INTERP: Interpreter requirements needed for tissue plasminogen activator evaluations and resulting performance: a retrospective review
Julia Ting Bu, Dawn M. Meyer, Benjamin Shifflett, Brett C. Meyer

TL;DR
This study examines how interpreter services affect the timing of administering rt-PA for stroke patients.
Contribution
It identifies that interpreter service needs do not delay rt-PA administration but increase exclusion due to time.
Findings
Patients needing interpreters had no significant delay in rt-PA administration.
Interpreter-requiring patients were more likely to be excluded from rt-PA due to being out of the time window.
Baseline characteristics were similar between interpreter and non-interpreter groups.
Abstract
To examine the influence of interpreter service needs (IS) on rt-PA administration time metrics. Retrospectively reviewed prospectively collected data from Comprehensive Stroke Center database (January 2011- April 1, 2021) and EMR. Inclusion: Subjects for whom a “stroke code” was activated. Excluded in-house strokes. Baseline characteristics, frequency of rt-PA, rt-PA exclusions and time metrics, NIHSS were compared between patients who did or did not require IS. Analyses utilized ANOVA, t-Test, Brown-Mood Median Test, or Pearson’s Chi-squared test as appropriate. Of 2,191 patients with stroke code activations, 81 had a documented need for IS. Rt-PA was administered in 9 IS and 358 non-IS patients. Median baseline NIHSS was higher in rt-PA group (9±8 vs 3±9, p<0.005). In IS patients, there were no differences in baseline characteristics between those who received rt-PA and those who…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
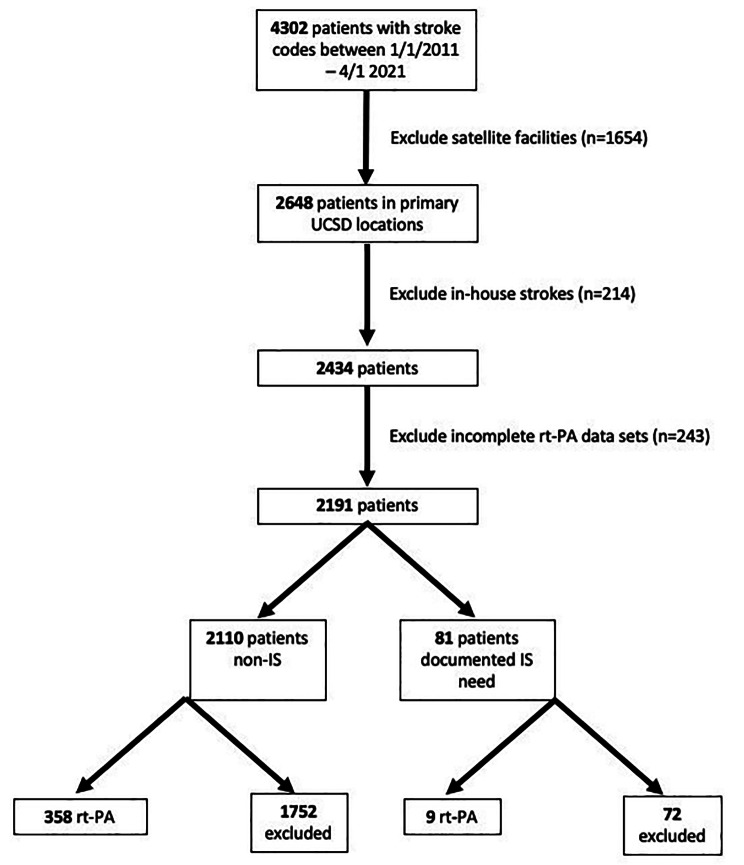 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInterpreting and Communication in Healthcare · Healthcare Systems and Practices · Acute Ischemic Stroke Management
Introduction
In an acute stroke, “Time is brain”. Language barriers can inhibit efficient emergency response. In our experience, acute ischemic stroke (AIS) patients requiring interpreter services during an acute stroke code can experience care delays in obtaining a qualified medical interpreter.
Current literature is nebulous regarding the effect of language interpretation service needs (IS) on acute stroke response and outcomes. Though rt-PA administration rate does not appear to be different [1] in patients requiring IS versus not, patients in the former group were more likely to be discharged to facilities [2] or discharged with more severe neurologic deficits [3] with worse quality of life indicators on follow up [4]. Another study found no significant difference in quality benchmarks and outcomes [5].
The purpose of this study was to examine the influence of requiring IS on time metrics of rt-PA administration among acute stroke patients found in one comprehensive stroke center database.
Methods
We retrospectively reviewed prospectively collected data from our Comprehensive Stroke Center database (1/2011-4/1/2021) and EMR. The status of requiring interpreter services was identified by patient or healthcare proxy. Subjects in one of two primary hospitals for whom a “stroke code” was activated were included; in-house strokes and stroke code activations from satellite facilities were excluded. Baseline characteristics, frequency of rt-PA, rt-PA exclusions, and rt-PA time metrics were compared between patients who did or did not require IS. Analyses utilized ANOVA, t-Test, Brown-Mood Median test, or Pearson’s Chi-squared test as appropriate.
