The Feasibility of Omission of Postoperative Radiotherapy in Japanese Patients With Early Breast Cancer Treated With Breast-Conserving Surgery
Akihiro Nakashima, Hideya Yamazaki, Gen Suzuki, Kei Yamada, Norihiro Aibe, Takuya Kimoto, Koji Masui, Katsuhiko Nakatsukasa, Tetsuya Taguchi, Yasuto Naoi

TL;DR
This study suggests that skipping post-surgery radiation may be safe for low-risk Japanese breast cancer patients who had breast-conserving surgery.
Contribution
The study identifies a low-risk group of Japanese patients for whom omitting postoperative radiotherapy may be feasible without compromising outcomes.
Findings
Postoperative radiotherapy improved local control but not breast cancer-specific survival in the total population.
In low-risk patients, omitting radiotherapy did not significantly affect local recurrence rates or survival outcomes.
Equivalent outcomes were observed in low-risk patients with and without radiotherapy after propensity-score matching.
Abstract
Background This study was aimed at analyzing the impact of postoperative radiotherapy (PORT) after breast-conserving surgery (BCS) on Japanese patients with early-stage breast cancer and exploring the potential of PORT omission. Materials and methods Data from 794 patients with early-stage breast cancer (T1-2, N0-1), who underwent BCS with (n = 310) or without PORT (n = 484) were retrospectively analyzed. Local control (LC) rate and breast cancer-specific survival (BCSS) were compared between the groups that received and did not receive PORT in the whole cohort and low-risk cohort (i.e., the cohort with negative surgical margin, lymph node negativity, and estrogen receptor positivity, excluding young age of 49 or less), and in low-risk subgroup using propensity-score matching. Results PORT was associated with better LC but not BCSS in the total population. In the low-risk cohort,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
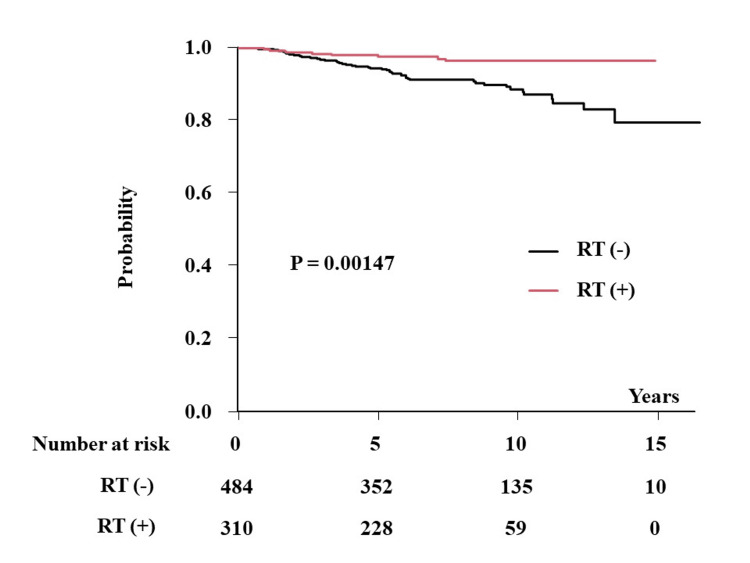 Figure 1
Figure 1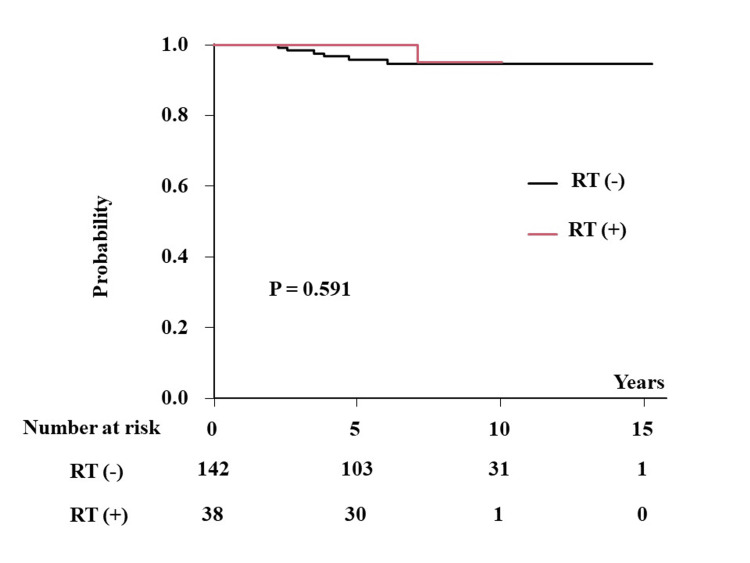 Figure 2
Figure 2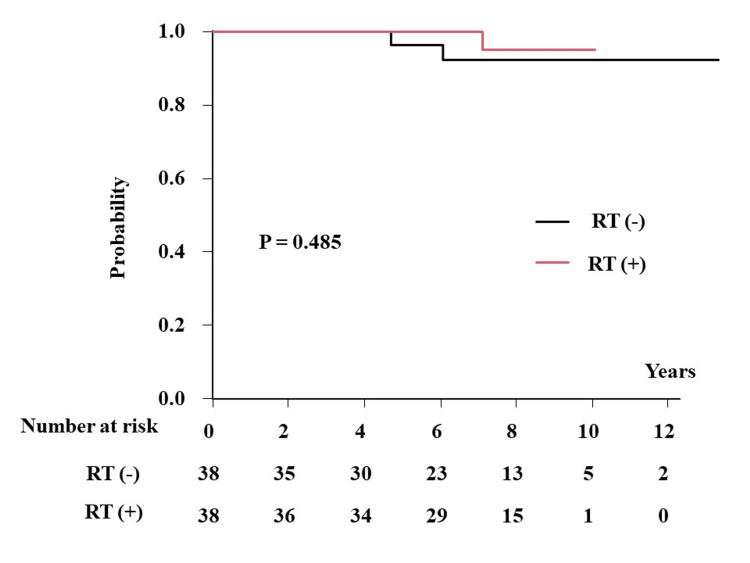 Figure 3
