Preoperative breast MRI positively impacts surgical outcomes of needle biopsy–diagnosed pure DCIS: a patient-matched analysis from the MIPA study
Andrea Cozzi, Giovanni Di Leo, Nehmat Houssami, Fiona J. Gilbert, Thomas H. Helbich, Marina Álvarez Benito, Corinne Balleyguier, Massimo Bazzocchi, Peter Bult, Massimo Calabrese, Julia Camps Herrero, Francesco Cartia, Enrico Cassano, Paola Clauser, Marcos F. de Lima Docema

TL;DR
Preoperative MRI for pure DCIS increases mastectomy rates but significantly reduces the need for reoperations after surgery.
Contribution
This study shows that preoperative MRI reduces reoperations more than it increases mastectomies in pure DCIS patients when confounding factors are matched.
Findings
MRI group had a 20.1% first-line mastectomy rate compared to 11.0% in the noMRI group.
MRI group had a 10.0% reoperation rate compared to 22.0% in the noMRI group.
Reduction in reoperations from MRI was more than twice the increase in mastectomies.
Abstract
To investigate the influence of preoperative breast MRI on mastectomy and reoperation rates in patients with pure ductal carcinoma in situ (DCIS). The MIPA observational study database (7245 patients) was searched for patients aged 18–80 years with pure unilateral DCIS diagnosed at core needle or vacuum-assisted biopsy (CNB/VAB) and planned for primary surgery. Patients who underwent preoperative MRI (MRI group) were matched (1:1) to those who did not receive MRI (noMRI group) according to 8 confounding covariates that drive referral to MRI (age; hormonal status; familial risk; posterior-to-nipple diameter; BI-RADS category; lesion diameter; lesion presentation; surgical planning at conventional imaging). Surgical outcomes were compared between the matched groups with nonparametric statistics after calculating odds ratios (ORs). Of 1005 women with pure unilateral DCIS at CNB/VAB (507…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
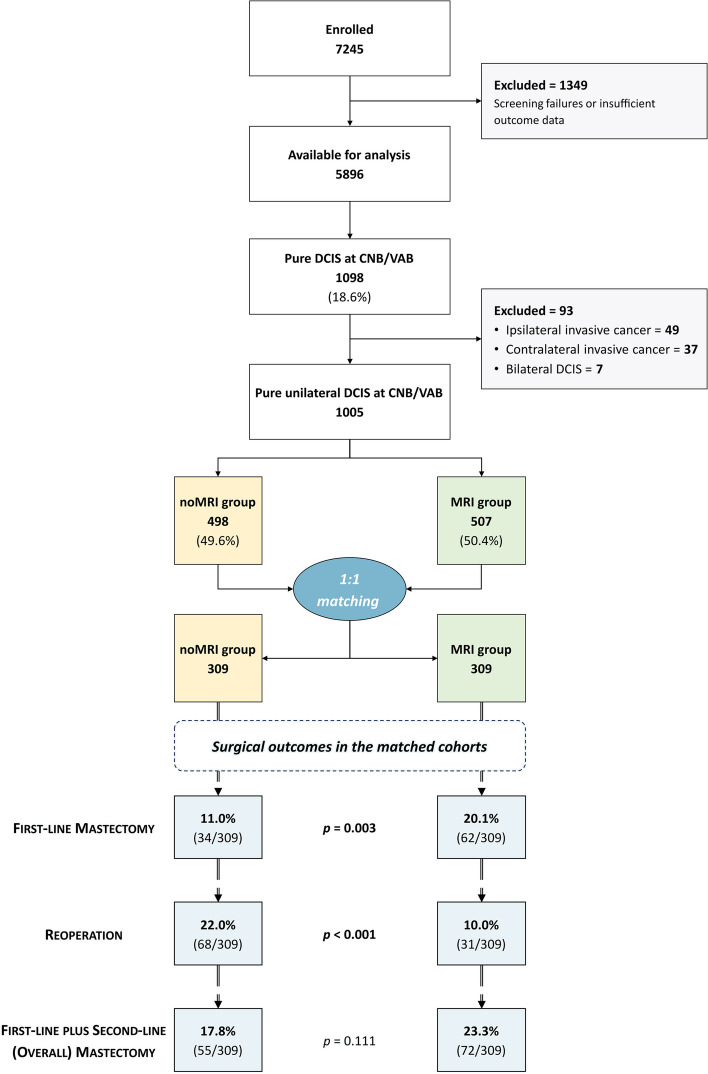 Figure 1
Figure 1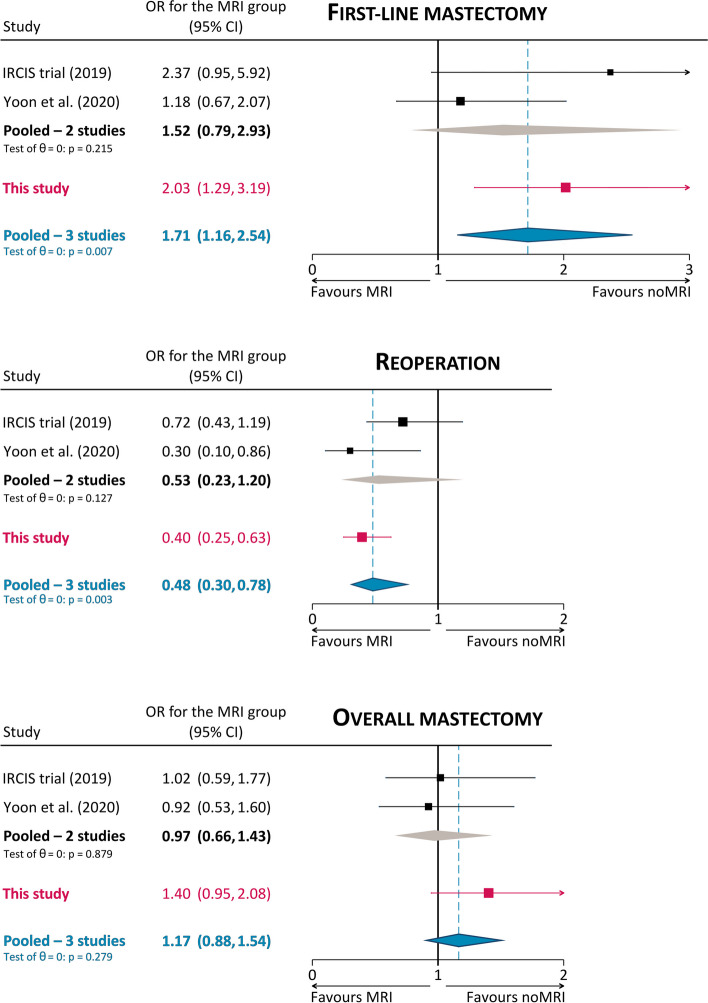 Figure 2
Figure 2- —http://dx.doi.org/10.13039/100004326Bayer
- —Università degli Studi di Milano
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInnovation Diffusion and Forecasting · Customer churn and segmentation
Introduction
