Endoscopic papillectomy of a rare isolated ampullary hamartoma
Ahmed Altonbary, Fady Sabry, Hazem Hakim, Amr Elrabat, Wagdi Elkashef

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
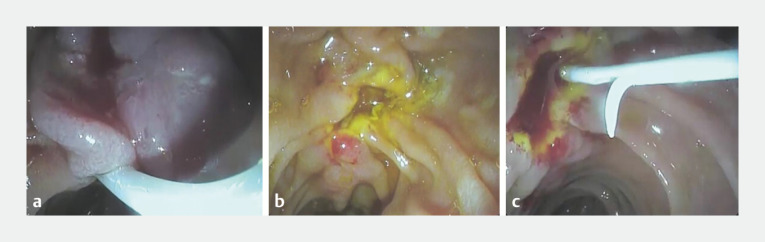 Fig. 1
Fig. 1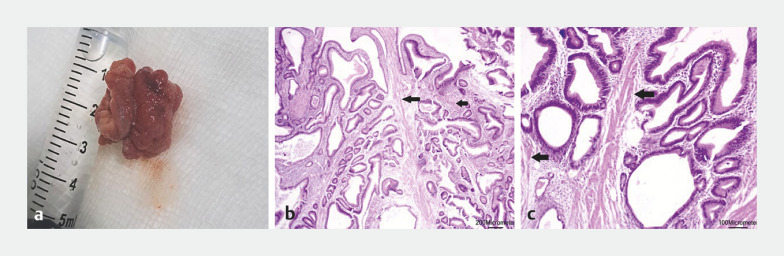 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSoft tissue tumor case studies · Pancreatic and Hepatic Oncology Research · Neuroendocrine Tumor Research Advances
An isolated hamartoma in the ampulla of Vater is very rare, with only seven cases reported in the literature in patients without either Peutz–Jeghers or Cowdens syndrome as an underlying disease 1 . Herein, we report a rare case of isolated ampullary hamartoma diagnosed by endoscopic papillectomy.
A 69-year-old man was admitted to our hospital with recurrent abdominal pain and jaundice. Magnetic resonance cholangiopancreatography (MRCP) revealed a 2-cm ampullary mass, with dilatation of the common bile duct (CBD) to 12 mm and a normal pancreatic duct (PD). Laboratory investigations were unremarkable, apart from elevated serum bilirubin. Endoscopic ultrasound (EUS) evaluation showed a 2-cm hypoechoic mass with no intraductal extension or lymphadenopathy and intact muscularis propria.
Endoscopic papillectomy was performed as follows ( Video 1 ). After the lesion had been carefully assessed using the duodenoscope, the snare tip was anchored at the apex of the papilla then slowly opened and drawn down over the mass. The snare was then tightly closed without losing contact with the point of impaction above ( Fig. 1 a ). The entrapped mass was checked to ensure it was independently mobile from the duodenal wall before blend current was applied to resect the lesion en bloc. The resected specimen was retrieved by snaring and the resection bed was carefully examined ( Fig. 1 b ). The PD was then canulated, and this was followed by insertion of a pancreatic stent (5 cm, 5 Fr) ( Fig. 1 c ). No adverse events were reported during or after the procedure. Pathologic examination of the resected specimen revealed a polypoid lesion showing irregular glandular formations and strands of smooth muscle fibers, consistent with an ampullary hamartoma ( Fig. 2 ). Colonoscopy was then performed, which was clear up to the terminal ileum.
Endoscopic images during endoscopic papillectomy of an ampullary hamartoma showing: a a snare being tightly closed over the ampullary mass; b the clean resection bed; c a pancreatic stent in situ.
Pathologic examination of the retrieved specimen revealed: a on macroscopic view, a polypoid lesion; b, c the polypoid lesion with irregular glandular formations and strands of smooth muscle fibers (arrows) on a hematoxylin and eosin (H&E)-stained section, magnification: b × 40; c × 100.
Endoscopic papillectomy of an ampullary hamartoma.Video 1
Endoscopy_UCTN_Code_TTT_1AR_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.