Status of COVID-19 Patients Treated With Extracorporeal Membrane Oxygenation in Japan: Nationwide Database Analysis
Tomoki Kuribara, Yusuke Asai, Norio Ohmagari, Isao Yokota

TL;DR
This study analyzed ECMO treatment outcomes for 196 Japanese COVID-19 patients, finding a 33.2% mortality rate and manageable complication rates compared to global data.
Contribution
The study provides the first nationwide analysis of ECMO-treated COVID-19 patients in Japan, offering detailed clinical and epidemiological insights.
Findings
Hospital mortality for ECMO-treated patients was 33.2%, with 23.0% discharged home.
Common complications included pneumothorax (9.7%) and stroke (4.6%).
38.3% of patients had worsened self-care ability at discharge.
Abstract
Background The report of epidemiological data on coronavirus disease 2019 (COVID-19) patients treated using extracorporeal membrane oxygenation (ECMO) in Japan has been limited. Our study seeks to fill the existing gap in knowledge by providing an in-depth analysis of the clinical epidemiological characteristics and diverse medical outcomes of COVID-19 patients treated with ECMO in Japan. Methods This study used the COVID-19 Registry Japan nationwide database. We included patients aged 18 years or older enrolled between March 17, 2020, and February 1, 2022, with traceable ECMO data. The items on clinical epidemiological characteristics and various medical outcomes were collected. Statistical analysis included a median and interquartile range (IQR) for continuous variables and frequencies for categorical variables. Results The number of participating hospitals was 731, and the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
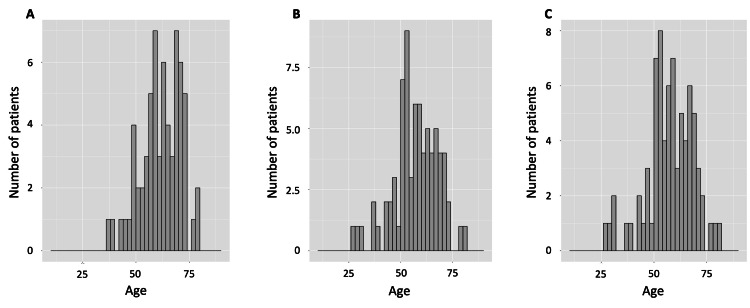 Figure 1
Figure 1| Parameters | Subcategories | Overall (n=49590) | ECMO (n=196) | Non-ECMO (n=49394) |
| Background | ||||
| Age (years) | 58.0 (42.0, 74.0) | 59.5 (51.0, 68.0) | 58.0 (42.0, 74.0) | |
| Sex | Male | 28664 (57.8) | 160 (81.6) | 28504 (57.7) |
| Female | 20909 (42.2) | 36 (18.4) | 20873 (42.3) | |
| Other | 13 (0.0) a | 0 | 13 (0.0) a | |
| Smoking history | Currently smoking | 7936 (16.0) | 26 (13.3) | 7910 (16.0) |
| Smoking in the past | 10689 (21.6) | 66 (33.7) | 10623 (21.5) | |
| Never | 22799 (46.0) | 65 (33.2) | 22734 (46.0) | |
| Unknown | 8068 (16.3) | 39 (19.9) | 8029 (16.3) | |
| Drinking alcohol | Daily | 3146 (6.3) | 11 (5.6) | 3135 (6.3) |
| Occasional | 16247 (32.8) | 63 (32.1) | 16184 (32.8) | |
| None | 17496 (35.3) | 45 (23.0) | 17451 (35.3) | |
| Unknown | 12059 (24.3) | 70 (35.7) | 11989 (24.3) | |
| BMI (kg/m2) | 24.0 (21.0, 26.7) | 27.7 (24.5, 31.1) | 23.6 (21.0, 26.7) | |
| Conditions at admission | ||||
| Days from symptom onset to hospitalization | 4.0 (2.0, 7.0) | 7.0 (4.0, 10.0) | 4.0 (2.0, 7.0) | |
| Body temperature (℃) | 37.0 (36.6, 37.8) | 37.5 (36.8, 38.3) | 37.0 (36.6, 37.8) | |
| Heart rate (beats/minute) | 86.0 (76.0, 97.0) | 94.0 (79.8, 107.3) | 86.0 (76.0, 97.0) | |