Figure 3| Factor | Group | Total (n = 794), No. (%) or median (range) | PORT (-) (n = 484), No. (%) or median (range) | PORT (+) (n = 310), No. (%) or median (range) | p-value* |
| Age | 53.00 (23.00, 89.00) | 56.00 (26.00, 89.00) | 50.00 (23.00, 82.00) | <0.001 | |
| cT | 1 | 371 (46.7) | 224 (46.3) | 147 (47.4) | 0.771 |
| 2 | 423 (53.3) | 260 (53.7) | 163 (52.6) | ||
| cN | 0 | 705 (88.8) | 421 (87.0) | 284 (91.6) | 0.05 |
| 1 | 89 (11.2) | 63 (13.0) | 26 (8.4) | ||
| ER | Positive | 555 (69.9) | 317 (65.5) | 238 (76.8) | 0.001 |
| Negative | 239 (30.1) | 167 (34.5) | 72 (23.2) | ||
| PgR | Positive | 433 (62.8) | 231 (57.9) | 202 (69.7) | <0.001 |
| Negative | 256 (37.2) | 253 (52.3) | 108 (34.8) | ||
| HER2 | Positive | 84 (10.6) | 50 (10.3) | 34 (11.0) | 0.813 |
| Negative | 710 (89.4) | 434 (89.7) | 276 (89.0) | ||
| Margin | Positive | 219 (27.6) | 77 (15.9) | 142 (45.8) | <0.001 |
| Negative | 575 (72.4) | 407 (84.1) | 168 (54.2) | ||
| Preoperative systemic therapy | Yes | 148 (18.6) | 88 (18.2) | 60 (19.4) | 0.709 |
| No | 646 (81.4) | 396 (81.8) | 250 (80.6) | ||
| Adjuvant chemotherapy | Yes | 159 (20.0) | 95 (19.6) | 64 (20.6) | 0.785 |
| No | 635 (80.0) | 389 (80.4) | 246 (79.4) | ||
| Adjuvant hormonal therapy | Yes | 331 (41.7) | 184 (38.0) | 147 (47.4) | 0.01 |
| No | 463 (58.3) | 300 (62.0) | 163 (52.6) | ||
| Follow-up period (months) | 91.0 (6.6, 197.8) | 96.8 (6.6, 197.8) | 88.9 (6.6, 178.8) | 0.005 |
| Factor | Group | Total (n = 794), No. (%) | RT (-) (n = 484), No. (%) | RT (+) (n = 310), No. (%) | p-value* |
| Local failure | Yes | 55 (6.9) | 46 (9.5) | 9 (2.9) | <0.001 |
| Lymph node recurrence | Yes | 23 (2.9) | 13 (2.7) | 10 (3.2) | 0.669 |
| Distant metastasis | Yes | 30 (3.8) | 19 (3.9) | 11 (3.5) | 0.851 |
| Cause of death | Death of breast cancer | 21 (2.6) | 14 (2.9) | 7 (2.3) | 0.751 |
| Other causes of death | 5 (0.6) | 5 (1.0) | 0 (0.0) | 0.181 |
| Outcome | Variable | Strata | Hazard ratio (95% CI) | p-value* |
| LC | ER | Positive vs. negative | 0.34 (0.16-0.73) | 0.005 |
| RT | Yes vs. no | 0.25 (0.11-0.58) | 0.001 | |
| BCSS | cT | 1 vs. 2 | 4.69 (1.05-20.8) | 0.041 |
| OS | cT | 1 vs. 2 | 6.67 (1.52-29.2) | 0.011 |
| Factor | Group | RT (-) (n = 142), No. (%) or median (range) | RT (+) (n = 38), No. (%) or median (range) | p-value* |
