Ferrer Adjustable Speaking Valve for Early Phonation in a Deconditioned Patient
Rafael Cartaya, Syed A. A Rizvi, Viviane Manara, Mari L Tesch, Rahaghi Franck

TL;DR
A new adjustable speaking valve helped a patient with a long-term tracheostomy to speak and breathe more effectively.
Contribution
The introduction of the Ferrer adjustable speaking valve allows for earlier phonation and diaphragm exercise in deconditioned patients.
Findings
The patient tolerated the Ferrer valve at 20% closure and progressed to 50% closure with partial phonation.
The valve was used safely for 23 days, suggesting its potential for early communication and respiratory function improvement.
Abstract
A patient with multiple comorbidities and an eight-year history of tracheostomy was being treated for tracheitis. At this point, she became incapable of using regular speaking valves, and multiple attempts to reintroduce the speaking valve failed. A Ferrer adjustable speaking valve (FASV) was designed with gradations of outflow closure, allowing air to go through the vocal cords for phonation. The FASV was offered to her through the compassionate use program at the FDA. At 20% initial closure, the patient was able to tolerate the valve and was advanced to 50% closure, at which point she could phonate partially. The use of the valve was terminated at the time of her transfer, 23 days after the initiation of use. This suggests the safety and possible efficacy of using an adjustable speaking valve earlier than regular valves, allowing patients to communicate earlier and further exercise…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
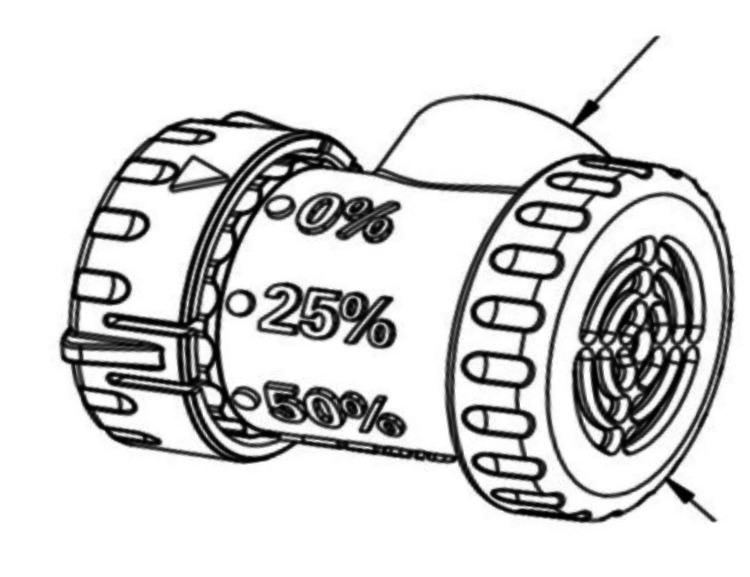 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVoice and Speech Disorders · Tracheal and airway disorders · Dysphagia Assessment and Management
Introduction
Patients with tracheostomy cannot phonate without some degree of tube occlusion during exhalation. This resistance is provided by a speaking valve, a one-way valve that provides minimal resistance during inspiration and shuts down for expiration, thus allowing phonation. Unfortunately, due to weakness, multiple tries are needed before the patient can tolerate this setup, as they would not be able to tolerate the full closure of the outflow path through the tracheostomy or even the additional resistance of the inflow path after the valve is added. Once the valve is in place, the patient can phonate with every breath if needed. Complete occlusion trials generally follow this in anticipation of tracheostomy discontinuation. A large body of evidence supports using speaking valves to improve communication in tracheostomy patients [1].
Case presentation
Ms. J is a 46-year-old female with chronic respiratory failure s/p tracheostomy as well as a history of subglottic stenosis, restrictive lung disease 2/2 to severe kyphoscoliosis, Sjogren syndrome, antiphospholipid syndrome, systemic lupus erythematosus, major depression, and anxiety. She had a tracheostomy eight years prior.
She was being treated for possible pneumonia/tracheitis and finished a course of Cefepime. At that time, she could not tolerate multiple trials of a speaking valve. She self-occluded, by her finger, her tracheostomy site to communicate and make her needs known. Before starting the adjustable speaking valve trials, she was being treated for recurrent cellulitis of the right-sided peri-stomal tracheal area with an associated complicated boil. When she first started using the Ferrer adjustable speaking valve (FASV), she started at 20% occlusion and could only speak one word per breath. As her pulmonary status improved, the percent occlusion increased to 50%, and she improved to speak two words per breath consistently. She made continuous improvements as expected until the trials were placed on hold as she was preparing for transfer to another facility after 23 days of use. Of note was that the boil and cellulitis resolved and did not exacerbate while she continued with the Ferrer-adjustable speaking valve trials. No complications or adverse events were noted from the use of the FASV. In this case, the adjustable outflow obstruction allowed earlier use of a valve for phonation.
