Plasma 25-hydroxyvitamin D deficiency in the peri-operative period is associated with survival outcome in colorectal cancer patients: a meta-analysis
Baojia Zheng, Jianchang Chen, Xiaohua Gong

TL;DR
Low vitamin D levels before and after surgery are linked to worse survival in colorectal cancer patients, with post-surgery levels being most critical.
Contribution
This study is the first to meta-analyze the impact of peri-operative 25(OH)D deficiency on colorectal cancer survival outcomes.
Findings
Peri-operative 25(OH)D deficiency was found in 59.61% of patients.
Post-operative 25(OH)D deficiency was more strongly linked to short-term survival than pre-operative deficiency.
Male gender, rectum tumors, and seasonal sampling were identified as risk factors for 25(OH)D deficiency.
Abstract
Surgery had a significant impact on 25-hydroxyvitamin D (25-(OH)D) levels. Uncertainty still existed regarding the effects of peri-operative 25(OH)D deficiency on colorectal cancer (CRC) patients’ prognosis. The purpose of the present study was to explore the potential association between the peri-operative 25(OH)D deficiency and the survival outcome of CRC. Seven electronic databases [including PubMed, EMBASE, Web of Science, The Cochrane Library, OvidMEDLINE(R), China National Knowledge Infrastructure (CNKI) and Wangfang data] were searched without language limitations. The primary outcomes were overall survival and all-cause mortality. Secondary outcomes were the incidence of 25(OH)D deficiency and risk variables for low 25(OH)D level in the peri-operative period. 14 eligible studies were obtained with 9324 patients for meta-analysis. In the peri-operative period, the pooled…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
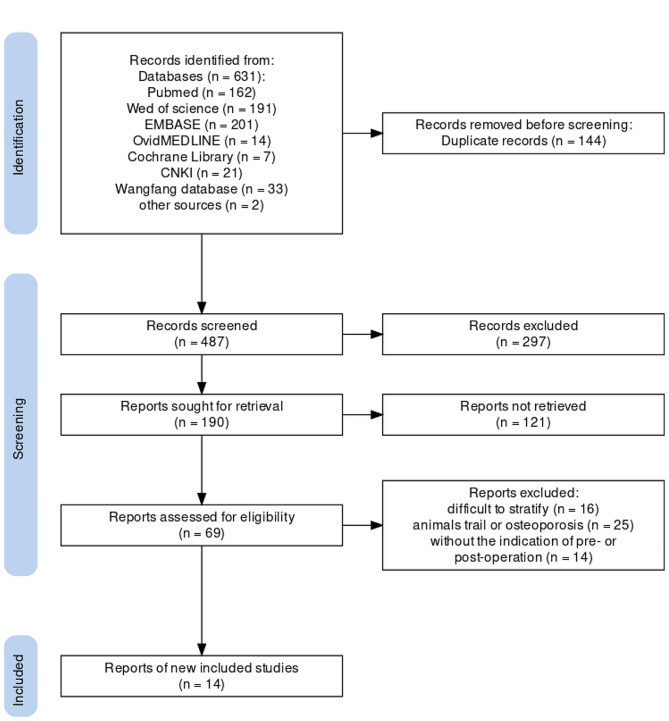 Figure 1
Figure 1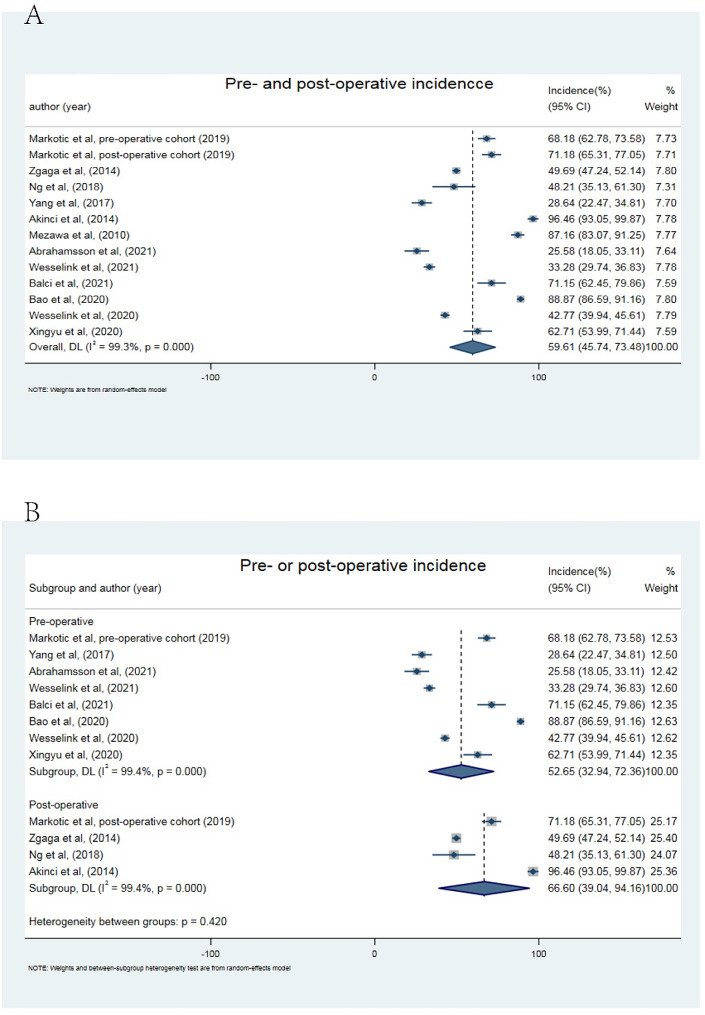 Figure 2
