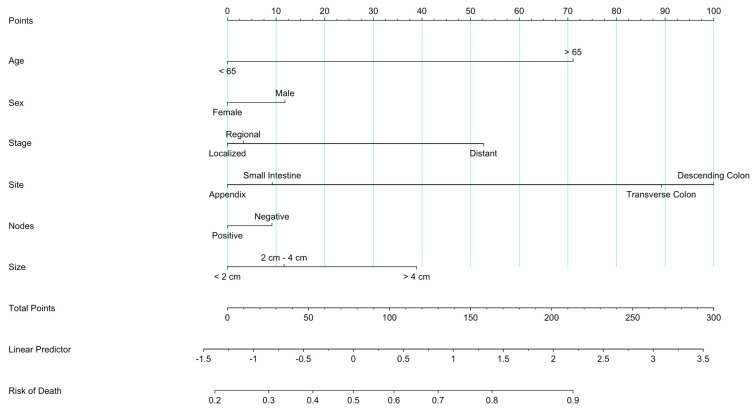 Figure 8
Figure 8Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroendocrine Tumor Research Advances · Lung Cancer Research Studies · Pancreatic and Hepatic Oncology Research
1. Introduction
Gastrointestinal neuroendocrine tumors (GI-NETs) are rare malignancies originating from multipotent stem cells located in the glands of the GI tract, with the capability to secrete biogenic amines and peptide hormones [1,2,3]. The reported incidence of GI-NETs in the United States is approximately 3.56 per 100,000 persons annually, with NECs composing approximately only 10–20% of all these tumors [4]. GI-NETs and NECs are characterized by the expression of neuroendocrine markers such as synaptophysin, chromogranin A, and somatostatin receptors [3,5]. However, GI-NETs can be differentiated based on their histological grade, differentiation, and location [1,2]. In 2019, the World Health Organization established classification guidelines for the malignant tumors of the digestive system, specifically noting the distinction between neuroendocrine tumors (NETs) as well-differentiated neoplasms and neuroendocrine carcinomas (NECs) as poorly differentiated neoplasms [2,6]. G3 staged NETs are considered well-differentiated yet high-grade tumors that are different/non-related to NECs [6]. However, the highly proliferative nature of G3 NETs has led to an increasing need for specific biomarkers to discern between G3 NETs and NECs [7,8].
GI-NECs can clinically present with nonspecific symptoms such as upper abdominal pain/discomfort or bleeding, whereas functional tumors may progress to present with secretory diarrhea, flushing, or multiple peptic ulcers [9]. Diagnostic imaging for NECs includes CTs or MRIs; however, advancements in endoscopic techniques have resulted in increased detection and diagnosis of GI-NECs [2,10]. The rarity of NECs has left much to be developed regarding the treatment and management of GI-NECs [11]. Currently, NECs are treated with multimodality therapy with small-cell lung cancer treatment protocols. With current NEC treatment regimens, prognosis is poor with survival ranging from 5 months in metastatic NECs to 38 months in the localized form of the disease [12]. In this study, we used the Surveillance, Epidemiology, and End Result (SEER) database to analyze demographic, treatment, and clinical outcomes, to further elucidate future therapeutic developments for GI-NECs. This study aims to provide a comprehensive understanding of GI-NECs, describe clinical patterns, assess the impact of current practices, and generate prognosis tools.