| Age | 62.00 (50.00, 87.00) | 57.00 (50.00, 81.00) | 0.007 | |
| cT | 1 | 71 (50.0) | 20 (52.6) | 0.856 |
| 2 | 71 (50.0) | 18 (47.4) | ||
| PgR | Positive | 88 (63.3) | 31 (81.6) | 0.034 |
| Negative | 51 (36.7) | 7 (18.4) | ||
| HER2 | Positive | 11 (8.0) | 4 (10.5) | 0.527 |
| Negative | 131 (92.3) | 34 (89.5) | ||
| Preoperative systemic therapy | Yes | 20 (14.1) | 7 (18.4) | 0.609 |
| No | 122 (85.9) | 31 (81.6) | ||
| Adjuvant chemotherapy | Yes | 7 (4.9) | 1 (2.6) | 1 |
| No | 135 (95.1) | 37 (97.4) | ||
| Adjuvant hormonal therapy | Yes | 67 (47.2) | 27 (71.1) | 0.01 |
| No | 75 (52.8) | 11 (28.9) | ||
| Follow-up period (months) | 91.35 (8.10, 183.30) | 88.80 (14.90, 120.80) | 0.481 |
| Factor | Group | RT (-) (n = 38), No. (%) or median (range) | RT (+) (n = 38), No. (%) or median (range) | p-value* |
| Age | 55.00 (50.00, 77.00) | 57.00 (50.00, 81.00) | 0.399 | |
| cT | 1 | 18 (47.4) | 20 (52.6) | 0.819 |
| 2 | 20 (52.6) | 18 (47.4) | ||
| PgR | Positive | 29 (76.3) | 31 (81.6) | 0.779 |
| Negative | 9 (23.7) | 7 (18.4) | ||
| HER2 | Positive | 5 (13.2) | 4 (10.5) | 1 |
| Negative | 33 (86.8) | 34 (89.5) | ||
| Preoperative systemic therapy | Yes | 13 (34.2) | 7 (18.4) | 0.192 |
| No | 25 (65.8) | 31 (81.6) | ||
| Adjuvant chemotherapy | Yes | 3 (7.9) | 1 (2.6) | 0.615 |
| No | 35 (92.1) | 37 (97.4) | ||
| Adjuvant hormonal therapy | Yes | 26 (68.4) | 27 (71.1) | 1 |
| No | 12 (31.6) | 11 (28.9) | ||
| Follow-up period (months) | 88.50 (8.10, 160.00) | 88.80 (14.90, 120.80) | 0.685 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Cancer Treatment Studies · Global Cancer Incidence and Screening · Breast Lesions and Carcinomas
Introduction
In the world, female breast cancer has become the second most often diagnosed cancer. In 2022, there were expected to be 2.3 million new cases [1]. Postoperative radiotherapy (PORT) is the established standard of care following breast-conserving surgery (BCS) for early breast cancer because it enhances local recurrence-free survival and reduces cancer-specific mortality, as supported by several randomized clinical trials (RCTs) and meta-analyses [2-4].