| Respiratory rate (breaths/minute) | 18.0 (16.0, 21.0) | 22.0 (18.0, 28.0) | 18.0 (16.0, 21.0) | |
| Systolic blood pressure (mmHg) | 128.0 (115.0, 142.0) | 130.0 (112.0, 147.8) | 128.0 (115.0, 142.0) | |
| Diastolic blood pressure (mmHg) | 79.0 (70.0, 89.0) | 78.0 (68.0, 90.0) | 79.0 (70.0, 89.0) | |
| State of consciousness (AVPU scale) | A (alert) | 45742 (92.2) | 138 (70.4) | 45604 (92.3) |
| V (verbal) | 1376 (2.8) | 17 (8.7) | 1359 (2.8) | |
| P (pain) | 261 (0.5) | 6 (3.1) | 255 (0.5) | |
| U (unresponsive) | 145 (0.3) | 8 (4.1) | 137 (0.3) | |
| SpO2 under room air (%) | 97.0 (95.0, 98.0) | 94.0 (90.0, 96.0) | 97.0 (95.0, 98.0) | |
| Route of noninvasive O2 administration | Nasal cannula | 5429 (10.9) | 17 (8.7) | 5412 (11.0) |
| Face mask | 1526 (3.1) | 30 (15.3) | 1496 (3.0) | |
| Reservoir mask | 1074 (2.2) | 28 (14.3) | 1046 (2.1) | |
| High-flow oxygen device | 210 (0.4) | 6 (3.1) | 204 (0.4) | |
| Finding by X-ray | No abnormality | 14494 (29.2) | 8 (4.1) | 14486 (29.3) |
| Pneumonia | 20008 (40.3) | 164 (83.7) | 19844 (40.2) | |
| Abnormality (excluding pneumonia) | 558 (1.1) | 1 (0.5) | 557 (1.1) | |
| Finding by CT | No abnormality | 7591 (15.3) | 4 (2.0) | 7587 (15.4) |
| Pneumonia | 28031 (56.5) | 157 (80.1) | 27874 (56.4) | |
| Abnormality (excluding pneumonia) | 886 (1.8) | 4 (2.0) | 882 (1.8) | |
| Comorbidities | ||||
| Myocardial infarction | 946 (1.9) | 6 (3.1) | 940 (1.9) | |
| Congestive heart failure | 1567 (3.2) | 4 (2.0) | 1563 (3.2) | |
| Cerebrovascular disease | 3231 (6.5) | 9 (4.6) | 3222 (6.5) | |
| Paralysis | 725 (1.5) | 0 | 725 (1.5) | |
| COPD | 1214 (2.4) | 9 (4.6) | 1205 (2.4) | |
| Chronic lung disease other than COPD | 711 (1.4) | 6 (3.1) | 705 (1.4) | |
| Bronchial asthma | 2652 (5.3) | 15 (7.7) | 2637 (5.3) | |
| Moderate to severe liver dysfunction | 169 (0.3) | 1 (0.5) | 168 (0.3) | |
| Hypertension | 15336 (30.9) | 82 (41.8) | 15254 (30.9) | |
| Dyslipidemia | 7312 (14.7) | 43 (21.9) | 7269 (14.7) | |
| Diabetes with complications | 1108 (2.2) | 8 (4.1) | 1100 (2.2) | |
| Obesity | 3501 (7.1) | 37 (18.9) | 3464 (7.0) | |
| Moderate to severe renal dysfunction | 833 (1.7) | 4 (2.0) | 829 (1.7) | |
| Hemodialysis before admission | 495 (1.0) | 2 (1.0) | 493 (1.0) | |
| Immunosuppressionb | 1050 (2.1) | 4 (2.0) | 1046 (2.1) | |
| Parameters | Subcategories | Overall (n=49590) | ECMO (n=196) | Non-ECMO (n=49394) |
| Treatments during hospitalization | ||||
| Noninvasive mechanical ventilationa | 599 (1.2) | 32 (16.3) | 567 (1.1) | |
| Mechanical ventilation | 2439 (4.9) | 192 (98.0) | 2247 (4.5) | |
| Mechanical ventilation duration days | 8.0 (4.0, 14.0) | 16.0 (11.0, 28.0) | 7.0 (4.0, 13.0) | |
| Days to ECMO initiation from admission | 4.0 (1.0, 8.0) | 4.0 (1.0, 8.0) | NA | |
| Length of ICU stay (days) | 7.0 (3.0, 14.0) | 21.0 (14.0, 35.0) | 7.0 (3.0, 13.0) | |
| ECMO duration days | 11.0 (8.0, 20.0) | 11.00 (8.0, 20.0) | NA | |
| Prone positioning | 2302 (4.6) | 105 (53.6) | 2197 (4.4) | |
| Nitric oxide inhalation | 37 (0.1) | 9 (4.6) | 28 (0.1) | |