Figure 2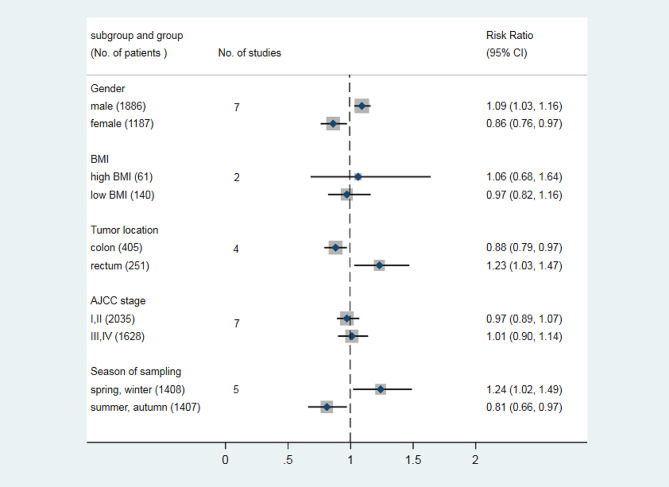 Figure 3
Figure 3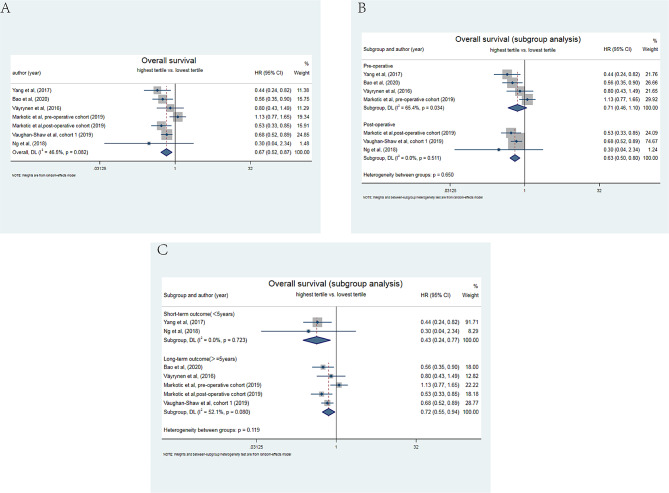 Figure 4
Figure 4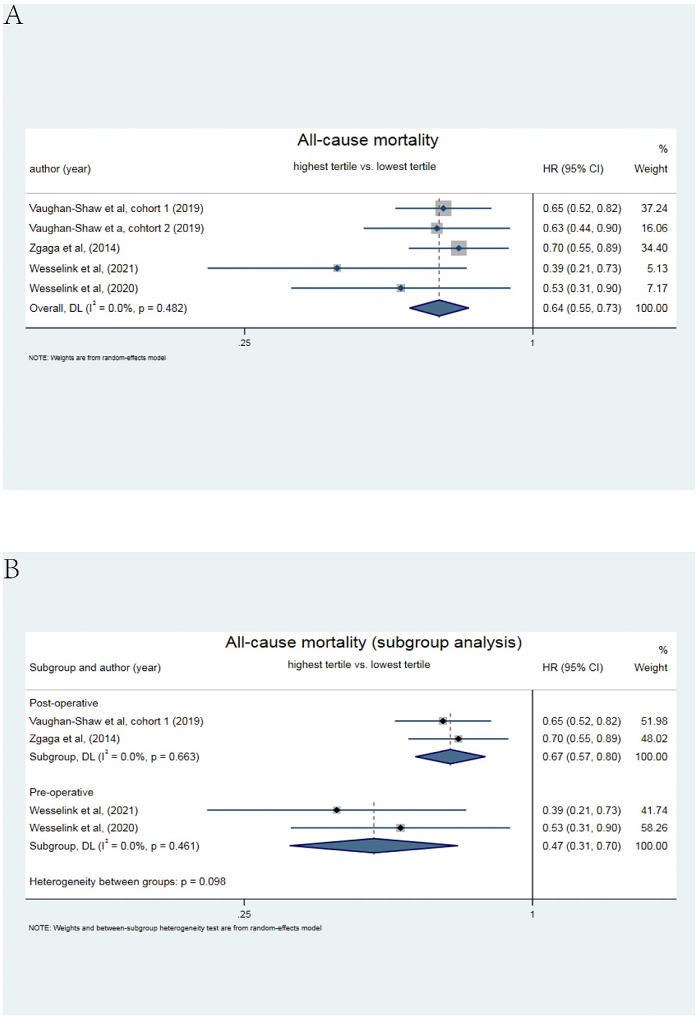 Figure 5
Figure 5- —Science and Technology Projects of Social Development in Zhuhai
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVitamin D Research Studies · Colorectal Cancer Surgical Treatments · Pituitary Gland Disorders and Treatments
Introduction
Colorectal cancer (CRC) was currently the fourth most common cancer worldwide, and its incidence was still on the rise [1]. In the United States, CRC was the second most common cause of cancer death [2]. The mainstay of treatment for colorectal cancer was still surgery [3]. Despite advances in treatment over the past three decades, the mortality rate of CRC remained high mostly due to recurrence and distant organ metastases [4]. It was widely reported that tumor characteristics were not the only factor influencing prognosis, while host-related factors in the peri-operative period were greatly contributing to the poor survival outcomes in patients with CRC [5]. Up to now, it had been discovered that peri-operative status of some host factors, such as anima [6], sarcopenia [7] and immune status [8] played substantial roles in tumor growth, which were closely associated with prognosis. Thus, exploring other possible peri-operative host-factors associated to prognosis and taking early intervention possibly benefited the prognosis and survival of CRC.
Vitamin D was a steroid hormone known to affect calcium homeostasis and skeletal physiology [9]. Due to the strong homeostatic regulation of the formation and levels of 1,25(OH)2D and the short half-life, studies frequently used circulating 25-hydroxyvitamin D (25(OH)D) to determine vitamin D status [10]. Vitamin D status in human disorders had drawn increasing attention, which was recognized as a kind of