Chronic Ileum Obstruction, Granulation, and Ulceration With IgG4-Positive Plasma Cell Infiltration in a Six-Year-Old Girl With 21trisomy
Hiroshi Yamanaka, Masahiro Ueki, Keisuke Kikuchi, Satoshi Yakuwa

TL;DR
A six-year-old girl with 21trisomy developed chronic ileum obstruction and inflammation, which was successfully treated with surgery and linked to her immunological and gastrointestinal issues.
Contribution
This case highlights a novel association between IgG4-positive plasma cell infiltration and gastrointestinal complications in a patient with 21trisomy.
Findings
Surgical resection resolved ileum obstruction and normalized fecal calprotectin levels.
Pathological findings included intussusception, ischemia, ulceration, and IgG4-positive plasma cell infiltration.
The condition is linked to immunological and gastrointestinal disorders in 21trisomy patients.
Abstract
Patients with 21trisomy often develop congenital or acquired gastrointestinal diseases, such as duodenal or anal atresia, celiac disease, intussusception, and constipation. In these patients, it is often challenging to diagnose gastrointestinal diseases because most patients have difficulty explaining their complaints in detail. Furthermore, these patients also possess immunological disorders, such as increased type I interferon activation, innate immune hypersensitivity, and polarization to autoimmune. Here, we present a girl with 21trisomy and constipation who developed severe anemia, occult blood and elevated levels of calprotectin in stool, and chronic ileum obstruction confirmed by computed tomography. The patient underwent surgical resection of the ileum and recovered without complications. Pathological examination demonstrated intussusception, ischemia, ulceration, inflammatory…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
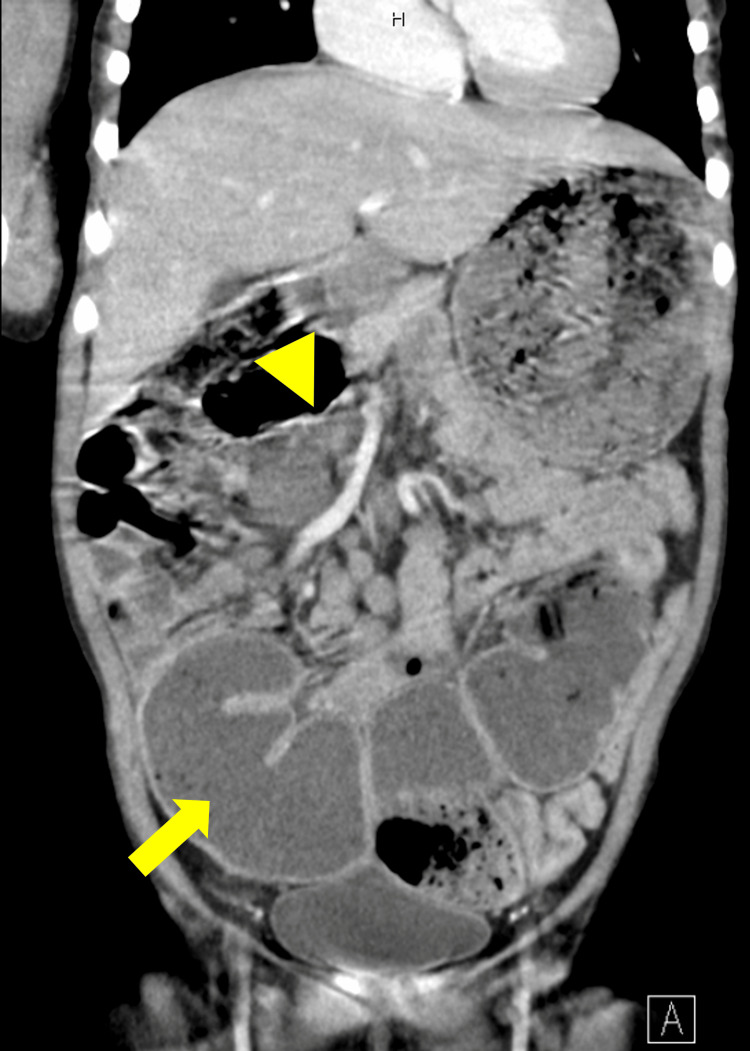 Figure 1
Figure 1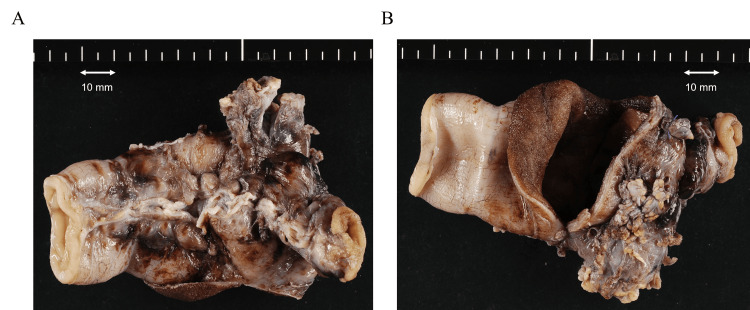 Figure 2
Figure 2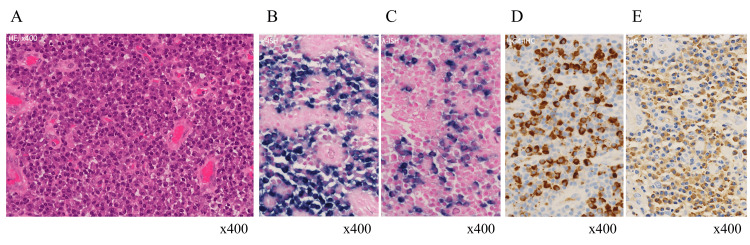 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIgG4-Related and Inflammatory Diseases · Gastrointestinal disorders and treatments · Biliary and Gastrointestinal Fistulas
Introduction