2. Materials and Methods
The data were extracted from the SEER database between the years 2000 and 2020 using SEER Stat software (Version 8.4.2). Inclusion criteria included histologically confirmed gastrointestinal neuroendocrine tumor/neoplasm, international classification of diseases version 3 (ICD-O-3) (https://seer.cancer.gov/seerstat/releasenotes.html, accessed 15 November 2023). Patients without histological confirmation and tumors classified as in situ were excluded. Extracted variables included age, gender, race, tumor stage, tumor grade, tumor histology, tumor size, lymph node status, type of treatment received, and survival. Statistical analysis was performed using R version 4.2.3 data-analysis software. Endpoints examined included overall survival, mortality, and 1- and 5-year cancer-specific survival. Univariate analysis was conducted to identify significant factors for multivariate analysis. The Cox regression method was used to calculate hazard ratios and to identify independent factors on survival outcomes. Unidentified or missing data were removed from multivariate analysis to ensure validity and remove biases in the case of non-random missing data. The data was analyzed using multivariate Cox regression with statistical significance defined as p < 0.05. A prognostic nomogram was also constructed to be used to predict future patient mortality and survival rate. This was done through the “rms” package in R. After pertinent prognostic variables were identified, the resultant mathematical models were then used to construct a nomogram. All variables that were found to have significance on the survival of patients through Cox Regression were added to the prognostic nomogram. The nomogram was then built using a Cox proportional hazards method. By giving each variable, a numerical score determined by how much of an impact it has on the overall forecast, the nomogram provides a visual representation of the predictive model. Following the addition of these scores, a total point value is produced that is correlated with the expected likelihood or risk of the specified outcome, such as the course of the disease or survival. The correctness and generalizability of the nomogram were confirmed through the use of internal and external validation approaches. Internal validation entailed evaluating the nomogram’s performance within the original dataset using resampling techniques like bootstrapping or cross-validation.
3. Results
Data from 10,387 patients with GI-NECs of the tubular GI tract met the inclusion criteria.
3.1. Demographic Characteristics
The distribution by gender in patients with GI NEC was relatively similar with a slight overall male predominance (51.5%). The median age of the patients was 63 years old, with ages ranging from 6 years old to older than 90 years of age. The highest number of patients were between 60 and 69 years of age (25.7%). White patients accounted for a majority (65.8%) of cases, with Black patients having the second most cases (14.4%). The data show an almost equal racial/ethnic distribution through the US population (https://www.census.gov/quickfacts/fact/table/US/PST045223, accessed on 14 April 2024). The breakdown of the median annual household income was close to even, with a slight majority (51.8%) of patients earning below $70,000 per year. A majority of our patients were from metropolitan areas (87.0%) (Table 1) (Supplemental Figure S1).
3.2. Tumor Characteristics and Treatment Modalities:
Most patients were younger than 65 years old, with a slight predominance in men (51.5%). The most common site for the NECs was the small intestine (33.6%), followed by the rectum (18.1%) and the stomach (15.4%). The largest proportion of patients had tumors smaller than 2 cm (44.5%). The most common tumor stage was distant (37.3%) followed by localized (34.8%) (Figure 1a).
The most common metastasis was to the liver (19.9%). The majority of patients (73.6%) with known metastasis information had no metastases. Lymph node status was known in 4391 (42.3%) of patients. In patients with known lymph node status, 3338 (76.0%) of patients had positive regional lymph nodes (Figure 2).
The most common treatment modality for patients with GI-NEC was surgery only (57.8%), followed by chemotherapy only (11.6%). A significant minority of patients did not receive any treatment (20.0%). A total of 210 patients with GI-NEC (2.0%) received multimodal therapy, or a treatment regimen consisting of chemotherapy, radiation therapy, and surgery (Figure 1b).
3.3. Overall and Cause-Specific Survival of Patients with GI-NEC
The 1-year and 5-year overall survival of the patient group was 72.9% (95% CI 72.0–73.7%) and 54.7% (95% CI 53.7–55.7%), respectively (Figure 3a). SEER calls disease-specific survival “cause-specific survival” in their database. The 1-year and 5-year cause-specific survival of the study group was 74.2% (95% CI 73.3–75.2%) and 60.0% (95% CI 59.0–61.1%) (Figure 3b) (Supplemental Figure S1).
3.4. Survival Analysis of Demographic Factors
3.4.1. Outcomes by Age
The 1-year and 5-year survival of patients below the age of 65 years was 81.7% (95% CI (80.7–82.8%) and 68.2% (95% CI 66.9–69.5%), respectively. The 1-year and 5-year survival of patients 65 years of age and older was 62.4% (95% CI 61.0–63.8%) and 38.9% (95% CI 37.4–40.4%), respectively (Figure 1a) (Supplemental Table S4). Univariate analysis determined older age to be associated with an increased mortality (H.R = 2.62, 95% CI 2.47–2.77%, p < 0.001) (Figure 4b).