Results
There were a total of 4,302 patients with stroke codes between 1/1/2011 and 4/1/2021 (Fig. 1). Patients from satellite facilities (n = 1,654), who were in-house stroke codes (n = 214), or with incomplete rt-PA datasets (n = 237) were excluded. Of 2,191 patients remaining, 81 had a documented need for IS. rt-PA was administered in 9 IS and 358 non-IS patients.
Fig. 1. Flowchart of patient inclusion and exclusion criteria
Baseline characteristics of IS patients are shown in supplemental Table (1) In IS patients, there were no differences in baseline characteristics between those who received rt-PA and those who did not including median score for NIHSS aphasia (0 ± 1 vs. 0 ± 1, p = 0.46). Baseline characteristics of subjects who received rt-PA are shown in supplemental Table (2) Median baseline NIHSS was higher in rt-PA group (9 ± 8 vs. 3 ± 9, p < 0.005). In patients who received rt-PA, there was a larger amount of Hispanic ethnicity (p < 0.01) and hyperlipidemia (p = 0.04) in patients requiring IS.
There were no rt-PA rate differences between those that did not and did require IS (17% vs. 11%, p = 0.22). In patients with final diagnosis acute ischemic stroke, patients excluded from rt-PA solely due to being out of the window were more likely to have required IS (59% vs. 35%, p = 0.003). Time metrics of rt-PA administration were not different in IS patients (Table 1).
Table 1rt-PA + Subset Analysis: time metrics by interpreter needsInterpreter StatusNumber of subjectsMedian time (minutes)P-Value Onset to Arrival IS (-)33463.0IS (+)876.0All34263.5P = 0.65 Arrival to Decision IS (-)31133.0IS (+)842.5All31934.0P = 0.45 Arrival to Treatment IS (-)33453.0IS (+)875.5All34253.5P = 0.48 Onset to Treatment IS (-)334128.0IS (+)8169.0All342128.5P = 0.46
Conclusions
Though this study found no significant difference in frequency or time metrics of rt-PA administration in patients requiring interpreter services during an acute stroke code, it adds to prior literature in showing that if patients required an interpreter, they were more likely to be solely excluded from rt-PA on the basis of time. Prior literature has shown disparities in discharge dispositions and outcomes [2–4]– our study suggests there may be disparities in how rapidly IS patients are being evaluated. Since rt-PA time metrics are not significantly different, one theory is that for patients with clear stroke syndromes, rt-PA may be offered under emergency consent. However, for mild strokes where further history is needed to elucidate degree of disability for rt-PA eligibility, requiring translator services may be a barrier to time-sensitive treatment.
One limitation of this study is the small single-center sample population. Based on our data, there was no significant difference in mRS between IS requiring patients who received or did not receive rt-PA. There was also a significantly larger amount of Hispanic ethnicity and HLD in patients requiring IS who received rt-PA. The clinical significance of these findings is unclear, but likely attributed to random variance in a small patient population where 30.3% of the community population is Hispanic [6]; of all patients in this time frame documented in need of interpreter, 77% required a Spanish interpreter.
We nevertheless add this study to the growing body of research on the impact that language has in a time sensitive field such as acute stroke care. Should our finding be replicated in other institutions or larger populations, this serves as a call to action for health care institutions to invest in language interpretation services. More work is planned in larger data sets to ensure resource availability and health equity to patients in need of interpreter services.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Erfe BL Siddiqui KA Schwamm LH Mejia NI Relationship between Language Preference and Intravenous Thrombolysis among Acute ischemic stroke patients J Am Heart Assoc 20165 e 00378210.1161/JAHA.116.00378227881425 PMC 5210419 · doi ↗ · pubmed ↗
- 2Rezania, F., Sharobeam, A., Mackey, E. (2018). Care and Outcome of Stroke patients with Language Barrier in a busy stroke centre. Neurology; 90.
- 3Shah BR Khan NAO’Donnell MJ Kapral MK Impact of Language barriers on Stroke Care and outcomes Stroke 20154681381810.1161/STROKEAHA.114.00792925657184 · doi ↗ · pubmed ↗
- 4Kilkenny MF Lannin NA Anderson CS Quality of life is poorer for patients with Stroke who require an interpreter: An observational Australian Registry Study Stroke 20184976176410.1161/STROKEAHA.117.01977129439194 · doi ↗ · pubmed ↗
- 5Anderson N Janarious A Liu S Flanagan LA Stradling D Yu W Language disparity is not a significant barrier for time-sensitive care of acute ischemic stroke BMC Neurology 20202036310.1186/s 12883-020-01940-933008325 PMC 7532579 · doi ↗ · pubmed ↗
- 6The City of San Diego Population. https://www.sandiego.gov/economic-development/sandiego/population. Accessed 4 March 2024.