| Tracheostomy | 426 (0.9) | 69 (35.2) | 357 (0.7) | |
| Neuromuscular blocking agent | 1415 (2.9) | 140 (71.4) | 1275 (2.6) | |
| Vasopressor support | 1339 (2.7) | 141 (71.9) | 1198 (2.4) | |
| RRT or dialysis | 706 (1.4) | 66 (33.7) | 640 (1.3) | |
| Blood transfusion | 979 (2.0) | 158 (80.6) | 821 (1.7) | |
| Complications | ||||
| ARDS | 2323 (4.7) | 117 (59.7) | 2206 (4.5) | |
| Severity of ARDS | Mild | 499 (1.0) | 3 (1.5) | 496 (1.0) |
| Moderate | 789 (1.6) | 21 (10.7) | 768 (1.6) | |
| Severe | 969 (2.0) | 89 (45.4) | 880 (1.8) | |
| Myocardial ischemia | 87 (0.2) | 5 (2.6) | 82 (0.2) | |
| Bacteremia | 474 (1.0) | 53 (27.0) | 421 (0.9) | |
| Gastrointestinal bleeding | 290 (0.6) | 20 (10.2) | 270 (0.5) | |
| Patient status at discharge | ||||
| Oxygen therapy requiredb | 3231 (6.5) | 34 (17.3) | 3197 (6.5) | |
| RRT or dialysisb | 377 (0.8) | 3 (1.5) | 374 (0.8) | |
| Tracheostomyb | 362 (0.7) | 18 (9.2) | 344 (0.7) | |
| Parameters | Subcategories | Overall (n=49590) | ECMO (n=196) | Non-ECMO (n=49394) |
| Patient outcomes at hospital discharge | ||||
| Hospital mortality, %(n) | 4.9 (2437) | 33.2 (65) | 4.8 (2372) | |
| Discharge to home | 36598 (73.8) | 45 (23.0) | 36553 (74.0) | |
| Discharge to long-term care center | 1962 (4.0) | 1 (0.5) | 1961 (4.0) | |
| Discharge to acute care hospital | 5798 (11.7) | 57 (29.1) | 5741 (11.6) | |
| Discharge to an isolation hospital | 2132 (4.3) | 0 | 2132 (4.3) | |
| Still in the hospitala | 11 (0.0)b | 1 (0.5) | 10 (0.0)b | |
| Complications | ||||
| Pneumothorax | 201 (0.4) | 19 (9.7) | 182 (0.4) | |
| Seizures | 111 (0.2) | 8 (4.1) | 103 (0.2) | |
| Stroke | 175 (0.4) | 9 (4.6) | 166 (0.3) | |
| Pulmonary thromboembolism | 170 (0.3) | 4 (2.0) | 166 (0.3) | |
| Patient condition at discharge | ||||
| Self-care abilityc | Same as before hospitalization | 40098 (80.9) | 22 (11.2) | 40076 (81.1) |
| Worsened or required assistance | 4393 (8.9) | 75 (38.3) | 4318 (8.7) | |
| Improved | 990 (2.0) | 1 (0.5) | 989 (2.0) | |
| Unknown | 3099 (6.2) | 75 (38.2) | 3024 (6.1) | |
| Ambulatory functionc | Same as before hospitalization | 39428 (79.5) | 18 (9.2) | 39410 (79.8) |
| Worsened or required assistance | 4507 (9.1) | 76 (38.8) | 4431 (9.0) | |
| Improved | 795 (1.6) | 1 (0.5) | 794 (1.6) | |
| Unknown | 901 (1.8) | 6 (3.1) | 895 (1.8) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMechanical Circulatory Support Devices · Respiratory Support and Mechanisms · Long-Term Effects of COVID-19
Introduction
Since 2019, the outbreak of coronavirus disease 2019 (COVID-19) has escalated into a global pandemic, presenting unprecedented challenges to healthcare systems worldwide. Among the myriad of complications associated with COVID-19, severe respiratory failure stands out, often requiring intensive care [1], like extracorporeal membrane oxygenation (ECMO), which has been a critical tool in managing severe respiratory failure worldwide, with its efficacy well-established [2].