21trisomy is one of the major genetic disorders for pediatricians. Patients with 21trisomy demonstrate systemic manifestations, such as facial features including epicanthic folds, oblique palpebral fissures, a depressed nasal bridge, an upturned nose, intellectual disability, impaired motor development by low muscle tonus, congenital cardiac diseases, endocrinological and metabolic disorders, hematologic disorders, ophthalmologic diseases, and gastrointestinal diseases. Gastrointestinal diseases are one of the major complications caused by congenital (atresia of the esophagus, duodenum, ileum, or anus) or acquired reasons such as celiac diseases or constipation [1].
Abdominal distention is a common manifestation in children. The most common cause is constipation, and there are several other factors, such as obstruction by intussusception, Meckel band, inflammatory bowel disease, ascites, or functional problems such as paralytic ileus [2].
In patients with 21trisomy, severe complications of the infection and autoimmune diseases, such as thyroiditis, type I diabetes mellitus, and celiac diseases, are the characteristics. Recent studies demonstrated that these patients possess immunological disorders, such as increased type I interferon production, increased innate immune response, and polarization to autoimmunity [3-5].
Patients with 21trisomy are complicated with intellectual disabilities and could not explain their complaints in detail. Indeed, clinicians had difficulty in making the diagnosis of these patients, which could be associated with delayed diagnoses [6,7].
Here, we report a six-year-old girl with 21trisomy, ventricular septum defect, and constipation, who demonstrated severe anemia, abdominal distention, occult blood, and elevated calprotectin levels in the stool. She underwent surgical resection of the ileum and recovered without complications. Pathological examination demonstrated the intussusception with ischemia, inflammatory granulation, ulceration, and massive IgG4-positive plasma cell infiltration around the ulcer. These manifestations were caused by the intellectual, gastrointestinal, and immunological disorders in the patient with 21trisomy.
Case presentation
The patient developed mild respiratory distress at birth, although there were no significant signs during pregnancy. She was diagnosed with transient tachypnea of the newborn and ventricular septum defect. Also, distinct facial characteristics such as a flat face and upward palpebral slant were noticed. G-band karyotyping test demonstrated 21 trisomy. She received regular evaluations from the pediatricians. She developed constipation treated with high dose picosulfate sodium and magnesium oxide at 1.5 years old and moderate developmental retardation.
