Blood Fluke Infection (Spirorchidiasis) and Systemic Granulomatous Inflammation: A Case Study of Green Sea Turtles (Chelonia mydas) on Jeju Island, South Korea
Da Sol Park, Won Hee Hong, Jae Hoon Kim, Adams Hei Long Yuen, Sib Sankar Giri, Sung Bin Lee, Won Joon Jung, Young Min Lee, Su Jin Jo, Mae Hyun Hwang, Jae Hong Park, Eun Jae Park, Se Chang Park

TL;DR
This case study examines spirorchiidiasis in green sea turtles from South Korea, highlighting severe systemic inflammation and the need for conservation efforts.
Contribution
The study provides a detailed pathological analysis of spirorchiidiasis in green sea turtles from Northeast Asia.
Findings
Spirorchiidiasis caused severe lung lesions and systemic granulomatous inflammation in green sea turtles.
Computed tomography revealed pulmonary and extrapulmonary manifestations, including joint masses.
Histopathology confirmed the presence of spirorchiid ova in multiple organs of infected turtles.
Abstract
This case report offers a comprehensive analysis of the clinical symptoms, radiological findings, and postmortem examinations of three green sea turtles (Chelonia mydas) investigated for spirorchiidiasis. These findings highlight the complexity and severity of the disease, emphasizing the presence of systemic, granulomatous inflammation, and its impact on the overall health of sea turtles. This study advocates for continuous research and conservation efforts to mitigate the impact of spirorchiidiasis on marine turtles. Despite the precarious state of marine turtles as a highly endangered species, our understanding of their diseases remains limited. This case report presents a detailed pathological investigation of spirorchiidiasis, a blood fluke infection that poses a substantial threat to marine turtles. This retrospective study examined three cases of spirorchiid-infected sea…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
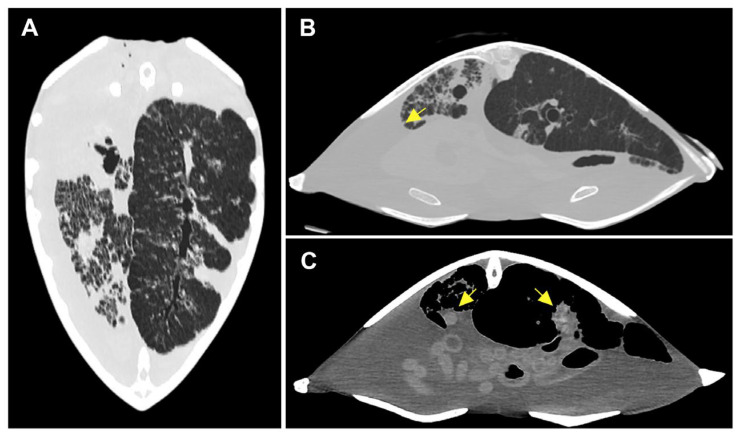 Figure 1
Figure 1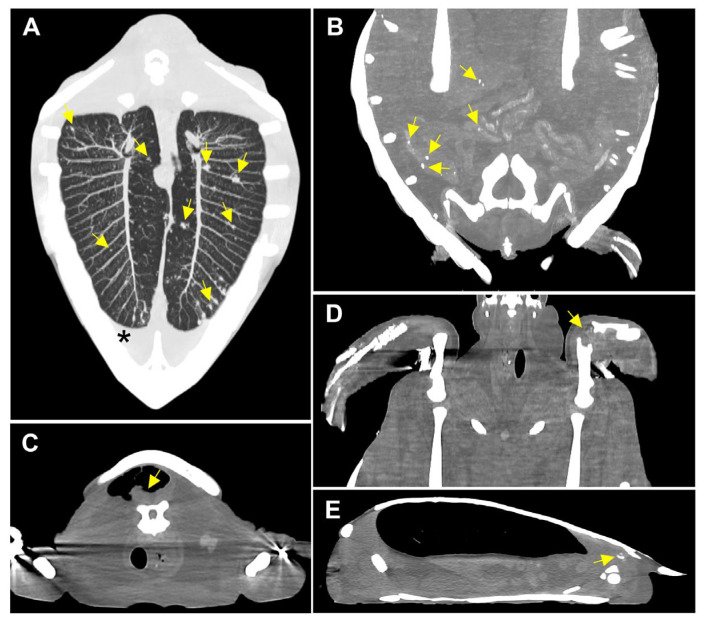 Figure 2
Figure 2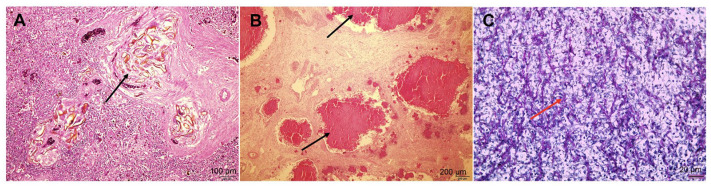 Figure 3
Figure 3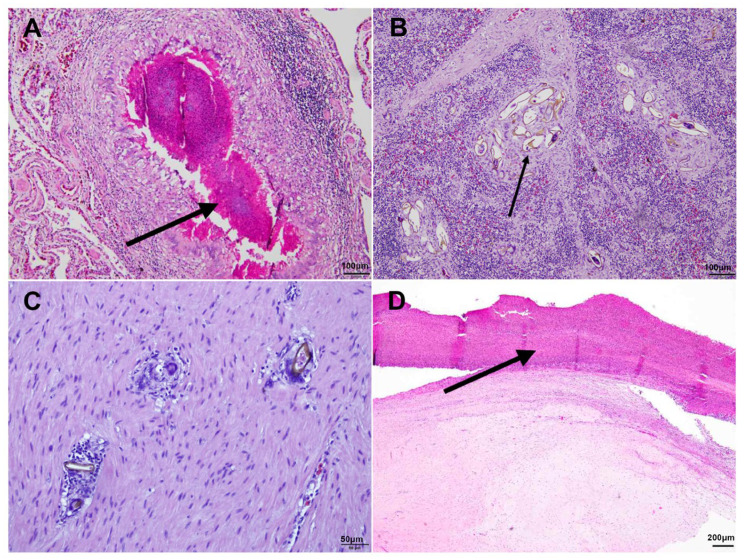 Figure 4
Figure 4- —National Research Foundation of Korea (NRF)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTurtle Biology and Conservation · Bird parasitology and diseases · Parasite Biology and Host Interactions
1. Introduction
