Solid brain metastasis mimicking intracerebral hematoma on imaging
Satoshi Hori, Shoichi Nagai, Yoshinobu Maeda, Kohtaro Tsumura, Satoshi Kuroda

TL;DR
A patient with colon cancer had a brain metastasis that looked like a brain hemorrhage on imaging, leading to a rare and challenging diagnosis.
Contribution
This case highlights the rare presentation of brain metastasis mimicking intracerebral hematoma on CT scans.
Findings
The cerebellar lesion was surgically resected and confirmed to be a brain metastasis, not a hematoma.
The metastasis appeared as a hyper-dense lesion on CT, resembling spontaneous intracerebral bleeding.
This case emphasizes the importance of considering metastasis in patients with cancer presenting with brain lesions.
Abstract
A 79-year-old woman with a history of resection of the ascending colon cancer presented with conscious disturbance, dysarthria, nausea, and dizziness. Computed tomography (CT) revealed striking high-density lesions in the left cerebellum and left frontal lobe with slight perifocal edema. These lesions were suspected the coexistence of spontaneous cerebellar hemorrhage and frontal lobe metastasis, or multiple brain metastases with massive hematoma. Because of the mass effect of the cerebellar lesion and impaired consciousness, she underwent emergency resection of the cerebellar lesion which was found to be composed of grayish abnormal soft solid tissue and did not include an obvious hematoma mass. The pathological findings were consistent with brain metastasis from colon cancer. This is an impressive rare case of intraoperative solid brain metastasis with a clearly homogenous hyper-dense…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
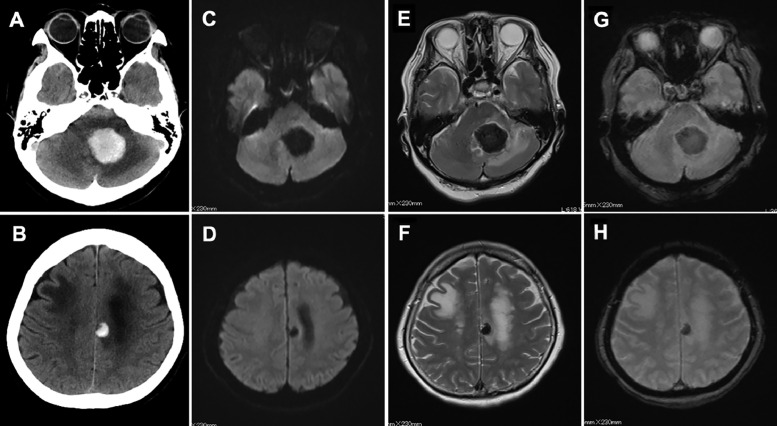 Figure 1
Figure 1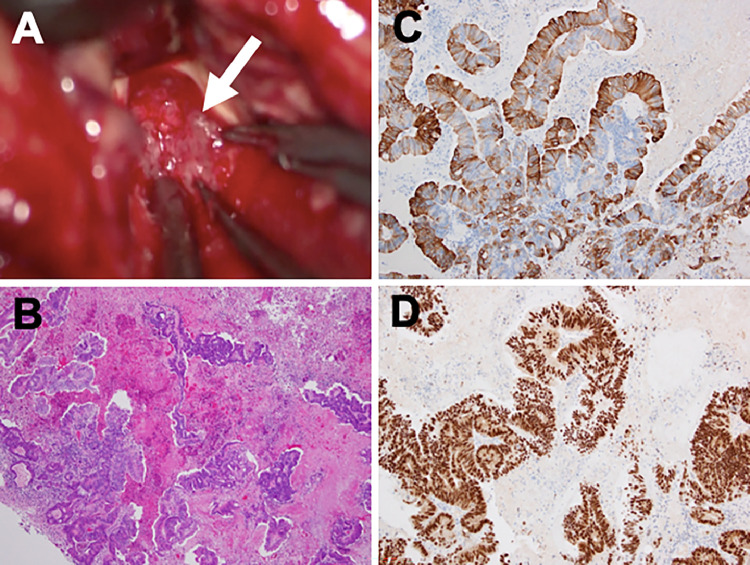 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBrain Metastases and Treatment · Glioma Diagnosis and Treatment · Management of metastatic bone disease
Introduction
Brain metastasis with adenocarcinoma usually presents as a region of low to moderate attenuation on plain computed tomography (CT). It is well known that calcification, hemorrhage, and the densely packed cell structures of tumors can increase pre-contrast attenuation. Calcification is conspicuous on the CT bone window images. Densely packed cell structures usually produce slightly higher density findings than gray matter. Hemorrhagic brain metastasis is relatively evident in the high-density region [1], which often needs to be discriminated from spontaneous cerebral hemorrhage for diagnosis. Here, we demonstrate an impressive case of intraoperative solid brain metastasis with a clearly homogenous hyper-dense CT appearance mimicking intracerebral hematoma.