crucial hormone for preserving the regular operation of many organs or bodily systems [11]. A recent meta-analysis confirmed that higher vitamin D intake and serum 25(OH)D levels were associated with lower cancer risk and cancer-related mortality [12]. Numerous research and meta-analyses had revealed that adequate vitamin D consumption reduced the onset of CRC [13, 14]. Besides, vitamin D might act as a predictive factor for the survival outcome in CRC [15, 16]. The level of 25(OH)D concentration significantly fluctuated during surgery [17]. However, peri-operative vitamin D levels still had ambiguous findings on prognosis in patients with CRC [18, 19].
Therefore, the meta-analysis was conducted to further identify the impact of the peri-operative vitamin D levels on short-term and long-term survival outcome in CRC. Simultaneously, the incidence and risk factors of peri-operative 25(OH)D deficiency were further evaluated to assist in the clinical identification of evidence for intervention.
Materials and methods
Search strategy
The present review adhered to Preferred Reporting Items For Systematic Reviews and Meta-Analyses(PRISMA) statement [20]. In the last week of April 2023, a search was conducted in seven electronic databases, including PubMed, EMBASE, Web of Science, The Cochrane Library, OvidMEDLINE(R), China National Knowledge Infrastructure (CNKI) and Wangfang data, without language limitations. The following search terms (MeSH) were used in “All fields” to identify relevant published articles:
- “CRC” OR “colorectal cancer” OR “colorectal tumor” OR “colorectal neoplasms” OR “colon cancer” OR “rectal cancer” OR “rectal neoplasm” OR “colonic neoplasm” OR “colon” OR “rectum”.
- “25(OH)D” OR “25-hydroxyvitamin D” OR “vitamin D”.
- “surgery” OR “operation”.
- “prognosis” OR “mortality” OR “survival” OR “outcomes”.
- 1 AND 2 AND 3 AND 4.