Spirorchiid infections are highly prevalent in turtles worldwide, including in Australia, Hawaii, Florida, Egypt, Italy, Indonesia, India, Japan, and Taiwan [1]. However, manifestations of severe diseases appear to demonstrate spatial disparities [2]. The occurrence of chronic and fatal spirorchiid infections raises concerns about mortality, complicating diagnosis with nonspecific clinical signs such as anorexia, cachexia, sunken eyes, and plastron concavity [3]. The diverse pathological effects associated with spirorchiid fluke infection affect various organs and tissues, primarily the aortae and heart chambers where adult flukes are frequently found, eventually causing systemic granulomatous inflammation [1].
To the best of our knowledge, there are no reports on the pathological details of spirorchiidiasis in sea turtles in Northeast Asia. This retrospective case report was conducted to provide insights into the pre- and postmortem examination of spirorchiid infections in South Korea, particularly in the waters surrounding Jeju Island. We aimed to present the clinical symptoms, computed tomography (CT) results, postmortem gross findings, and histopathology of spirorchiid infections.
2. Materials and Methods
2.1. Specimen Information
This retrospective case study was conducted to investigate the clinical history and postmortem findings of three stranded juvenile green sea turtles (Chelonia mydas) with spirorchiid-infection that were admitted to Aqua Planet, Jeju Island, South Korea (Table 1). Lethargy and respiratory distress were noted in all three turtles upon physical examination. During the treatment period, the turtles received a comprehensive therapeutic regimen involving antibiotics, fluid therapy, vitamin complex injections, anti-inflammatory agents, and forced tube feeding. All three turtles succumbed to their conditions and died during the rehabilitation period.
2.2. Premortem Examination
Blood samples were collected for use in hematology and biochemistry. Manual assessments were performed for white blood cells, red blood cell counting, and to determine packed cell volume. Hemoglobin level and blood chemical analyses were carried out using the FujiFilm Dri-chem 4000i (Fujifilm Techno Products Co., Ltd., Takematsu, Japan).
CT scanning was conducted in Case 2 and Case 3 using a 16-row, 32-slice helical CT system from Aquilion Lightning (Aquilion Lightning, Canon Medical Systems, Otawara, Japan). The scan was performed at 120 kV, 250 mA, and 2 mm slice thickness, while the scan field of view (sFOV) was set to 39 cm. CT images were then assessed using open-source Digital Imaging and Communications in Medicine (DICOM) viewing software, Horos version 3.3.6.