Case presentation
A 79-year-old woman presented with consciousness disorder in May 2020 and was admitted to our hospital. She had previously undergone resection of adenocarcinoma of the ascending colon cancer in December 2017. Her postoperative course was uneventful, without local recurrence. Although the surgeon recommended aftercare chemotherapy, she refused it and was observed conservatively. On admission to our hospital, her Glasgow Coma Scale score was 13, and neurological examination revealed dysarthria, nausea, and dizziness. Computed tomography (CT) showed striking homogenous high-density lesions in the left cerebellum and frontal lobe with slight perifocal edema and edematous changes in the right frontal lobe (Figs. 1A and B). Lesions in the left cerebellum and frontal lobe presented as homogenous low intensity signals on diffusion-, T2-, and T2*-weighted magnetic resonance (MR) imaging, respectively (Figs. 1C-H). Based on these examinations and the patient's history, we suspected that the coexistence of spontaneous cerebellar hemorrhage and frontal lobe metastasis, or multiple brain metastasis with massive hematoma. Because of the mass effect of the cerebellar lesion and impaired consciousness, the patient was promptly sent to the operating room for emergency resection by posterior fossa craniotomy. Intraoperatively, the lesion was found to be composed of grayish abnormal soft solid tissue, which bled readily and did not include an obvious hematoma mass (Fig. 2A). Pathological findings revealed a well-differentiated papillotubular adenocarcinoma with hemorrhage in partial area (Fig. 2B). Immunohistochemistry was positive for cytokeratin 20 and CDX-2 (Figs. 2C and D). These findings were compatible with the diagnosis of metastatic brain tumor from colon cancer with partial hemorrhage.Fig. 1. Computed tomography image showing striking high-density lesions in the left cerebellum (A) and left frontal lobe, (B) with slight perifocal edema and edematous change in the right frontal lobe. Diffusion (C, D), T2 (E, F), and T2* (G, H) -weighted magnetic resonance imaging presented homogenous low intensity lesions in the left cerebellum and left frontal lobe, respectively.Fig 1. Fig. 2Intraoperative findings demonstrated that the lesion was found to be made up of grayish abnormal soft solid tissue which bled easily (white arrow), and obvious hematoma mass could not be confirmed (A). Pathological findings revealed a well differentiated papillotubular adenocarcinoma with hemorrhage in partial area (B). Hematoxylin and eosin staining, original magnification ×200. Immunohistochemical staining with Cytokeratin 20 (C) and CDX-2 (D) revealed positive staining in tumor cells, original magnification ×200.Fig 2
Discussion
This is an impressive rare case of solid brain metastasis mimicking intracerebral hematoma on imaging. Two unique previous reports demonstrated the cases of metastatic brain tumors with clearly high attenuation on CT mimicking hemorrhage, which present as non-hemorrhagic tissue intraoperatively and mucin-producing adenocarcinoma pathologically. It was indicated that lesions containing more mucinous material and less water could produce hyper-dense CT appearance [1,2]. Our case is similar to this situation of which there is an unexpected discrepancy between the preoperative radiological findings and intraoperative findings. However, it differs in terms of pathological findings that our case did not demonstrate the mucin-containing lesion and showed partial hemorrhage within the tumor. On the other hands, Kondziolka et al. described a retrospective review of hemorrhage from brain tumor which is categorized by size into macroscopic or microscopic, which showed that 14.6% of metastatic brain tumors develop intratumoral hemorrhage, macroscopic in 5.4% and microscopic in 9.2% of cases [3].
Based on these findings, our case may be consistent with the metastatic brain tumor with microscopic hemorrhage, which is the possible reason for mimicking intracerebral hemotoma on imaging in spite of intraoperative solid metastatic tumor. However, the radiological findings of brain metastasis with microscopic hemorrhage have not been well understood. It is usual for neurosurgeons to estimate the presence of a gross hematoma as one possibility when the region is shown as a strikingly high attenuation on plain CT. T1-weighted magnetic resonance imaging is considered to one of the useful sequences for diagnosing intracerebral hemorrhage, however, unfortunately, it was not taken in our case. Although the standard for diagnosing metastatic brain tumors is contrast MRI [4], this procedure cannot be performed immediately in all emergent patients. Neurosurgeons should keep in mind that greater awareness of several neuroimaging features is needed for accurate diagnosis and optimal surgical strategies.
Conclusions
We report an impressive case of intraoperative solid brain metastasis with a clearly homogenous hyper-dense CT appearance mimicking intracerebral hematoma. It may mean the presence of microscopic hemorrhage within the metastatic tumor.
Patient consent
Informed consent was obtained from the patient for the publication of this case report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Harrigan MR Gebarski SS Messe SR Blaivas M Mc Gillicuddy JE Metastatic adenocarcinoma to the brain mimicking hemorrhage: case repor Surg Neurol 5211999464910.1016/s 0090-3019(99)00048-810390172 · doi ↗ · pubmed ↗
- 2Ruelle A Macchia G Gambini C Andrioli G Unusual appearance of brain metastasis from adenocarcinoma of colon Neuroradiology 284198637510.1007/BF 003334533762922 · doi ↗ · pubmed ↗
- 3Kondziolka D Bernstein M Resch L Tator CH Fleming JF Vanderlinden RG Significance of hemorrhage into brain tumors: clinicopathological study J Neurosurg 676198785285710.3171/jns.1987.67.6.08523316531 · doi ↗ · pubmed ↗
- 4Zakaria R Das K Bhojak M Radon M Walker C Jenkinson MD The role of magnetic resonance imaging in the management of brain metastases: diagnosis to prognosis Cancer Imaging 1412014810.1186/1470-7330-14-825608557 PMC 4331840 · doi ↗ · pubmed ↗