3.4.2. Outcomes by Sex
The 1-year and 5-year survival of female patients was 76.9% (95% CI 75.7–78.1%) and 59.0% (95% CI 57.6–60.5%), respectively (Supplemental Table S2). The 1-year and 5-year survival of male patients was 69.1% (95% CI 67.9–70.4%) and 50.7% (95% CI 49.3–52.1%), respectively (Figure 1b). Univariate analysis found males to have a higher mortality rate (H.R = 1.28, 95% CI 1.21–1.35%, p < 0.001) (Figure 4a).
3.4.3. Outcomes by Race
The 1-year and 5-year survival for white patients was 70.9% (95% CI 69.8–72.0%) and 52.6% (95% CI 51.3–53.8%), respectively. The 1-year and 5-year survival for black patients was 77.6% (95% CI 75.5–79.8%) and 59.7% (95% CI 57.1–62.4%), respectively. The 1-year and 5-year survival for Hispanic patients was 74.7% (95% CI 72.3–77.2%) and 56.5% (95% CI 52.6–59.5%). The 1-year and 5-year survival for Asian patients was 74.8% (95% CI 71.3–78.4%) and 56.0% (95% CI 51.9–60.4%) (Supplemental Table S3) (Figure 4c). Univariate analysis found white patients to have a lower survival rate (H.R = 1.17, 95% CI 1.07–1.28%, p < 0.001) (Figure 4c).
3.5. Survival Analysis of Tumor Characteristics and Treatment ModalitiesTumor Characteristics
Tumor Characteristics
The survival rates for GI-NEC vary across different gastrointestinal sites. Notably, GI-NEC of the appendix demonstrated the best survival rates with 1-year and 5-year survivals of 93.7% (95% CI 91.8–95.5%) and 86.5% (95% CI 83.8–89.4%), respectively (Supplemental Table S7). Univariate analysis revealed significantly worse prognoses for GI-NEC of the ascending colon (H.R = 3.56, 95% CI 3.17–4.00%, p < 0.001), descending colon (H.R = 4.16, 95% CI 3.20–5.42%, p < 0.001), esophagus (H.R = 5.98, 95% CI 5.24–6.81%, p < 0.001), sigmoid colon (H.R = 2.44, 95% CI 2.07–2.86%, p < 0.001), stomach (H.R = 2.02, 95% CI 1.86–2.20%, p < 0.001), and transverse colon (H.R = 4.99, 95% CI 4.17–5.97%, p < 0.001) compared to GI-NEC of the small intestine, while GI-NEC of the appendix exhibited a better survival rate (H.R = 0.34, 95% CI 0.28–0.42%, p < 0.001) (Figure 5d).
The 5-year survival rates for patients with localized, regional, and distant tumors were 79.9% (95% CI 78.4–81.4%), 63.2% (95% CI 61.3–65.2%) and 24.0% (95% CI 22.5–25.5%), respectively (Supplemental Table S5). Localized tumors were associated with a better prognosis (HR = 0.51, p < 0.001), while distant tumors had a worse prognosis (HR = 3.05, p < 0.001) compared to regional tumors (Figure 5b).
For tumors smaller than 2 cm, the survival rate at 5 years was 79.8% (95% CI 78.2–81.5%). Tumors measuring 2 cm to 4 cm had survival rates of 60.8% (95% CI 58.5–63.3%), while those greater than 4 cm had rates of 27.6% (95% CI 25.2–30.2%) (Supplemental Table S6). Larger tumors were linked to higher mortality, with tumors > 4 cm showing the poorest outcomes (HR = 5.20, p < 0.001) (Figure 5a).
The 5-year survival rates of patients with negative and positive regional lymph node statuses were 65.7% (95% CI 62.7–68.8%) and 57.2% (95% CI 55.4–58.9%), respectively (Supplemental Table S8). Positive lymph node status was associated with increased mortality (HR = 1.33, p < 0.001) (Figure 5c).