Extracorporeal membrane oxygenation has also been used for severe respiratory failure in COVID-19 cases worldwide. However, a notable variability in outcomes has been observed, influenced by regional and institutional differences [3-4]. This variability can be attributed to factors such as the rapid and extensive spread of the virus, the evolving efficacy of treatments for severe respiratory failure [5], and the diverse results observed by different countries. Various circumstances emerged worldwide, with some nations successfully implementing measures while others faced challenges. Furthermore, the COVID-19 virus underwent mutations with varying characteristics in various locales [6], highlighting the necessity for region-specific medical systems.
In Japan, the pandemic has led to a significant reliance on ECMOs for managing severe respiratory failure [7]. However, the reported outcomes for COVID-19 patients nationwide in Japan have been limited to survival rates [8], a metric that, while important, does not fully encapsulate the multifaceted nature of effective medical treatment. In contrast, other countries have provided more comprehensive reports, encompassing a range of clinical and epidemiological outcomes [3,9]. Such detailed reporting is invaluable, contributing significantly to the global understanding of respiratory infectious diseases and their management.
In light of this, our study seeks to fill the existing gap in knowledge by providing an in-depth analysis of the clinical epidemiological characteristics and diverse medical outcomes of COVID-19 patients treated with ECMO in Japan. This approach not only aligns with the global need for comprehensive data on COVID-19 management but also contributes uniquely to the body of knowledge on the effectiveness of ECMO in varied clinical settings.
Materials and methods
Study design and data source
This study was a retrospective cross-sectional study using the COVID-19 Registry Japan (COVIREGI-JP), an extensive registry database of patients at various sites during the COVID-19 pandemic. The study data were collected and managed using REDCap (Research Electronic Data Capture), a secure, web-based data capture application hosted at the Joint Center for Researchers, Associates, and Clinicians (JCRAC) data center of the National Center for Global Health and Medicine. All patients registered in COVIREGI-JP were diagnosed with COVID-19. Extensive data were collected on their life background before admission, vaccination status for COVID-19, drugs used during hospitalization, and treatment during hospitalization. This study was conducted with the approval of the ethics committee of Hokkaido University Hospital, Sapporo, Japan (approval number: 021-0211) and COVIREGI-JP (approval number: 1248600101). The study conducted has been reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement [10].
Patient selection
Data from patients over 18 years enrolled between March 17, 2020, when COVIREGI-JP was opened, and February 1, 2022, were included. Patients with missing data on ECMO implementation during hospitalization were excluded from the analysis. Only those subjects for whom responses regarding ECMO implementation during hospitalization were available were classified into the ECMO group. For ECMO implementation responses, COVIREGI-JP does not distinguish between venovenous (V-V) ECMO and venoarterial (V-A) ECMO. Therefore, all patients who used ECMO, whether V-V or V-A, were included in response to ECMO implementation.