Some patients do not undergo PORT for various reasons, including concerns regarding secondary cancer and side effects, such as breast pain, dermatitis, risk for heart and lung complications, lack of informed consent, or fragile condition [5,6]. Therefore, omission of PORT has been explored in several low-risk groups, more specifically in those with early disease(s) (T1-2, N0-1), advanced age, and/or hormone positivity, in part, due to the limited benefits of PORT [6-13]. Recently, several retrospective studies and prospective RCTs in Western countries have indicated that omitting PORT in elderly patients is a viable option [6-13]. For example, the PRIME II trial on BCS with or without irradiation demonstrated the safety of the omission of PORT in women ≥65 years of age with T1 or T2 tumors (≤3 cm) and node-negative, estrogen receptor (ER)-positive breast cancer [6]. However, such evidence is limited in non-Asian cohorts, and Asian and non-Asian people differ in the effectiveness and toxicity of systemic therapy [14].
Therefore, we conducted a retrospective review of data housed in our database. This study analyzed the impact of PORT on Japanese patients with early breast cancer who underwent BCS to explore the potential of omitting PORT.
Materials and methods
We conducted a retrospective analysis of 1137 Japanese patients who had BCS for early breast cancer at the Department of Endocrine and Breast Surgery, Kyoto Prefectural University of Medicine, between January 2001 and May 2016. We included histologically confirmed breast cancer patients with clinical T1-2N0-1M0 disease, identified based on available and accessible data on the T, N, and M classifications according to the National Comprehensive Cancer Network (NCCN) risk classification [15] and hormonal receptor status. We excluded patients with distant metastases at diagnosis (n = 10), Tis or 3-4 (n = 165), node-positive (N2 or more, n = 152), short follow-up within six months without any failure (n = 11), and incomplete PORT discontinuation before the planned dose (n = 5). A total of 794 patients who underwent BCS with or without PORT were eligible for analysis. Patient characteristics are shown in Table 1.
A total dose of 50 Gy was administered as PORT in 2 Gy fractions daily in two opposing tangential fields to the residual breast tissue utilizing generally 6-MV photons. Cases with a pathologically positive surgical margin received an additional boost radiotherapy with 10 Gy in five fractions using electron beams (4-12 MeV) in general.
In general, adjuvant endocrine therapy for early breast cancer in pre-menopausal women included tamoxifen (20 mg/day) ± goserelin (3.6 mg/four weeks) or leuprorelin (3.75 mg/four weeks), whereas in post-menopausal women, it included tamoxifen (20 mg/day), aromatase inhibitors (anastrozole 1 mg/day or letrozole 2.5 mg/day), or toremifene (40 mg/day). The standard administration period of adjuvant endocrine therapy was five years or more (up to 10 years). Preoperative systemic therapy mainly consisted of the cyclophosphamide/epirubicin/fluorouracil and taxane regimens, with or without trastuzumab.