3.6. Treatment Modalities
The 1-year and 5-year survival for patients that received chemotherapy only was 34.9% (95% CI 32.3–37.8%) and 8.0% (95% CI 6.4–10.0%). The 1-year and 5-year survival for patients that received surgery only was 87.3% (95% CI 86.5–88.2%) and 73.2% (95% CI 72.0–74.4%). The 1-year and 5-year survival for patients who received chemotherapy and surgery was 65.3% (95% CI 62.1–68.7%) and 33.6% (95% CI 30.3–37.2%). The 1-year and 5-year survival for patients without treatment was 56.1% (95% CI 54.0–58.3%) and 33.6% (95% CI 30.3–37.2%) (Supplemental Table S9). Univariate analysis found patients who received chemotherapy only had the worst outcomes (H.R = 6.02, 95% CI 5.57–6.51%, p < 0.001) (Figure 6). Other treatment modalities were not analyzed due to low power.
3.7. Multivariate Analysis
Multivariable analysis was performed using Cox Survival Regression analysis. Independent factors associated with increased mortality were identified as age greater than 65 years, male gender, a GI-NEC tumor site of the transverse colon or descending colon, tumor stage of distant, positive nodal status, or a tumor size of >4 cm. Factors associated with decreased mortality were a tumor site of an appendix or small intestine, or a localized tumor (Table 2). A hazard ratio above 1 indicates a higher incidence of mortality in the pertaining group, whereas a hazard ratio below 1 indicates a decreased incidence of mortality. All significant statistical factors and their hazard ratios are displayed in the Forest plot. The hazard ratios are displayed along with confidence intervals (Figure 7).
3.8. Prognostic Nomogram
To create a predictive measure that could extrapolate the survival of patients with GI-NEC, a prognostic nomogram was created to measure patient survivability using the factors of age, treatment, and systemic treatment. The nomogram visually represents the predictive model by assigning a numerical score to each variable based on its relative contribution to the overall prognosis. These scores are then summed to generate a total point value, which correlates with the predicted probability or risk of the defined outcome, which was overall survival (OS). The prognostic nomogram showed increased mortality for patients with a higher age. In addition to that, the prognostic nomogram also predicted increased mortality for patients who had tumors greater than 4 cm in size. Distantly metastasized tumors were associated with a significantly increased probability of death, whereas regional metastases were associated with a moderate increase in mortality. The nomogram also showed a slight increase in mortality for patients that were males. Tumors of the descending or transverse colon were associated with higher mortality, whereas tumors of the small intestine and appendix were associated with decreased mortality (Figure 8).
3.9. Propensity Score Matching
To further investigate the effect of gender on mortality, propensity score matching was performed. Male and Female patients were matched based on the demographic, tumor, and treatment factors that were found to have significant effect on survival based on the multivariate analysis—age, tumor stage, tumor size, tumor site, and regional lymph node status. Propensity score matching showed that when matched to females of similar age, tumor stage, size, site and regional lymph node status, males had a higher mortality rate (p = 0.049).
4. Discussion
Our study analyzed data from 10,387 patients, most of whom were white, finding a slight predominance of GI NEC in the male population. The small intestine was the most common site, and the most common stage was distant (37.3%). The liver is the most frequent site of metastasis. Surgery was the most common treatment modality.
The univariate analysis showed that older age is associated with increased mortality. Factors associated with worse prognosis: tumors of the esophagus, stomach, and at any part of the colon. Tumor size > 4 cm. On the other hand, tumor of the appendix and patient who underwent only surgery showed the best survival rate.
The multivariable analysis identified factors associated with increased mortality: age greater than 65 years, male gender, a GI-NEC tumor site of the transverse colon or descending colon, tumor stage of distant, positive nodal status, or a tumor size of >4 cm. Factors associated with decreased mortality were a tumor site of the appendix or small intestine or a localized tumor.
With all this information, we created a prognostic nomogram, which showed increased mortality for older age, patients with tumors greater than 4 cm in size, distant metastasis, and tumors of the descending or transverse colon. On the other hand, tumors of the small intestine and appendix were associated with decreased mortality. Men present a slight increase in mortality, which was confirmed by the propensity score analysis.