2.3. Postmortem Examination
Turtles were necropsied within a day of their deaths using standard methods for sea turtle postmortem examination [4]. Tissue samples were collected and fixed with 10% neutral-buffered formalin (OCI Company Ltd., Seoul, Republic of Korea) at a 10:1 fixative-to-tissue ratio before being processed in paraffin wax and sectioned. The tissue slides were then stained with hematoxylin and eosin (H&E), a Gram staining kit (modified Brown and Brenn method; Sigma-Aldrich, St. Louis, MO, USA), and a periodic acid Schiff (PAS) stain kit (Muto Pure Chemicals Co., Ltd., Tokyo, Japan).
3. Results
3.1. Premortem Examination
3.1.1. Clinical Symptoms and Blood Analysis
All three turtles exhibited uniform clinical symptoms, including algal coverage, buoyancy issues, lethargy, dehydration, and emaciation (Body condition score 2), all of which are indicative of nonspecific distress. Table 2 and Table 3 summarize the hematological and serum chemistry data for each turtle. The observed elevation in blood urea nitrogen aligns with clinically observed dehydration, while the parallel reduction in total protein and cholesterol matches the noted malnutrition. Given the context of dehydration, the manual packed cell volume (mPCV) levels in Cases 2 and 3, namely, 11.5% and 24% (normal range: 17–38%), are considered low and may indicate the presence of severe anemia. The concurrent elevation of aspartate aminotransferase and creatine kinase, observed in all three cases, can be associated with factors like muscle damage and infection causes.
3.1.2. Radiological Findings
Using pulmonary window settings, the CT images of Case 2 demonstrated a ground-glass opacification pattern in the left lung and widespread peribronchovascular consolidations in the right lung, indicating the presence of pulmonary infection (Figure 1A). Both Case 2 and 3 exhibited pleural effusion (Figure 1B and Figure 2A). Case 2 revealed two irregular consolidated masses extending from the pleura, with lengths up to 2.5 cm. These were observed in the lung field (Figure 1C). Case 3 displayed multiple pulmonary nodules (Figure 2A). In Case 3, multiple calcified nodules were observed in the intestinal mucosa and gallbladder (Figure 2B). A well-defined mass (0.7 cm [H] × 1.3 cm [W] × 1.1 cm [L]) enclosed by an intramuscular air pocket was observed beneath the nuchal of the carapace (Figure 2C). A mass (1 cm [H] × 3.2 cm [W] × 3.5 cm [L]) was observed in the left humeroulnar and humeroradial joints (Figure 2D). Using bone window settings, a calcified lesion (1.2 cm [H] × 1.5 cm [W] × 2 cm [L]) was observed beneath the right 5th carapace scutes and adjacent to the right ilium (Figure 2E).
3.2. Postmortem Examination
3.2.1. Gross Findings
The necropsy of Case 1 revealed a greenish intracoelomic exudate upon theincision of the coelomic cavity, with abdominal organs and omentum being uniformly covered in yellow nodules (<0.5 mm). The lungs and bronchi showed foam accumulation, and serosa from the lower duodenum to the rectum displayed vasodilation and redness. In Case 2, both lungs had abscesses and possible inflammatory nodules, with bronchial foam observed. The spleen exhibited petechial hemorrhages. Case 3’s necropsy showed multifocal granulomas in lung parenchyma and similar yellow nodules on abdominal organs and lung cross-sections. Inflammatory masses were noted in various joints, including the left elbow, carapace, right femoral, iliac, and sternal joints. No adult flukes were noted during the necropsies.
3.2.2. Histopathological Findings
In Case 1, multifocal granulomas were noted in the pleura, with PAS staining confirming the presence of fungal spores and hyphae in the lungs, alongside yellowish ova indicating spirorchiid infection in the lung parenchyma. The heart showed nonsuppurative endocarditis and vasculitis, while the liver and pancreas revealed granulomas with fungal hyphae and necrosis. Severe inflammation and spirorchiid ova were also present in the spleen and beneath the intestinal mucosa, with urate crystals being present in kidney ducts.
Case 2 revealed similar lung parenchyma granulomas (Figure 3B), with evidence of fungal (Figure 3C), bacterial, and spirorchiid developments. Further, there was spleen inflammation, characterized by the presence of spirorchiid ova around blood vessels (Figure 3A). Additionally, Case 2 showed numerous deposits of dark pigmentation in the liver.