The primary endpoint was local control (LC), and local recurrence was defined as any cancer in the scar or the same breast (including a second primary tumor in the same breast) [6]. The secondary endpoints were breast cancer-specific survival (BCSS) rate and overall survival (OS) rate. We examined factors influencing LC, BCSS, and OS in the total population. Next, we compared LC, BCSS, and OS between the groups that received PORT (RT (+)) or did not receive PORT (RT (-)) in the total population. We added subgroup analysis of the low-risk cohort and a propensity-matched group in the low-risk cohort, which consisted of surgical margin-free (>5 mm), lymph node-negative, and ER-positive cases, and age 50 or more according to previous literature [6-10].
Informed consent was obtained by providing an opt-out form on the website, and patients who refused to participate were excluded (number of people excluded = 0). We also received permission to analyze and publish data according to the guidelines of the Institutional Ethics Committee (approval number: ERB-C-1363-1). We published another article [16] using a different population of the same database with this approval number.
Statistical analyses
The EZR (Easy R) statistical package was used for statistical analyses [17]. Fisher's exact test and Student's t-test were used to analyze percentages and normally distributed data, respectively. The Mann-Whitney U test was used for comparisons of skewed data. Kaplan-Meier analysis was performed to analyze the LC, BCSS, and OS. The time to event was determined from the day of surgery. Cutoff values were set as the median or mean if they were not specified. Multivariate Cox regression models were applied for LC, BCSS, and OS. The candidate covariates in these models were age (≤ 65 vs. > 65), clinical T classification (T1 vs. T2), clinical and pathological N classification, estrogen receptor (ER) status, progesterone receptor (PgR) status, human epidermal growth factor receptor 2 (HER2) status, margin status, preoperative systemic therapy, adjuvant chemotherapy, and adjuvant hormonal therapy and PORT. Variable selection for multivariate models was conducted using the stepwise method with the Akaike information criterion. Statistical significance was set at p < 0.05.
As we did not randomize the included patients, there were unbalanced baseline characteristics that could lead to selection bias. Therefore, this selection bias influenced the decision to administer or not administer PORT. We used the propensity score, which was defined as the probability of being assigned to the RT (-) or RT (+) group, given the patient characteristics. The logistic regression model was used to calculate the propensity scores, considering the baseline covariates mentioned above excluding PORT. After the initial analysis of the whole and low-risk cohorts, we performed a propensity score-matched pair analysis (a caliper value of 0.2 was used) to minimize bias related to the choice of and allocation to the RT (-) or RT (+) groups in the low-risk cohort. Nine factors for the low-risk cohort prescribed before were used to create a 1:1 matched cohort assigned to the RT (+) and RT (-) groups.
Results
Patient characteristics and factors influencing local control, breast cancer-specific survival, and overall survival in the total population
The median follow-up was 7.8 years (range: six months to 16.5 years). Patient characteristics and treatments are summarized in Table 1. The PORT group consisted of younger patients with more advanced disease stages and positive margins. The outcome after BCS is depicted in Table 2. PORT was associated with better LC in the total population.
The incidence of local recurrence was 11.3% (95% CI = 8.3-15.4%) and 3.7% (95% CI = 1.9-7.3%) at 10 years (5.6% (5.8-8.2) and 2.5% (1.2-5.2%) at five years) in patients without and with PORT, respectively (p = 0.00147) (Figure 1). BCSS was 96.6% and 95.9% at 10 years (p = 0.924) (98.6% (96.9-99.4%) and 98.5% (96.1-99.4%) at five years) in patients with and without PORT, respectively. OS was 95.3% and 95.9% at 10 years (p = 0.521) (95.3% (92.0-97.3%) and 95.9% (90.5-98.3%) at five years) in patients with and without PORT, respectively. Multivariate Cox analysis revealed that ER positivity and PORT administration were statistically significant predictors of LC (Table 3). Regarding BCSS and OS, PORT administration was not a significant predictor.
Local control after breast-conserving surgery according to the presence or absence of postoperative radiotherapy.RT: radiotherapy.
Impact of PORT on the low-risk cohort
A comparison of patient characteristics is shown in Table 4. The PORT group comprised younger patients with more advanced disease stages who underwent adjuvant hormonal therapy.