At six years old, she came to the hospital for a regular assessment and demonstrated lethargy and a pale face, although previous laboratory examinations performed nine months ago showed no anemia (Hb 14.0 g/dl). Although the patient did not show significantly decreased oral intake or vomit, physical examination demonstrated abdominal distention and mild tenderness of the upper abdominal area without muscular defense. Laboratory examination data was as follows: WBC 6200 cells/μl (neut 64%, lymph 28%, mono 6.0%, Eos 1.0%), RBC 2.65x10^6 cells/μl, Hb 4.3 g/dl, hematocrit 18.0%, mean corpuscular volume (MCV) 67.9 fl, mean corpuscular hemoglobin (MCH) 16.2 pg, mean corpuscular hemoglobin concentration (MCHC) 23.9%, platelet (Plt) 476 x10^3/μl. Prothrombin time-international normalized ratio (PT-INR) 0.98, activated partial thromboplastin time (APTT) 23.8 sec, blood urea nitrogen (BUN) 19.3 mg/dl, Cre 0.38 mg/dl, Fe 0.7 μg/L, unsaturated iron-binding capacity (UIBC) 44.3 μg/L, ferritin 5.0 ng/ml, C-reactive protein 0.6 mg/L, IgG 9.61 g/L, IgG4 0.823 g/L, IgA 1.73 g/L, IgM 0.56 g/L. Severe microcytic hypochromic anemia was confirmed, whereas no overt bleeding was noticed in this period. A detailed examination demonstrated occult blood (Hb 551 U/L) and elevated calprotectin levels (2650 μg/g, normal range < 50 μg/g) in the stool. An enlarged ileum with possible stenosis was confirmed in the contrast-enhanced computed tomography (CT) scan (Figure 1). Since there was no sign of ischemia, she was treated conservatively with fasting and iron supplements. The patient got well after a resolution of anemia and took foods and drinks orally without vomiting, although abdominal distention was not resolved.
Dilated ileum (indicated with an arrow) and possible stenosis (indicated with an arrowhead) in a contrast-enhanced computed tomography scan.
After two months, she received the contrast-enhanced CT scan which demonstrated persistent ileum dilation. She underwent exploratory laparoscopic surgery for possible stenosis or ileum duplex. Pediatric surgeons found stenosis in the middle section of the ileum and resected it. The resected intestine showed short intussusception (Figure 2).
Focal dilation and ischemic change in the resected ileum.The oral side is located on the left of the photograph. An Outer appearance without section B Internal appearance of focal dilation with section.
Pathological examination demonstrated incarceration, ulcer, granulation, and massive infiltration of inflammatory cells, predominantly IgG4-positive plasma cells (Figure 3). Infiltration of IgG4-positive cells was found only around the ulcer and granulation. After the surgery, the ileum dilation did not relapse and the fecal calprotectin level was normalized. She got well without complications.
Massive filtration of IgG4-positive plasma cells in the ileum by pathological examination.A: Massive plasma cell infiltration in hematoxylin-eosin staining; B and C: Normal surface immunoglobulin by in-situ hybridization. κ-chain (B) and λ-chain (C); D and E: Significant IgG4 positive cells by immunohistochemistry of IgG4 (D) and IgG (E).
Discussion
Our patient demonstrated chronic obstruction by intussusception. Although ischemia was confirmed by pathological examination, severe necrosis or perforation was not noted. Intussusception except in infants could be associated with organic problems such as lymphoma or Meckel’s diverticulum. In this patient, granulation and ulceration with IgG4-positive plasma cell infiltration was the only manifestation that could be associated with intussusception.