Similarly, Case 3 showed the pathology of lungs with a fungal and bacterial presence, yellowish parasitic ova, and associated inflammatory responses. Notably, Case 3 exhibited severe multifocal granulomatous inflammation, with spirorchiid ova being present in most major organs, including the lungs (Figure 4A), spleen (Figure 4B), liver, heart (Figure 4C), kidneys, and digestive system. Severe multifocal granulomatous inflammation was evident in the carapace and bone tissues (Figure 4D).
The ova observed in our study displayed multiple morphological, similarities to those of the spirorchiid ova reported in earlier research [2]. These eggs, measuring up to 100 × 50 µm, are oval-shaped with a yellowish wall (Figure 3A and Figure 4B,C). The presence of blue, round aggregates, which are considered to be miracidia, along with the surrounding granulomatous lesions is consistent with observations in a previous study [2]. These morphological features confirm that the specimens in our study are spirorchiid ova, supporting our diagnostic conclusions.
4. Conclusions
The complex respiratory and multi-organ pathologies seen in fatal spirorchiidiasis cases from Korea highlight the importance of a systemic diagnostic approach for the diagnosis, progression, and prognosis of spirochidiasis. Currently, the diagnosis of spirorchiidiasis relies on accurate postmortem pathogen identification [1]. The alignment between CT findings and histopathology demonstrates the potential benefits of premortem imaging for accurate disease assessment. In addition, given that many fungi are ubiquitous organisms and part of the natural microbiota of the respiratory systems of sea turtles and other reptiles, their role in secondary infections is substantial [7]. The severe granulomatous inflammation observed (especially in the spleen of Case 2), along with spirorchiid infection, suggests that parasitic infection may predispose or exacerbate the growth of opportunistic fungal pathogens, thereby leading to secondary infections. This relationship between the presence of spirorchiid ova and secondary fungal infections underscores the need for a comprehensive understanding of host–pathogen interactions in sea turtles in order to better diagnose, manage, and prevent the progression of such complex infections.
In this study, no adult flukes were found, and DNA could not be obtained from the ova, making species-level identification impossible. Further research, including comprehensive necropsies with traditional parasitological examinations, is needed to accurately assess the infection status of this parasitic group in the domestic sea turtle population. Continuous efforts on an international scale are essential for developing comprehensive strategies for monitoring, managing, and conserving marine turtle populations facing the threat of spirorchiid infection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chapman P.A. Cribb T.H. Flint M. Traub R.J. Blair D. Kyaw-Tanner M. Mills P.C. Spirorchiidiasis in Marine Turtles: The Current State of Knowledge Dis. Aquat. Org.201913321724510.3354/dao 0334831187736 · doi ↗ · pubmed ↗
- 2Chapman P.A. Owen H. Flint M. Soares Magalhães R.J. Traub R.J. Cribb T.H. Kyaw-Tanner M.T. Mills P.C. Molecular Epidemiology and Pathology of Spirorchiid Infection in Green Sea Turtles (Chelonia mydas)Int. J. Parasitol. Parasites Wildl.20176394710.1016/j.ijppaw.2017.03.00128331802 PMC 5345959 · doi ↗ · pubmed ↗
- 3Glazebrook J.S. Campbell R.S.F. Blair D. Pathological changes associated with cardiovascular trematodes (Digenea: Spirorchidae) in a green sea turtle Chelonia mydas (L)Comp. Haematol. Int.19819136136810.1016/0021-9975(81)90006-27320241 · doi ↗ · pubmed ↗
- 4Manire C.A. Norton T.M. Stacy B.A. Sea Turtle Health & Rehabilitation J. Ross Publishing Fort Lauderdale, FL, USA 2017209239
- 5Samour J.H. Hewlett J.C. Silvanose C. Hasbun C.R. Al-Ghais S.M. Normal haematology of free-living green sea turtles (Chelonia mydas) from the United Arab Emirates Comp. Haematol. Int.1998810210710.1007/BF 02642499 · doi ↗
- 6Lewbart G.A. Hirschfeld M. Denkinger J. Vasco K. Guevara N. García J. Muñoz J. Lohmann K.J. Blood Gases, Biochemistry, and Hematology of Galapagos Green Turtles (Chelonia mydas)P Lo S ONE 20149 e 9648710.1371/journal.pone.009648724824065 PMC 4019482 · doi ↗ · pubmed ↗
- 7Domiciano I.G. da Silva Gagliotti G.F.P. Domit C. Lorenzetti E. Bracarense A.P.F.R.L. Bacterial and fungal pathogens in granulomatous lesions of Chelonia mydas in a significant foraging ground off southern Brazil Vet. Res. Commun.20224685987010.1007/s 11259-022-09911-w 35378659 · doi ↗ · pubmed ↗