The role of preoperative breast magnetic resonance imaging (MRI) in guiding the treatment of ductal carcinoma in situ (DCIS) diagnosed at core needle biopsy (CNB) or vacuum-assisted biopsy (VAB) is an open issue in clinical practice [1–4] that has been extensively investigated considering different outcomes, e.g., short-term surgical results [5–16], upgrade to invasive cancer at final pathology [17, 18], detection of additional ipsilateral or contralateral disease [19], long-term recurrence [20], and patient preferences [21, 22]. Surgical outcomes are crucial, as the rate of mastectomy and the rate of reoperation after breast-conserving surgery are major indicators of breast care quality and the focus of multidisciplinary efforts towards surgical de-escalation [23–25].
As shown by three systematic reviews published between 2015 and 2021 [26–28], cohort studies that investigated the effects of preoperative MRI on surgical outcomes of DCIS generally exhibit a referral bias towards MRI for young patients with extensive and high-grade DCIS. These characteristics represent strong confounding factors, being intrinsically associated with poor outcomes and ultimately prompting more aggressive surgery [27, 29]. Naturally, these studies outline contrasting scenarios and add to ongoing uncertainty about the impact of preoperative MRI on surgical outcomes [27, 28].
However, different results emerge from the very few studies adopting methods to minimize or remove the referral bias [30]. Save for the very small subgroups of DCIS in the MONET randomized controlled trial [31], as of mid-2023, only two studies present such characteristics: the IRCIS randomized controlled trial [11] and the propensity score matching study by Yoon et al [15]. Pooled together, data from these two studies show that, compared to patients not referred to preoperative MRI, patients with DCIS undergoing preoperative MRI have a 1.52 odds ratio (OR) of undergoing mastectomy as their initial surgery, a 1.89 OR of having negative margins and avoiding reoperation, and a 0.97 OR of overall mastectomy (at first-line surgery or at reoperation). Nonetheless, as noted in the conclusions of a systematic review by the European Commission Initiative on Breast Cancer working groups [27], estimates from these studies remain affected by low statistical power.
In this context, the present study takes advantage of the large cohort of patients with DCIS registered in the database of the Multicenter International Prospective Analysis (MIPA) study [32–34], which allows the application of methods for confounder adjustment while still retaining a large number of patients. Thus, we aimed to compare in matched cohorts the surgical outcomes of patients with DCIS referred or not referred to preoperative MRI, namely the first-line mastectomy rate, the reoperation rate, and the overall mastectomy rate.