Of all GI neuroendocrine malignancies, GI-NECs represent 10–20% of these cancers [13]. However, due to their aggressive nature, there are limited studies investigating the epidemiology of GI-NECs as most cases are commonly diagnosed in their advanced stages [13,14].
A previous SEER database study identified 5509 cases of GI-NECs between 2000 and 2012, with most NECs occurring in the colon (26%), pancreas (20%), and rectum (12%) [15]. In our study, the most common site was the small intestine. This difference may be attributed to the inclusion of pancreatic NEC in the previous study, while our excluded and included SEER data through the year 2018. Moreover, GI-NEC site variations may depend on geography; in Taiwan and Japan, the rectum is the most common primary site, while in Australia and Canada, the small intestine is the most common site, similar to our study [16,17,18,19,20]. The common site of metastasis is strongly predicted by the primary site of tumor [21]. Because we cannot discern if these differences can be attributed to genetic or environmental factors, further studies are needed to substantiate the existence of possible modifiable GI-NEC risk factors.
Furthermore, in our study, older age (>65 years) at diagnosis, size >4 cm, and distant metastasis were independent negative risk factors affecting overall survival. Tumors of the esophagus, anus, cecum, and colon were also risk factors associated with increased mortality. NEC of the colon has been found to have worse survival compared to other sites of the GI tract [22]. Colon NEC have a higher tendency to metastasize than their peers contributing to its worse survival [23].
Age as an independent risk factor was also found in a previous study where the authors analyzed data of 1861 patients, between 2004 and 2013. They found that younger age (<65 years) correlates with improved survival (p < 0.001) [24].
Sorbye et al. demonstrated that patients with primary colon tumors had significantly shorter median survival compared with other primary tumors [25]. Regarding independent factors associate with decreased mortality, a previous study also reported GI NEC from the small intestine as presenting better 5-year OS (68.2%) compared NECs of the rectum or colon (p < 0.001) [26].
Regarding treatment outcomes, our study found no added survival benefit with the addition of chemotherapy and radiation compared to surgical resection alone, but information about adjuvant therapy was limited.
In this regard, the Expert Consensus Practice Recommendations of the North American Neuroendocrine Tumor Society for the management of high-grade gastroenteropancreatic and gynecologic neuroendocrine published in 2023 states that the role of surgery, even with locoregional disease, is questionable due to poor prognosis, and suggest systemic therapy with chemoradiation especially in cases where surgery represents higher morbidity. The stronger indication of surgery is for localized NEC, but even here, there is an indication for chemotherapy and possibly radiation (esophageal, anal some rectal tumors). The same publication states chemoradiation strategies may provide durable local control for primary and metastatic disease [27]. There is still room for discoveries and approaches regarding the best treatment. Currently, there is an open trial to evaluate the efficacy of neoadjuvant chemotherapy in terms of DFS in patients with localized tumors [28].
The molecular landscape in NENs varies according to the type and location of the tumor [29]. Previous studies have highlighted the molecular complexities between well-differentiated G3 GI-NETs and poorly differentiated GI-NECs, paving the way for new treatment and management avenues [30]. Well-differentiated GI-NETs have a low rate of genomic alterations with a tumor mutational burden average of 1.09 mutations per megabase [31]. Frequent alterations are ARID1A, ATM, CDKN2A, KDM5A, ESR1, MYC, RB1, MEN1, and ATRX [32,33]. In contrast, NECs have intermediate tumor mutational burden with an average of 5.45/Mb and frequent alterations in TP53, KRAS, RB1, CSMD3, APC, CSMD1, LRATD2, TRRAP, and MYC [32,34].
APC, TP53, KRAS, or BRAF mutations occurred in 83% of large cell (LC) NECs and only 21% of G3-NECs, with a positive predictive value of about 83%. The study also revealed differences in microsatellite instability (MSI) between GI-NEC (5.3%) and G3 GI-NETs (3.4%) [32].
Based on Platinium-etoposide (PE) regimens outlined for SCLC, GI-NECs have a worse prognosis than their G3 GI-NET counterparts, with a median overall survival of <1 year with treatment and an overall response rate (ORR) of 30–56% [12,30,35]. On the other hand, G3 GI-NETs have a better overall prognosis but an inferior response to combination (ORR from 0% to 17%) [35].