Study selection
The published studies were retrieved with no restrictions of language. The included studies were required to meet the following eligible criteria: (a)prospective or retroprospective cohort studies; (b) measurement of circulating 25-OHD in patients with colorectal cancer; (c) description of the outcome in colorectal cancer; and (d) reporting HRs and corresponding 95%CIs according to different categories of blood 25(OH)D levels to conduct a meta-analysis. Reports published as review articles, protocol, editorials, guidance and consensus were excluded. All titles were independently screened by two authors in accordance with the search strategy mentioned above (B.Z and J.H). A total of 631 records were acquired from the 7 electronic databases. After removing duplicate records, two authors independently performed an abstract review of potentially relevant records to assess their eligibility based on the inclusion criteria. Differences were resolved through discussion until a consensus was reached. Then, a full text search of the remaining 69 records was conducted, and 55 records were eliminated due to animals trail, or without the indication of the pre- or post-operation, or difficulty in stratifying (Fig. 1). The Newcastle Ottawa Quality scale (NOS) for assessing the quality in meta-analyses was used to evaluated the quality of the included studies [21]. For NOS, a score of at least 6 out of 9 indicated high quality.
Fig. 1. Flow diagram for study selection
Data extraction
The data from eligible studies were extracted including the following information: first author’s name, publication year, country, study design, time for blood drawing, sample size, gender ratio(male/female), median age, follow-up duration, CRC stage, death, cut-off value of 25(OH)D deficiency, tertiles for outcome analysis, HR and 95%CI for overall survival and all-cause mortality in the studies.
Statistical analysis
The primary outcomes were the impact of the levels of peri-operative 25(OH)D on overall survival and all-cause mortality. Secondary outcomes were the incidence and risk factors of 25(OH)D deficiency in the peri-operative period. Pooled proportions were calculated for incidence of 25(OH)D deficiency by conducting single-arm meta-analysis, meanwhile subgroup meta-analyses were individually performed for all variables based on pre-operative point and post-operative point, short-term and long-term survival outcome. The binomial distribution was utilized to calculate risk ratio (RR) and 95% confidence interval (CI) for risk factors. The extracted HRs and 95% CIs were used to calculate the pooled HR estimates. A random-effects model was used for all meta-analysis because the significant heterogeneity was assumed among the included studies [22]. A forest plot was used to illustrate the distribution of the outcome and effect size obtained from each included study. Egger’s test was used to detect the potential publication bias. All statistical analyses were conducted using STATA 16.0 (STATA Corp, College Station, TX).
Results
Characteristics of the included studies
The flow diagram of the search and study selection process was shown in Fig. 1. Characteristics of the included studies [17, 18, 23–34] were summarized in Table 1. A total of 14 eligible studies with 9324 patients (male: 5541, female: 3783) were included. The numbers of patients in the included studies ranged from 56 to 1848 cases. The overall average age (± standard error [SE]) of the all patients was 64.09 ± 2.11 years. These studies were published between 2014 and 2021, of which twelve were prospective studies and two were retrospective studies. Of these studies, five were from Asia (three from China, one from Japan and one from Singapore) and nine were from outside Asia (two from the UK, two from Turkey, two from Netherlands, one from Finland, one from Ireland, and one from Norway). The cut-off values of 25(OD)D deficiency and the tertiles for outcome analysis in different studies were shown for pooled extraction. Overall survival and all-cause mortality [high level vs. low level of 25(OH)D] in the included studies were also revealed in Table 1. In addition, NOS scores represented the quality of all included studies based on the NOS checklist, of which 11 studies were at least 6, indicating high quality of adherence for most studies.