Collected items
As for the clinical epidemiological characteristics, patient background information like their age, sex, smoking history, drinking alcohol, and body mass index (BMI) was collected. In addition, as conditions at admission, the following items were collected: days from symptom onset to hospitalization, body temperature, heart rate, respiratory rate, systolic blood pressure, diastolic blood pressure, state of consciousness (alert, verbal, pain, and unresponsive (AVPU) scale), oxygen saturation (SpO_2_) under room air, route of oxygen administration (canula, mask, reservoir mask, high flow oxygen device), chest X-ray at admission (performed within ±3 days of admission), CT at admission (performed within ±3 days of admission). Furthermore, significant comorbidities at the time of hospitalization and other items related to major treatments performed during hospitalization were collected.
The medical outcomes in this study were defined as the patient outcomes at hospital discharge, the incidence of complications during hospitalization (pneumothorax, seizure, intracerebral bleeding/ischemic stroke, pulmonary thromboembolism), the patient's condition during hospital discharge regarding self-care ability, and ambulatory function. The complications of stroke included both cerebral hemorrhage and cerebral infarction.
Statistical analysis
Continuous variables were described as the median and interquartile range (IQR), and categorical variables were calculated for their frequencies. The number of deaths and the count of patients who worsened or required assistance with self-care ability and those who worsened or required assistance with ambulatory function in the ECMO group are shown against age. The percentage of missing values was calculated for each item when the items had missing values. All statistical analyses were conducted using R version 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
During the study period, 51,441 patients were enrolled, and 731 hospitals participated. Of these, 49,590 patients were included in the analysis as participants, after excluding those with missing responses regarding ECMO implementation during hospitalization. Among the participants, 196 patients (0.4%) were in the ECMO group.
Characteristics of patients
Participant characteristics are listed in Table 1. The median age of all patients was 58 years (IQR, 42-74 years), with the ECMO group being 59.5 years (51-58 years) and the non-ECMO group being 58 years (IQR, 42-74 years). Of all the patients, 28,664 (57.7%) were male, with 160 patients (81.6%) in the ECMO group and 28,504 patients (57.7%) in the non-ECMO group being male. The median BMI of all patients was 23.6 kg/m^2^ (IQR, 21-26.7 kg/m^2^), with the ECMO group having a median BMI of 27.7 kg/m^2^ (IQR, 24.5-31.1 kg/m^2^) and the non-ECMO group having a median BMI of 23.6 kg/m^2^ (IQR, 21-26.7 kg/m2).
Table 1: Characteristics of the patientsValues are presented as median (interquartile range) or n(%).BMI: body mass index; SpO2: oxygen saturation; CT: computed tomography; COPD: chronic obstructive pulmonary disease; ECMO: extracorporeal membrane oxygenation.aPercentage showed less than 0.1%.bImmunosuppression includes neutropenia (<500 neutrophils/μL), glucocorticoid/steroid use within one month (doses greater or equal to an equivalent of 20 mg of prednisone per day for at least one month), chemotherapy, radiation therapy, or immunosuppressant use (such as anti-tumor necrosis factor α therapy, anti-interleukin-6 receptor/anti-CD20 monoclonal antibodies, selective T-cell co-simulation blocker, methotrexate, tacrolimus) in the past three months, post-transplantation, asplenia, and primary immunodeficiency syndrome).
Treatments performed during hospitalization
During hospitalization, 599 (1.2%) patients received noninvasive mechanical ventilation. Among them, 32 (16.3%) belonged to the ECMO group, while 567 (1.1%) belonged to the non-ECMO group. In terms of invasive mechanical ventilation, 2,439 (4.9%) overall patients received it, with 192 (98.0%) in the ECMO group and 2,247 (4.5%) in the non-ECMO group. The median length of ICU stay was seven days (IQR, 3-14 days) for overall patients, 21 days (IQR, 14-35 days) for the ECMO group, and seven days (IQR, 3-13 days) for the non-ECMO group. The median duration of ECMO treatment was 11 days (IQR, 8-20 days). Table 2 provides further details.