Related to the intestinal inflammation, elevated levels of fecal calprotectin were confirmed in this patient. Fecal calprotectin is one of the neutrophilic intestinal inflammation markers. Its elevation was reported in inflammatory bowel diseases, granulomatous colitis in chronic granulomatous disease, celiac disease, and food-protein-induced enterocolitis [8,9]. As her symptoms and laboratory data were not compatible with these diseases, we assumed that neutrophilic inflammation and granulation were associated with elevated fecal calprotectin levels. In addition, neutrophils and monocytes in patients with 21trisomy demonstrate hypersensitivity to lipopolysaccharide [3]. Intestinal mucosal damage by chronic constipation and ileum dilation could permit enterobacterial invasion leading to hyperinflammation by neutrophils and monocytes. Indeed, elevated levels of calprotectin were normalized after the surgery (41 ug/g).
Associated with inflammation, massive IgG4-positive plasma cell infiltration and mild fibrosis were confirmed in our patient. Although these manifestations were one of the characteristics of IgG4-related diseases, granulation was one of the exclusion criteria for IgG4-related diseases [10]. Furthermore, IgG4-positive plasma cell infiltration was confirmed only around the granulation and ulcer in this patient. IgG4-positive plasma cell infiltration is also found in inflammatory bowel disease [11]. In patients with inflammatory bowel diseases who underwent surgical resection of the intestine or endoscopic biopsy, approximately 20% to 40% of patients demonstrated IgG4-positive plasma cell infiltration [12,13]. Although the pathophysiology of IgG4-positive plasma cell infiltration has not been determined, this phenomenon could be associated with the activation or suppression of immune cells in the intestine. We assumed that a similar immunological response occurred in the patient’s ileum.
Although the patient does not demonstrate any symptoms associated with irritable bowel disease or IgG4-related diseases after the surgery, successive evaluation of the development of these diseases is necessary.
Conclusions
We experienced a patient with 21trisomy developing severe anemia and ileum stenosis. This case is rare, but it could suggest the importance of careful evaluation of abdominal distention including the treatment of the constipation, especially in patients with 21trisomy. To evaluate abnormal intestinal conditions by the inflammation, fecal calprotectin could be a potential marker, although more detailed evaluations are needed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Feeding problems and gastrointestinal diseases in Down syndrome Arch Pediatr Ravel A Mircher C Rebillat AS Cieuta-Walti C Megarbane A 53602720203178429310.1016/j.arcped.2019.11.008 · doi ↗ · pubmed ↗
- 2Chronic constipation: a review of literature Medicine (Baltimore) Forootan M Bagheri N Darvishi M 097201810.1097/MD.0000000000010631 PMC 597634029768326 · doi ↗ · pubmed ↗
- 3Altered endotoxin responsiveness in healthy children with Down syndrome BMC Immunol Huggard D Mc Grane F Lagan N 311920183039064010.1186/s 12865-018-0270-z PMC 6215672 · doi ↗ · pubmed ↗
- 4Excessive negative regulation of type I interferon disrupts viral control in individuals with Down syndrome Immunity Malle L Martin-Fernandez M Buta S Richardson A Bush D Bogunovic D 207420845520223624300810.1016/j.immuni.2022.09.007PMC 9649881 · doi ↗ · pubmed ↗
- 5Autoimmunity in Down's syndrome via cytokines, CD 4 T cells and CD 11c(+) B cells Nature Malle L Patel RS Martin-Fernandez M 30531461520233681396310.1038/s 41586-023-05736-y PMC 9945839 · doi ↗ · pubmed ↗
- 6Superior mesenteric artery syndrome in Down syndrome: a case report Cureus Alshaibani F 014202210.7759/cureus.31854 PMC 979232936579270 · doi ↗ · pubmed ↗
- 7Navigating a complex presentation: management of hypernatremic dehydration, acute kidney injury, hyperkalemia, and metabolic acidosis in a patient with Down syndrome: a case report Cureus Al-Nattah M Abdullah A Alkhateeb N Abu Qaoud H Al Ali A Alzakeebeh O 015202310.7759/cureus.46053 PMC 1060458637900476 · doi ↗ · pubmed ↗
- 8Fecal calprotectin and organic gastrointestinal disease: a systematic review Cureus Asiri AS Algarni SS Althubaiti AQ Alzubaidi MA Alghamdi JA Almalki GA 015202310.7759/cureus.45019 PMC 1056588237829963 · doi ↗ · pubmed ↗