Table 1. Characteristics of the included studiesAuthor(year, country)Study designTime for blood drawing (median time)No. of patientsGender ratio(male/female)Median ageFollow-up(months)CRC stageDeathCut-off values of 25(OH)D deficiencyTertiles for outcome analysisOverall survial HR(95%CI)All-cause mortalityHR(95%CI)NOS scoresMarkotic et al., (2019,Ireland) [23]prospectivepre-operative cohort:1 day before surgery;post-operative cohort:8 days after surgery (median time)pre-operative cohort:286;post-operative cohort:229pre-operative cohort:184/102;post-operative cohort:137/92pre-operative cohort:65.9 ± 11.6;post-operative cohort:65.7 ± 11.770.8I-IIIpre-operative cohort:118;post-operative cohort:113≤ 50nmol/l≤ 50nmol/l, >50nmol/lpre-operative cohort:1.13(0.77–1.65);post-operative cohort:0.53(0.33–0.84)/7Wesselink et al.,(2021,Netherlands) [24]prospectiveat diagnosis679440/2396742I-III68< 50nmol/L< 50 nmol/L; ≥ 50 nmol/L/0.39(0.21–0.73)7Väyrynen et al.,(2016,Finland) [17]prospectivepre-operative11758/59/60I-IV//≤ 50nmol/l, >50nmol/l0.80 (0.43–1.49)/7Ng et al.,(2018,Singapore) [18]prospective17 days after surgery5634/226222II- III/< 20ng/ml<21ng/ml, 21-30ng/ml, >30ng/ml0.30(0.04–2.44)/5Vaughan-Shaw et al., (2019,UK) [25]prospectivecohort 1:postoperative;cohort 2:peri -operativecohort 1 :1687;cohort 2 :1848cohort 1 :970/717;cohort 2 :1024/824/cohort 1 :159.6;cohort 2 :43.2I-IIIcohort 1 :709;cohort 2 :211/cohort 1 : >18.1,18.1–33.1, >33.1nmol/l;;cohort 2 : <38.0,38.0-57.9, >57.9nmol/Lcohort 1:0.68(0.50–0.85)cohort 1 :0.65(0.51–0.81);cohort 2 :0.63(0.44–0.89)8Zgaga et al.,(2014,UK) [26]prospective105 days after surgery1598916/682/106.8I-III531<10ng/ml<7.25ng/ml, 7.25—13.25ng/ml, >13.25ng/ml/0.70(0.55–0.89)9Yang et al.,(2017,China) [27]prospectivewithin seven days before operation206131/756345I-III87<6.2ng/ml<6.2ng/ml, 6.2-29.9ng/ml, >29.9ng/ml0.442(0.238–0.819)/6Akinci et al.,(2014, Turkey) [28]retrospectivepost-operative: at the remission period11379/34/48I-IV/< 30ng/ml///5Mezawa et al.,(2010, Tokyo) [29]prospectivethe peri-operative period257165/926532.4I-IV39< 30ng/ml3-7ng/mL;8–10 ng/mL; 11–15 ng/mL; 16–36 ng/mL0.91(084-0.99)/7Abrahamsson et al.,(2021,Norway) [30]prospective2–3 days prior to histological confirmation12983/466539I-IV35< 50nmol/L///6Balci et al.,(2021, Turkey) [31]prospectivein a week to the scheduled operation10464/4062.71/I-IV/< 20ng/ml///5Bao et al.,(2020, China) [32]retroprospectivebefore surgerythe primary cohort:523; the validation cohort:205the primary cohort:304/219; the validation cohort:120/8561the primary cohort: 64.7; the validation cohort:53II-III81< 75 nmol/L<47.5nmol/L, ≥ 47.5nmol/L0.564 (0.352–0.904)/7Wesselink et al.,(2020,Netherlands) [33]prospectiveat diagnosis1169751/41867/I-III/< 50nmol/L< 50 nmol/L; ≥ 50 nmol/L/0.53(0.31–0.89)8Xingyu et al.,(2020,China) [34]prospectivebefore surgery11881/37////< 20ng/ml///5Total93245541/378364.09 ± 2.11
Incidence and risk factors of blood 25(OH)D deficiency in the peri-operative period
The cut-off values of blood 25(OH)D deficiency from the included studies were presented in Table 1. As shown in Fig. 2A, the incidence of peri-operative blood 25(OH)D deficiency was ranging from 25.58 to 96.46%, estimated of 59.61% (95% CI, 45.74–73.48) in the peri-operative period. Furthermore, the incidence of blood 25(OH)D deficiency post-operatively was higher than that pre-operatively, reaching for 66.60% (95% CI: 39.09–94.16; Fig. 2B) with significant heterogeneity. Male, rectum tumor, spring and winter sampling were the risk factors for peri-operatively blood 25(OH)D deficiency, with a pooled RR of 1.09 (95% CI: 1.03–1.16) in male; 1.23 (95% CI: 1.03–1.47) in rectum tumor and 1.24 (95% CI: 1.02–1.49) in spring and winter sampling, more detail shown in Fig. 3.