Medical outcomes
The results of the medical outcomes are shown in Table 3. This study found that hospital mortality was higher in the ECMO group (33.2%) compared to the non-ECMO group (4.8%). Regarding other patient outcomes, more patients in the ECMO group (23.0%) were discharged to acute care hospitals compared to the non-ECMO group (11.6%). A lower percentage of patients in the ECMO group (0.5%) were discharged to long-term care centers than the non-ECMO group (4.0%). The majority of patients (73.8%) were discharged home. The complications during hospitalization were pneumothorax (9.7%), seizures (4.1%), stroke (4.6%), and pulmonary thromboembolism (2.0%) in the ECMO group. In addition, at the time of discharge, a higher percentage of patients in the ECMO group (38.3%) had worsened or required assistance with self-care ability compared to the non-ECMO group (8.7%). Similarly, a higher percentage of patients in the ECMO group (38.8%) had worsened or required assistance with ambulatory function compared to the non-ECMO group (9.0%). This study also provided information on the age distribution of patients in the ECMO group who died, which increased beginning in the late 50s, and patients with worsened or required assistance with self-care ability and ambulatory function increased from the early 50s (Figure 1). The number of missing data points for all variables has been provided in Appendices A-C.
The distribution of patients by outcomes in the ECMO groupA: The distribution of hospital mortality in the ECMO group indicates that the number of patients who died increased in the late 1950s. B: The distribution of worsened or required assistance with self-care ability in the ECMO group showed patients increased from the early 50s. C: The distribution of worsened or required assistance with ambulatory function in the ECMO group showing patients increased from the early 50s.ECMO: extracorporeal membrane oxygenation
Discussion
Our study utilized the COVIREGI-JP database to conduct a descriptive analysis of COVID-19 patients in Japan treated with ECMO. We identified the mortality rate and the range of complications associated with ECMO treatment. Notably, our findings show a mortality rate of about 33% in Japan, consistent with national data [8] and slightly more favorable outcomes compared to international meta-analyses [3-4].
A significant aspect of our study was examining the age demographics of patients treated with ECMO in Japan. We observed that the third quartile of age was higher compared to other countries [9, 11] but younger than the overall group. This suggests a more selective approach to ECMO use in non-elderly patients within Japan, potentially contributing to the slightly better mortality outcomes observed. Our findings align with existing research indicating that age is a significant factor in ECMO outcomes, with increased mortality risks associated with ECMO in patients over the age of 59 [8-9]. This selective approach may reflect a balance between the risks and benefits of ECMO treatment in an aging population, highlighting the importance of considering patient age in ECMO treatment decisions.
The incidence of complications in the ECMO group is managed at the same level worldwide. In general, significant complications related to ECMO treatment are reported to be related to hemorrhage [12], just as in COVID-19 patients [13-14]. For intracerebral hemorrhage, many studies have reported incidence rates ranging from 2.3% to 17.4% [9,11,15-21], with some reporting incidence rates as high as 41.7% [22]. In addition, ischemic stroke has been reported to have an incidence of 0.7% to 7% [9,11,15-16,18-21]. These results suggest that the incidence of intracerebral hemorrhage and ischemic stroke for patients managed with ECMO in Japan is comparable to other countries. Regarding the incident rate of seizures, the previous study reported 0% to 2% [9,18,20] and a rise to 14% restricted to non-survivors [18]. Our study included both non-survivors and survivors, which may have resulted in a higher percentage. In the development of pneumothorax, previous studies reported the incidence rate was 11% and 12.6% [15,23], and the present results were similar to slightly lower rates. For pulmonary thromboembolism, various studies have reported incidence rates ranging from 1.6% to 19% [11,15-18,23-24], with some reporting rates of over 60% [25-26]. In light of these circumstances, the incidence of pulmonary thromboembolism in Japan is confirmed to be relatively low. A unique ECMO support system was established in Japan to assist almost all ICUs treating COVID-19 patients who require ECMO [27]. Furthermore, the Japan ECMOnet for COVID-19, a collaboration of several major Japanese societies specializing in ECMO, has introduced Japan’s basic ECMO management concept [28]. The results of this study may reflect the variety of Japan’s responses to the COVID-19 pandemic.