Discussion
The Ferrer Adjustable Speak Easy-Valve (FASV), made by Dr. Ferrer Biopharma, is a compact, lightweight apparatus engineered to fit the universal 15 mm hub of tracheostomy tubes (Figure 1). The FASV’s design includes a wider diameter pathway, preventing the restriction of inhaled air, a problem that may arise with other one-way speaking valves. The FASV can be used interchangeably by tracheostomized and ventilator-dependent patients. They can be easily adapted for use in line with a ventilator circuit and can be used alongside closed suctioning systems, swivel adapters, supplemental oxygen, and humidification.
*Ferrer adjustable speaking valveLong arrow: Attachment to patients tracheostomy hub. Short arrow: Inflow diaphragm. Reprinted with permission of Dr. Ferrer Biopharma
A significant number of tracheostomized patients cannot tolerate the currently available speaking valves when they try them for the first time. Concurrently, about half of these patients require multiple trials before fully engaging with the device [2]. Studies indicate that most patients experience a feeling of suffocation when they first try the PMV [3]. In light of this, the FASV was designed to be set at an initial setting of 50% resistance/closure of the one-way outflow and meant to cap the valve to a complete 100% closure of the diaphragm. Once the one-way valve is closed, the outer part of the AV features an adjustable flow cylinder. The valve has been indexed for attenuating flow in 25% increments to 50%, 75%, and 100% (fully closed) using a knob instead of drilling holes (which can lead to inaccurate airflow) to improve tolerance [4,5].
Patients typically spend more than a week in the weaning process [6]. The FASV's initial benefit is that it enables earlier phonation. There is fair evidence that in-line speaking valves can accelerate phonation in those too weak for cannula deflation [7-9]. In addition, Martin et al. showed that placement of speaking valves within 24 hours is possible and safe [9,10]. The ultimate objective of FASV is to enhance patient satisfaction and reduce hospital length of stay by increasing diaphragmatic exertion and earlier successful decannulation.
The FASV is currently undergoing an FDA approval process. The FDA explicitly permitted the use of FASV in this patient under compassionate use.
Conclusions
Regular speaking valves are initially hard to tolerate by deconditioned patients and those with significant respiratory insufficiency. An adjustable (resistance) speaking valve allowed the gradual introduction of phonation to a patient who could not tolerate regular speaking valves. This led to better communication, greater patient satisfaction, and perhaps further exercise of the patient’s diaphragm.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Return of voice for ventilated tracheostomy patients in ICU: a randomized controlled trial of early-targeted intervention Crit Care Med Freeman-Sanderson AL Togher L Elkins MR Phipps PR 107510814420162685543010.1097/CCM.0000000000001610 · doi ↗ · pubmed ↗
- 2Tolerance of one-way in-line speaking valve trials in ventilator dependent children Int J Pediatr Otorhinolaryngol Althubaiti A Worobetz N Inacio J 11113115720223542987310.1016/j.ijporl.2022.111131 · doi ↗ · pubmed ↗
- 3Tracheostomy tube manometry: evaluation of speaking valves, capping and need for downsizing Clin Respir J Johnson DC Campbell SL Rabkin JD 814320092029836610.1111/j.1752-699X.2008.00100.x · doi ↗ · pubmed ↗
- 4Drilling speaking valves to promote phonation in tracheostomy-dependent children Laryngoscope Buckland A Jackson L Ilich T Lipscombe J Jones G Vijayasekaran S 2316232212220122277774610.1002/lary.23436 · doi ↗ · pubmed ↗
- 5Technique to improve tracheostomy speaking valve tolerance after head and neck free flap reconstruction Plast Reconstr Surg Glob Open Stranix JT Danziger KM Dumbrava VL Mars G Hirsch DL Levine JP 04201610.1097/GOX.0000000000001082 PMC 522263828293493 · doi ↗ · pubmed ↗
- 6Tracheostomy timing and the duration of weaning in patients with acute respiratory failure Crit Care Boynton JH Hawkins K Eastridge BJ O'Keefe GE 078200410.1186/cc 2885 PMC 52284715312227 · doi ↗ · pubmed ↗
- 7The use of tracheostomy speaking valves in mechanically ventilated patients results in improved communication and does not prolong ventilation time in cardiothoracic intensive care unit patients J Crit Care Sutt AL Cornwell P Mullany D Kinneally T Fraser JF 4914943020152559994710.1016/j.jcrc.2014.12.017 · doi ↗ · pubmed ↗
- 8Safety and feasibility of above cuff vocalisation for ventilator-dependant patients with tracheostomies J Intensive Care Soc Mc Grath BA Wallace S Wilson M Nicholson L Felton T Bowyer C Bentley AM 59652020193079276410.1177/1751143718767055 PMC 6376581 · doi ↗ · pubmed ↗