Fig. 2. Estimated incidence of peri-operative blood 25(OH)D deficiency in colorectal cancer. (A) Single-arm meta-analysis of the incidence of blood 25(OH)D deficiency in pre- and post-operative period in enrolled cases. (B) Subgroup analysis of the incidence of blood 25(OH)D deficiency in pre- or post-operative period in enrolled cases by using single-arm meta-analysis
Fig. 3. Subgroup analysis of risk factor for peri-operative blood 25(OH)D deficiency in patients with colorectal cancer
Meta-analysis for overall survival
The associations between low peri-operatively blood 25(OH)D and overall survival(OS) were reported in seven cohorts with 3104 cases (Fig. 4). Based on a random-effects model (I^2^ = 46.5%), the combined result showed that low peri-operative blood 25(OH)D was significantly associated with poor OS (Fig. 4A, HR = 0.67, 95% CI = 0.52–0.87) when the highest tertiles compared with the lowest tertiles. The subgroup analysis between the pre- or post-operative time-point were conducted, and found that low post-operatively blood 25(OH)D (HR = 0.63, 95% CI: 0.50–0.80; I^2^ = 0%) was more likely to contribute to pooer OS than low pre-operative level (HR = 0.71, 95% CI: 0.46–1.10) as shown in Fig. 4B. Furthermore, in terms of the impact on short-term survival outcome (< 5 years) and long-term survival outcome (≥ 5 years), the pooled results showed that low peri-operative level of blood 25(OH)D affected both short-term and long-term survival outcome. And the HR for short-term survival outcome was 0.43 (95%CI:0.24–0.77, Fig. 4C) without heterogeneity, while the HR for long-term survival outcome was 0.72 (95%CI:0.55–0.94) with the I^2^ of 52.1%. The funnel plot showed in Supplemental Fig. 1A and p value of Egger’s test was 0.055, indicating no potential publication bias.
Fig. 4. Meta-analysis of the effect of peri-operative blood 25(OH)D level on overall survival. (A) Forest plot for the association of highest vs. lowest 25(OH)D levels in pre- and post-operative period with overall survival in patients with colorectal cancer. (B) Subgroup analysis of forest plot for the association of highest vs. lowest 25(OH)D levels in pre- or post-operative period with overall survival in patients with colorectal cancer. (C) Subgroup analysis of forest plot for the association of highest vs. lowest 25(OH)D levels in short term(< 5 years) or long term (≥ 5 years) with overall survival in patients with colorectal cancer
Meta-analysis for all-cause mortality
The effects of peri-operative blood 25(OH)D status on all-cause mortality in CRC patients were also assessed in the present study. Five cohorts with long-term survival outcome (larger than 5 years) comprising 6981 patients reported the prognostic value of blood 25(OH)D in the peri-operative period for all-cause mortality (Fig. 5A). The results suggested that lower level of peri-operative blood 25(OH)D was strongly associated with higher all-cause mortality (HR = 0.64, 95% CI: 0.55–0.73) without heterogeneity (I^2^ = 0.0%). As shown in Fig. 5B, the subgroup analysis showed that lower blood 25(OH)D status pre-operatively (HR = 0.47, 95% CI:0.31–0.70) was inclined to have higher all-cause mortality than lower blood 25(OH)D post-operatively (HR = 0.67, 95% CI: 0.57–0.80) with an I^2^ value of 0%. However, the funnel plot was observed and Egger’s test (p = 0.03; Supplemental Fig. 1B) implied a potential publication bias.
Fig. 5. Meta-analysis of the effect of peri-operative blood 25(OH)D level on all-cause mortality. (A) Forest plot for the association of highest vs. lowest 25(OH)D levels in pre- and post-operative period with all-cause mortality in patients with colorectal cancer. (B) Subgroup analysis of forest plot for the association of highest vs. lowest 25(OH)D levels in pre- or post-operative period with all-cause mortality in patients with colorectal cancer
Discussion
Adequate data suggested getting enough vitamin D could lower the risk of formation and incidence in CRC, highlighting the important role of vitamin D in CRC prevention [35]. Furthermore, the vitro studies also found that vitamin D evidently regulated cell proliferation and apoptosis, and promoted cellular differentiation to prevent the development of cancer [36]. However, the impact of vitamin D levels in peri-operative period on CRC patients’ prognosis was still inconsistent. It was challenging to provide precise time of intervention due to failure in specifying the exact time of blood collection, resulting from ignoring effects of peri-operative time of blood 25(0 H)D on CRCs treatment and outcomes, even though a few prior articles suggested the level of circulating vitamin D was associated with the prognosis in colorectal patients [[37](#CR37), [38](#CR38)]. Furthermore, vitamin D levels were fluctuating greatly and rapidly during surgery, which might lasting for three months or longer before the concentration recovers to “normal” levels [[39](#CR39)]. So an integrated meta-analysis was conducted to identify the role of peri-operative blood 25(0 H)D in survival outcome in CRCs patients. It was found that the incidence of peri-operative vitamin D deficiency was pretty high and did have a significantly negative impact on survival outcome.