Finally, this study indicates the significant impact on post-discharge life, particularly for patients in their post-middle-age years, underscoring the need for greater attention to these effects. Compared to those hospitalized in general wards, there was a decline in activities of daily living (ADL) after hospital discharge in older adult patients with COVID-19 who were admitted to the ICU [29]. Additionally, a reduction in ambulatory function at discharge was linked to an ongoing functional decline post-discharge [30]. The implications of these results may not be limited to Japan, as the rate of home discharge for patients who used ECMO in Japan was similar to that in other countries [9].
However, our study has limitations. The COVIREGI-JP lacks specific ICU data, including detailed invasive mechanical ventilator management and ECMO types like V-V ECMO or V-A ECMO, which restricts our ability to provide a comprehensive analysis of ICU treatments and outcomes.
Research implication
Most registry databases aim to collect data during hospitalization, and medical records do not include post-discharge data. We need the database collecting post-discharge data or other study methodologies to understand the daily lives of patients post discharge. In addition, post-discharge studies on COVID-19 patients who used ECMO are limited, and the cohort is small. Therefore, we may need a prospective study targeting a large cohort or large number to explore the effect and provide more evidence of the post-discharge life of COVID-19 patients on whom ECMO was used.
Conclusions
In this study, we revealed the clinical epidemiological characteristics of COVID-19 patients treated with ECMO. The results of this study suggest that Japanese hospitals managed COVID-19 patients with a more selective approach to ECMO use in cases of non-elderly patients. The medical outcomes related to ECMO-treated COVID-19 patients, such as hospital mortality and incidence of complications, were as good as or somewhat better than their counterparts in other countries. Furthermore, the results of this study indicate a potential impact on post-discharge life, particularly in post-middle-age patients. Future research should focus on the post-discharge life of ECMO patients to provide more evidence, as a wide range of ages may be affected by post-discharge life.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study Lancet Chen N Zhou M Dong X 50751339520203200714310.1016/S 0140-6736(20)30211-7PMC 7135076 · doi ↗ · pubmed ↗
- 2ECMO for severe ARDS: systematic review and individual patient data meta-analysis Intensive Care Med Combes A Peek GJ Hajage D 204820574620203302168410.1007/s 00134-020-06248-3PMC 7537368 · doi ↗ · pubmed ↗
- 3Extracorporeal membrane oxygenation for COVID-19: a systematic review and meta-analysis Crit Care Ramanathan K Shekar K Ling RR 2112520213412702710.1186/s 13054-021-03634-1PMC 8201440 · doi ↗ · pubmed ↗
- 4ECMO in COVID-19 patients: a systematic review and meta-analysis J Cardiothorac Vasc Anesth Bertini P Guarracino F Falcone M Nardelli P Landoni G Nocci M Paternoster G 270027063620223490638310.1053/j.jvca.2021.11.006PMC 8585556 · doi ↗ · pubmed ↗
- 5Chemoprophylaxis, diagnosis, treatments, and discharge management of COVID-19: an evidence-based clinical practice guideline (updated version)Mil Med Res Jin YH Zhan QY Peng ZY 41720203288767010.1186/s 40779-020-00270-8PMC 7472403 · doi ↗ · pubmed ↗
- 6A comprehensive review of COVID-19 virology, Vaccines, variants, and therapeutics Curr Med Sci Forchette L Sebastian W Liu T 103710514120213424177610.1007/s 11596-021-2395-1PMC 8267225 · doi ↗ · pubmed ↗
- 7Clinical epidemiology of hospitalized patients with coronavirus disease 2019 (COVID-19) in Japan: report of the COVID-19 Registry Japan Clin Infect Dis Matsunaga N Hayakawa K Terada M 08973202110.1093/cid/ciaa 1470 PMC 754331132986793 · doi ↗ · pubmed ↗
- 8Trends in survival during the pandemic in patients with critical COVID-19 receiving mechanical ventilation with or without ECMO: analysis of the Japanese national registry data Crit Care Ohshimo S Liu K Ogura T 3542620223638037710.1186/s 13054-022-04187-7PMC 9664428 · doi ↗ · pubmed ↗