The incidence of local recurrence was 5.3% (95% CI = 2.4-11.4%) and 4.8% (95% CI = 1.5-14.7%) at 10 years (0% and 4.2% (1.8-9.8%) at five years) in patients without and with PORT, respectively (p = 0.591) (Figure 2). BCSS and OS were considered the same because there was no other cause of death; three and one deaths were due to breast cancer in patients without and with PORT, respectively. Therefore, the BCSS and OS were 96.8% and 97.4% at 10 years (100% and 99.1% (93.7-99.9%) at five years) in patients without and with PORT, respectively (p = 0.906).
LC in the low-risk cohort according to the presence or absence of postoperative radiotherapy.LC: local control; RT: radiotherapy.
Impact of PORT on the low-risk cohort according to propensity score-matched pair analysis
A propensity score-matched pair analysis was performed in the low-risk cohort. A well-matched set of 38 patient pairs in each group was generated, and the background comparison is shown in Table 5.
The incidence of local recurrence was 4.8% (95% CI = 1.7-29.3%) and 7.8% (95% CI = 2.0-27.8%) at 10 years (0% and 1.1% (0.1-6.3%) at five years) in patients with and without PORT, respectively (p = 0.485) (Figure 3). The BCSS and OS were considered the same and were 96.6% and 94.1% at 10 years (100% and 96.6% (77.9-99.5%) at five years) in patients without and with PORT, respectively (p = 0.918).
LC in matched pair population in the low-risk cohort according to the presence or absence of postoperative radiotherapy.LC: local control; RT: radiotherapy.
Discussion
We examined the effect of PORT after BCS in Japanese patients with early T1-2N0-1 breast cancer to explore the impact and feasibility of omitting this therapy. We found that PORT reduced local recurrence in the total population but did not affect BCSS or OS. In the low-risk cohort, PORT did not affect all outcomes.
Our data are consistent with those of previous studies investigating LC, BCSS, and OS. For example, a meta-analysis by the Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) [4] revealed a 10-year risk for local recurrence of 10.0% and 29.7% for the PORT group and controls, respectively, in women with node-negative disease and a 10-year risk for ipsilateral local recurrence of 13.1% and 46.5% for the PORT group and controls, respectively, in women with node-positive disease. According to our data, the 10-year risk for local recurrence was 9.9% and 13.6% in the PORT group and controls, respectively, among women with node-negative disease and 11.6% and 13.1% in the PORT group and the controls, respectively, among women with node-positive disease. Thus, this trend is consistent with those reported in previous investigations, although relatively better outcomes were apparent in our population [3].
Generally, guidelines including the American NCCN recommend PORT after BCS, except in patients at low risk [15]. The omission of PORT in patients with biologically low-risk tumors has been explored and established based on the presence of several low-risk biological features [6-13]; these features are generally present in elderly patients because more elderly women exhibit favorable tumor biology with low-grade, hormone receptor-positive (i.e., ER or PgR) and HER-2-negative tumors [12]. As the European Society of Breast Cancer Specialists (EUSOMA) guidelines suggest an accepted maximum rate of locoregional recurrence of 10% at 10 years for omitting PORT in elderly patients, we thought that younger patients could not be a good candidate for omitting PORT [18].
Previous studies have explored the omission of PORT. Chesney et al. conducted a systemic review and meta-analysis that included four RCTs of early-stage breast cancer treated with BCS and tamoxifen and demonstrated that PORT reduced the risk for breast and axillary recurrence in elderly women aged >70 years but did not impact distant recurrence or overall survival [11]. Kunkler et al. recently reported the highly anticipated 10-year results of the PRIME II trial and revealed that omission of PORT did not affect survival after BCS in women aged ≥65 years with T1-2 (tumors ≤ 3 cm), node-negative, and ER-positive breast cancer [6]. The authors reported a 10-year risk for local recurrence of 0.9% and 9.5% along with a 10-year OS of 80.7% and 80.8% in the PORT and control groups, respectively. Our data for the low-risk cohort exhibited local recurrence rates of 4.8% and 5.3% at 10 years and OS of 97.4% and 96.8% at 10 years in patients with and without PORT, respectively [6]. Our results regarding the benefit of omission of PORT are consistent with those of previous omission trials [6-10].