14 studies were included comprising 9324 CRC’s patients in this systematic review. The findings revealed that the incidence of peri-operatively blood 25(OH)D deficiency had significantly over 50%, despite some substantial variability due to regional variations in vitamin D status [40]. Additionally, it was demonstrated by the estimated data from subgroup meta-analysis that the incidence of blood 25(OH)D deficit in post-operative period was higher than that in pre-operative period. As Vaughan-Shaw et al. previously reported, the authors found that blood 25(OH)D levels were lower in the twelve months following surgery, then recovering after twenty-four months [25]. The incidence of 25(OH)D deficiency after surgery was higher than that before surgery as shown in our findings, which was more likely to be caused by plasma loss during surgery or peri-operative anxiety, stress, fasting and other conditions [41]. Therefore, the impact of the deficiency in peri-operative period on tumor metastases and deterioration did warrant more investigation, even though 25(OH)D was more reported to be related to the onset of colorectal cancer [41, 42].
In the current study, the potential risk factors for 25(OH)D deficiency peri-operatively were also analyzed and revealed that male, rectum tumor, spring, and winter sampling were the significant risk variables. For sex deference, some literature evidenced the importance of some gender-specific determinants of circulating 25(OH)D as factors to be considered rather than straight differences in vitamin D basal levels between males and females [43]. As an example, higher incidence of colorectal carcinomas in men had been linked to male sex hormones compared with women [44]. Additionally, smoking [45] and low physical activity [46] seemed predictors of vitamin D deficiency in men, which exerted a continuous impact on vitamin D status in the peri-operative period. On the other hand, meta-analysis showed that rectum cancer had higher risk occurring peri-operative 25(0 H)D deficiency when compared with colon cancer, which might be related to rectal mucosal gene expression. It was found that normal rectal mucosal gene expression signature could induce higher 25-OHD level [47], while partial rectal resection and mucosal damage resulting from surgery probably lead to reduced plasma vitamin D level. The reduction in blood 25(0 H)D samples taken in spring and winter correlated with the lack of seasonal sunlight exposure, since adequate sunlight exposure was one of the main sources of vitamin D supplementation [48]. However, BMI and ACJJ stage were not the significant risk factors for low blood 25(0 H)D levels in this study. However, it is worth noting that in both inflammatory bowel disease (IBD) and Crohn’s disease (CD), there was a negative association between BMI and vitamin D serum levels [49]. A previous systematic review showed significant but weak correlation between BMI and 25-OHD in adults [50], However, another’s report revealed that BMI was not an independent predictor of low 25-OHD levels [17], so whether BMI was a risk factor for low plasma 25-OHD levels during CRC`s treatment remains controversial.
Low circulating 25(OH)D concentration throughout peri-operative period was greatly associated with overall survival and all-cause mortality, indicating that the vitamin D fluctuation and deficiency during surgery could result in adverse prognosis. As for overall survival, the subgroup analysis was conducted and revealed that association between the post-operative 25(OH)D and overall survival was more prominent than that before surgery. To our best knowledge, this was the first time to identify the role of the post-operative blood 25(OH)D level on overall survival in CRC by systematic review, especially in short-term survival(< 5 years), which facilitated to provide a time point for target clinical intervention. Animal researches showed that sufficient vitamin D could hinder the progression of CRC through multiple pathways, including Wnt/β-catenin, apoptosis, and inflammation [51]. Furthermore, vitamin D could enhance survival of CRC`s patients through increasing immune modulation [52], attenuation of fatigue symptoms [53], and a decrease of mood disorders or depression [54]. As mentioned above, post-operative vitamin D deficiency was highly prevalent and sustained for a long time, which could lead to dysregulation of anticancer pathways, contributing to the deterioration of CRC. On the contrary, patients with a high vitamin D level after surgery through supplementation presented better disease-free survival and overall survival than patients with low vitamin D level [55], which fostered the evidence that the importance of follow-up monitoring and supplementation of vitamin D level after surgery for CRC patients.
