Gastric endoscopic submucosal dissection through a gastrostomy using a newly developed thin endoscope
Satoki Shichijo, Mori Hitoshi, Koji Higashino, Noriya Uedo, Tomoki Michida

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1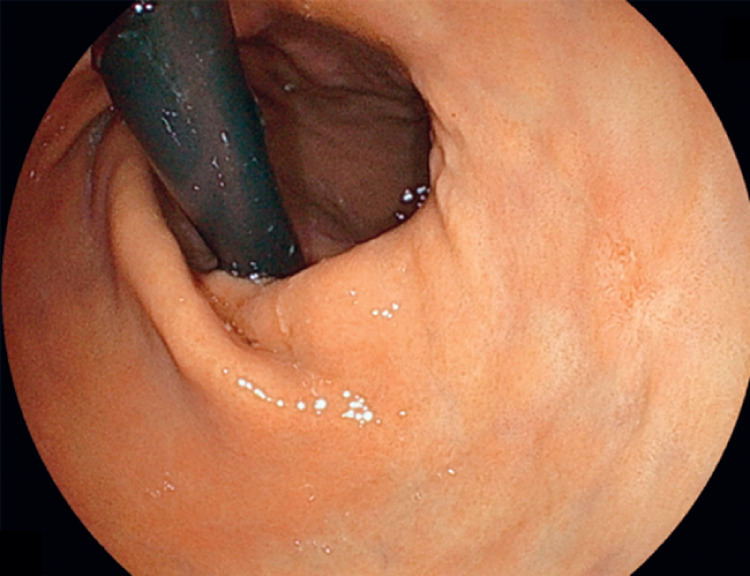 Fig. 2
Fig. 2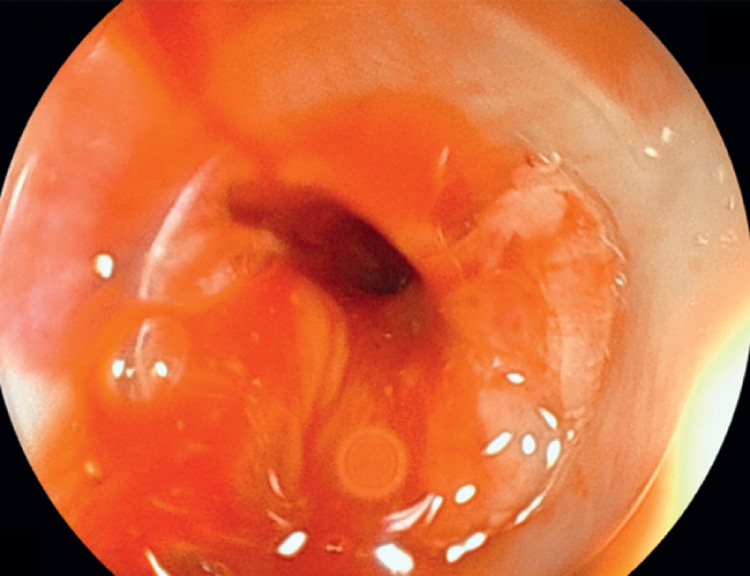 Fig. 3
Fig. 3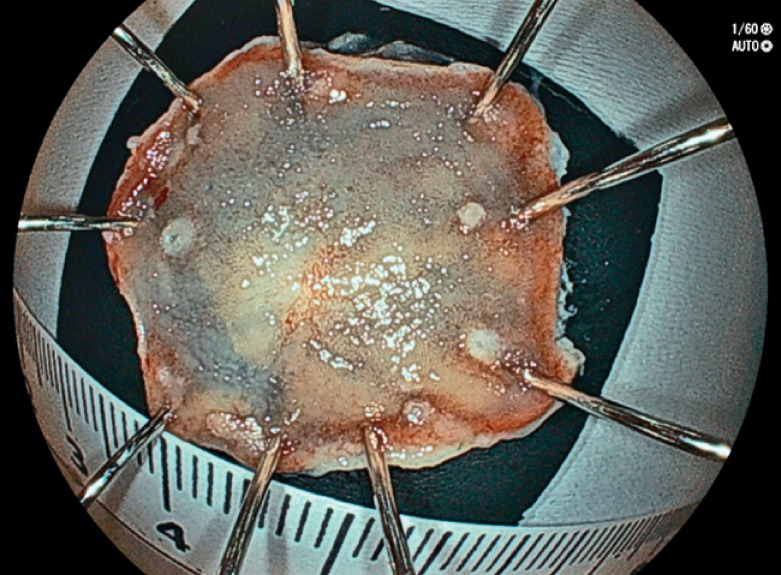 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Esophageal and GI Pathology · Dysphagia Assessment and Management
A 76-year-old man underwent follow-up endoscopy after undergoing curative endoscopic submucosal dissection (ESD) for esophageal cancer 1 . He had a past history of advanced pharyngeal cancer, which had been treated with chemoradiotherapy, and had a percutaneous endoscopic gastrostomy because of persistent trismus ( Fig. 1 ). The follow-up endoscopy, performed via transnasal endoscopy, revealed a 6-mm depressed lesion in the lesser curvature of the antrum, and a biopsy confirmed adenocarcinoma ( Fig. 2 ). ESD using a newly developed endoscope 2 3 was performed to treat the gastric cancer.
Photograph showing persisting trismus after chemoradiotherapy for advanced pharyngeal cancer.
Endoscopic images showing a slightly depressed lesion at the lesser curvature of the antrum viewed on transnasal endoscopy.
First, the catheter through the gastrostomy was removed and an endoscope with a diameter of 7.9 mm (EG-840TP; Fujifilm, Tokyo, Japan) was inserted through the gastrostomy ( Fig. 3 ; Video 1 ). Circumferential marking, mucosal incision, and circumferential incision were performed, and submucosal dissection was subsequently performed until the tumor was resected en bloc ( Fig. 4 ), taking 9 minutes. The lesion was retrieved through the gastrostomy, and a new catheter was placed into the gastrostomy using a guidewire. The final pathologic diagnosis was a 6×6-mm, 0–IIc, well-differentiated tubular adenocarcinoma, pT1a, pUL0, ly0, v0, pHM0, pVM0.
Gastric endoscopic submucosal dissection is performed through a gastrostomy using a newly developed thin endoscope.Video 1
An endoscope was inserted through gastrostomy.
Macroscopic appearance of the lesion, which was resected en bloc.
Although the newly developed endoscope has a large working channel of 3.2 mm and offers wide angles (up 210°; down 160°), its small width of 7.9 mm enabled efficient ESD to be performed through the gastrostomy without dilation 1 .
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shichijo S Kawakami Y Higashino K Retrograde esophageal endoscopic submucosal dissection through a gastrostomy Endoscopy 202355 E 507E 50836894142 10.1055/a-2037-5075 PMC 9998235 · doi ↗ · pubmed ↗
- 2Shichijo S Miyake M Ishihara R Usefulness of the ultrathin endoscope with a newly developed knife for complex esophageal endoscopic submucosal dissection Video GIE 2023818318510.1016/j.vgie.2023.01.00637197164 PMC 10183485 · doi ↗ · pubmed ↗
- 3Shichijo S Kawakami Y Kizawa A Endoscopic submucosal dissection for a duodenal polyp at the upper aspect of the duodenal bulb using a newly developed endoscope Video GIE 2023850951110.1016/j.vgie.2023.07.01638155827 PMC 10751466 · doi ↗ · pubmed ↗