The drastic differences in prognosis and treatment responses between G3 GI-NETs and GI-NECs solidify the need to elucidate the genomic differences between the two cancers.
Limitations
A major limitation of our study is the changing classification of NECs over time; the current WHO classification cannot be directly extrapolated to the categories available from the SEER database. Regarding therapy, the timing of the chemotherapy (adjuvant vs. neoadjuvant), the regimens and the duration of therapy are not available from the SEER database. Clinical factors like socioeconomic status, comorbidities, and side effects from therapies that might affect the outcomes are not always accurately coded or cannot be obtained from the SEER database. In addition, the prognostic nomogram was not tested prospectively. Despite these limitations, our study attempts to further characterize clinical and demographical aspects of the rare neuroendocrine carcinomas of the tubular GI tract.
5. Conclusions
To our knowledge, this is the largest population database study to date on GI-NECs of the tubular GI tract. The most common sites of NECs were the small intestine. Affected adults were generally older than 40 years old with the highest peak between 60 and 69 years old, with a small male predominance. In addition, compared to men, women had a better overall 5-year survival rate. Multivariate analysis shows older age (>60 years old), tumor size > 4 cm, and distant metastasis as independent risk factors associated with mortality. Esophageal, colonic, and anorectal locations of GI-NECs are also indicative of increased mortality, along with the presence of liver or lung metastases. Surgical resection provided the best outcome with no clear benefit observed for radiation and chemotherapy. However, our analysis also indicated better prognosis-associated tumor sites in the small intestine and appendix. This study provides better clinical and demographic insight into future clinical trials to include patients from all ethnicities and races for future personalized therapeutic approaches.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bonds M. Rocha F.G. Neuroendocrine Tumors of the Pancreatobiliary and Gastrointestinal Tracts Surg. Clin. N. Am.202010063564810.1016/j.suc.2020.02.01032402306 · doi ↗ · pubmed ↗
- 2Klöppel G. Neuroendocrine Neoplasms: Dichotomy, Origin and Classifications Visc. Med.20173332433010.1159/00048139029177160 PMC 5697503 · doi ↗ · pubmed ↗
- 3Rindi G. Mete O. Uccella S. Basturk O. La Rosa S. Brosens L.A.A. Ezzat S. de Herder W.W. Klimstra D.S. Papotti M. Overview of the 2022 WHO Classification of Neuroendocrine Neoplasms Endocr. Pathol.20223311515410.1007/s 12022-022-09708-235294740 · doi ↗ · pubmed ↗
- 4Pavel M. Öberg K. Falconi M. Krenning E.P. Sundin A. Perren A. Berruti A. Gastroenteropancreatic neuroendocrine neoplasms: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up Ann. Oncol.20203184486010.1016/j.annonc.2020.03.30432272208 · doi ↗ · pubmed ↗
- 5World Health Organization WHO Classification of Tumours. Digestive System Tumours: WHO Classification of Tumours, Volume 1World Health Organization Geneva, Switzerland 2019
- 6Raphael M.J. Chan D.L. Law C. Singh S. Principles of diagnosis and management of neuroendocrine tumours Can. Med. Assoc. J.2017189 E 398E 40410.1503/cmaj.16077128385820 PMC 5359105 · doi ↗ · pubmed ↗
- 7Tang L.H. Basturk O. Sue J.J. Klimstra D.S. A Practical Approach to the Classification of WHO Grade 3 (G 3) Well-differentiated Neuroendocrine Tumor (WD-NET) and Poorly Differentiated Neuroendocrine Carcinoma (PD-NEC) of the Pancreas Am. J. Surg. Pathol.2016401192120210.1097/PAS.000000000000066227259015 PMC 4988129 · doi ↗ · pubmed ↗
- 8Stawarski A. Maleika P. Neuroendocrine tumors of the gastrointestinal tract and pancreas: Is it also a challenge for pediatricians?Adv. Clin. Exp. Med.20202926527010.17219/acem/11180632091671 · doi ↗ · pubmed ↗