The role of peri-operative 25(OH)D level in all-cause mortality was also evaluated in this study. Although CRC-specific mortality might have more reference value, it was difficult to meta because the small number of articles describing CRC-specific mortality associated with the peri-operative 25(OH)D level. All articles for analyzing all-cause mortality included followed-up lasting for over 5 years, and the finding revealed that low peri-operative blood 25(OH)D level also resulted in the elevated all-cause mortality. Interestingly, the impact of low 25(OH)D pre-operatively was more pronounced than post-operatively on all-cause mortality. Inflammation was possibly one of the potential underlying processes explaining the link between vitamin D and all-cause mortality [56]. Cancer progression was significantly influenced by inflammation [57] and vitamin D’s active form (1,25-dihydroxycholecalciferol) has anti-inflammatory characteristics [58]. Inflammation might contribute to the development of comorbid conditions like cardiovascular disease [59], which was experienced by many cancer survivors [60]. Not to be overlooked, the systemic inflammatory response (SIR) possibly had an important confounding effect in the correlation between vitamin D and cancer survival outcomes, with some scholars suggesting that low plasma 25(OH) concentrations were a consequence of persistent SlR, as there was a recognized association between the presence of SIR and poor prognosis in cancer patients [61]. There was consistent evidence that plasma levels of the most common micronutrients, such as vitamin D, decreased progressively in mild, severe to profound inflammation [62]. Clearly, most plasma micronutrients were part of the systemic inflammatory response. It was recommended that measurements of plasma micronutrient concentrations should be performed in conjunction with measurements of inflammatory responses in patients with acute or chronic disease. However, few of the included studies analyzed the association between SIR markers and vitamin D, resulting in a lack of meta-analysis to verify.
This study had some limitations. Firstly, the number of studies included was still small. Although seven large database were searched and the references of included studies were checked, we cannot exclude having missed a relevant study. Second, there was significant heterogeneity in the combined results of the incidence of blood 25(OH)D deficiency peri-operatively due to regional and population variations. There were variations in units and cut-off values because of different trials and cohorts, but all our meta-analyses were comparing highest level and lowest level. And overall results were remarkably consistent across studies without heterogeneity. For the exact time of blood drawing in our included studies, the pre-operative time was at diagnosis or within a week before surgery, while the post-operative time was mostly within a week or a month after surgery and only one study was three months after surgery, but the results of meta-analysis were generally consistent after sensitivity analysis.
Conclusion
There was a high peri-operative incidence of circulating 25(OH)D deficiency in CRCs patients. Both the pre-operative and post-operative vitamin D level was greatly associated with the survival outcome in CRC patients. Due to the possible confounding effect of SIR in the correlation between vitamin D levels and colorectal survival, simultaneous measurement of vitamin D and SIR in the peri-operative period are essential for improving CRCs survival outcome.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H Ferlay J Siegel RL Laversanne M Global Cancer statistics 2020: GLOBOCAN estimates of incidence and Mortality Worldwide for 36 cancers in 185 countries CA Cancer J Clin 2021712094910.3322/caac.2166033538338 · doi ↗ · pubmed ↗
- 2Siegel RL Miller KD Goding Sauer A Colorectal cancer statistics, 2020 CA Cancer J Clin 20207031456410.3322/caac.2160132133645 · doi ↗ · pubmed ↗
- 3Pramateftakis MG Optimizing colonic cancer surgery: high ligation and complete mesocolic excision during right hemicolectomy Tech Coloproctol 201014 Suppl 1S 495110.1007/s 10151-010-0609-920697925 · doi ↗ · pubmed ↗
- 4Xu RH Muro K Morita S Modified XELIRI (capecitabine plus irinotecan) versus FOLFIRI (leucovorin, fluorouracil, and irinotecan), both either with or without bevacizumab, as second-line therapy for metastatic colorectal cancer (AXEPT): a multicentre, open-label, randomised, non-inferiority, phase 3 trial Lancet Oncol 20181956607110.1016/S 1470-2045(18)30140-229555258 · doi ↗ · pubmed ↗
- 5Miller KD Nogueira L Devasia T Cancer treatment and survivorship statistics, 2022 CA Cancer J Clin 20227254093610.3322/caac.2173135736631 · doi ↗ · pubmed ↗
- 6Kwon YH Lim HK Kim MJ Impacts of anemia and transfusion on oncologic outcomes in patients undergoing surgery for colorectal cancer Int J Colorectal Dis 202035713112010.1007/s 00384-020-03601-232363477 · doi ↗ · pubmed ↗
- 7Xie H Wei L Liu M Yuan G Tang S Gan J Preoperative computed tomography-assessed Sarcopenia as a predictor of complications and long-term prognosis in patients with colorectal cancer: a systematic review and meta-analysis Langenbecks Arch Surg 202140617758810.1007/s 00423-021-02274-x 34406490 · doi ↗ · pubmed ↗
- 8Chen JH Zhai ET Yuan YJ Systemic immune-inflammation index for predicting prognosis of colorectal cancer World J Gastroenterol 2017233462617210.3748/wjg.v 23.i 34.626128974892 PMC 5603492 · doi ↗ · pubmed ↗