The present study had some limitations. First, as this study was not a randomized prospective study, it was difficult to address all possible biases. Our data were retrospectively obtained from a small size of the subgroups, a heterogeneous population, which may have introduced selection bias in aspects including the choice of chemotherapeutic agents. Next, histological details, such as the presence of lymph vascular invasion or the nuclear grade, were not assessed due to a lack of such information in the database. Patients with lymph vascular invasion or nuclear grade 3 tumors are not suitable as candidates for PORT omission. We speculate that in selecting suitable patients for omitting PORT, clinicians were cautious in enrolling patients with grade 3 tumors or lymphovascular invasion because the risk of local recurrence is doubled in such patients. Third, the issue of the margin status has room for discussion. Because we identified positive margins as ≤5 mm, several patients with positive margins in our cohort may have been categorized as having negative margins in other studies. Fourth, data on the prescribed dose and duration of systemic therapy (e.g., primary systemic therapy and adjuvant therapy) are lacking. At last, we could not assess the impact of the hormonal status of the patient because we did not include information on premenopausal or postmenopausal women. In the future, analyses based on genomic background intrinsic subtypes, such as luminal types, epidermal growth factor, and BRCA [5,15], which are routinely used in clinical practice, should be considered.
Conclusions
PORT improved LC in the total population, but not BCSS or OS. In the low-risk group analysis (negative surgical margin, lymph node negativity, estrogen receptor positivity, and age 50 years or more), LC, BCSS, and OS were equivalent between RT (+) and RT (-) groups, including propensity-matched comparison. Therefore, this study showed that the omission of PORT could be a treatment option for low-risk Japanese patients. Further multi-center prospective studies are warranted to validate these findings and reduce the unnecessary burden of PORT for patients and institutions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J Clin Bray F Laversanne M Sung H Ferlay J Siegel RL Soerjomataram I Jemal A 2292637420243857275110.3322/caac.21834 · doi ↗ · pubmed ↗
- 2Does locoregional radiation therapy improve survival in breast cancer? A meta-analysis J Clin Oncol Whelan TJ Julian J Wright J Jadad AR Levine ML 122012291820001071529110.1200/JCO.2000.18.6.1220 · doi ↗ · pubmed ↗
- 3Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials Lancet Darby S Mc Gale P Correa C 1707171637820112201914410.1016/S 0140-6736(11)61629-2PMC 3254252 · doi ↗ · pubmed ↗
- 4Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials Lancet Clarke M Collins R Darby S 208721063662005 https://pubmed.ncbi.nlm.nih.gov/16360786/1636078610.1016/S 0140-6736(05)67887-7 · doi ↗ · pubmed ↗
- 5Breast cancer biology: clinical implications for breast radiation therapy Int J Radiat Oncol Biol Phys Horton JK Jagsi R Woodward WA Ho A 233710020182925477610.1016/j.ijrobp.2017.08.025 · doi ↗ · pubmed ↗
- 6Breast-conserving surgery with or without irradiation in early breast cancer N Engl J Med Kunkler IH Williams LJ Jack WJ Cameron DA Dixon JM 58559438820233679115910.1056/NEJ Moa 2207586 · doi ↗ · pubmed ↗
- 7Lumpectomy plus tamoxifen with or without irradiation in women age 70 years or older with early breast cancer: long-term follow-up of CALGB 9343 J Clin Oncol Hughes KS Schnaper LA Bellon JR 238223873120132369042010.1200/JCO.2012.45.2615 PMC 3691356 · doi ↗ · pubmed ↗
- 8Tamoxifen with or without breast irradiation in women 50 years of age or older with early breast cancer N Engl J Med Fyles AW Mc Cready DR Manchul LA 96397035120041534280410.1056/NEJ Moa 040595 · doi ↗ · pubmed ↗