Materials and methods
Study design
This is a subgroup analysis of data from the MIPA study (ISRCTN41143178), whose design is detailed in the protocol paper [32]. In summary, MIPA is a prospective observational study conducted in 27 centers worldwide between June 2013 and November 2018, after approval from the Ethics Committee of the coordinating center (Comitato Etico Ospedale San Raffaele, Milano, Italy; protocol number 2784). Each center consecutively enrolled women aged 18–80 years with newly diagnosed breast cancer, without indication for neoadjuvant therapy and amenable to upfront surgery. In accordance with the observational nature of the study, each multidisciplinary team followed local routine practice in the diagnostic and therapeutic pathway, including the decision on whether to refer patients to bilateral contrast-enhanced preoperative MRI after conventional imaging with digital mammography and/or ultrasonography (US).
Study population and endpoints
According to the aforementioned aims, this study focuses on patients with a diagnosis of pure unilateral DCIS at CNB/VAB, as the presence of ipsilateral and/or contralateral invasive cancer and the presence of bilateral DCIS are known to influence surgical management [35, 36], acting as strong potential confounding factors.
Following the study protocol [32], surgical endpoints for all patients in this analysis are (i) first-line mastectomy; (ii) immediate/short-term reoperation for close or positive margins; and (iii) overall mastectomy (i.e., performance of mastectomy as first-line surgery or at reoperation). Due to the focus on unilateral lesions, the secondary endpoint of first-line bilateral mastectomy is excluded from this analysis.
Conversely, data on non-surgical secondary study endpoints based on surgical pathology (such as the upgrade of DCIS to invasive cancer and complete DCIS removal) will not be considered in this analysis and will be separately reported for all patients with pure DCIS at CNB/VAB.
Patient matching
The nonrandomized observational design of the MIPA study implies the existence of different selection biases towards the referral to MRI, yielding a skewed distribution of several characteristics (i.e., covariates) between patients who underwent MRI before surgery (MRI group) and those who did not undergo MRI (noMRI group). Thus, patient matching was implemented to reduce covariate imbalance, to estimate the average effect of preoperative MRI on surgical outcomes in the population at clinical equipoise, i.e., patients with overlapping baseline characteristics [37, 38].
To strictly adhere to the real-world workflow of breast cancer care, the following baseline characteristics—all already available before the decision to refer (or not) patients to MRI—were considered covariates for patient matching (Table 1): age; hormonal status; presence of familial breast cancer risk1; posterior-to-nipple diameter2; highest BI-RADS category at conventional imaging; lesion diameter at conventional imaging; lesion presentation at conventional imaging3; surgical planning after conventional imaging.Table 1. Comparison of baseline demographic, clinical, and imaging characteristics in the unmatched and matched cohortsUnmatched cohortsMatched cohortsnoMRIMRIpSMDnoMRIMRIpSMDPatients498507––309309––Mean age (SD)59 years (10)56 years (10) < 0.0010.26757 years (10)57 years (9)0.8650.013Hormonal statusPremenopausal118 (23.8%)140 (27.6%)0.2290.13285 (27.5%)75 (24.3%)0.4620.022Perimenopausal49 (9.9%)62 (12.2%)32 (10.4%)43 (13.9%)Receiving HRT3 (0.6%)2 (0.4%)2 (0.6%)1 (0.3%)Post-menopausal326 (65.7%)303 (59.8%)190 (61.5%)190 (61.5%)Patients with familial breast cancer risk5 (1.0%)11 (2.2%)0.2240.0931 (0.3%)1 (0.3%)1.000 < 0.001Mean posterior-to-nipple diameter (SD)96.2 mm (31.9)89.6 mm (30.3)0.0010.21392.2 mm (26.5)90.9 mm (27.9)0.5540.043Highest BI-RADS at conventional imagingBI-RADS 05 (1.0%)10 (2.0%) < 0.0010.3541 (0.3%)1 (0.3%)1.000 < 0.001BI-RADS 10 (0.0%)4 (0.8%)0 (0.0%)0 (0.0%)BI-RADS 20 (0.0%)8 (1.6%)0 (0.0%)0 (0.0%)BI-RADS 314 (2.8%)33 (6.5%)7 (2.3%)7 (2.3%)BI-RADS 4363 (72.9%)319 (63.0%)238 (77.0%)238 (77.0%)BI-RADS 5116 (23.3%)132 (26.1%)63 (20.4%)63 (20.4%)Lesion presentation at conventional imagingUnifocal433 (86.9%)425 (83.8%)0.0140.185286 (92.6%)286 (92.6%)1.000 < 0.001Multifocal55 (11.0%)54 (10.7%)21 (6.8%)21 (6.8%)Multicentric10 (2.0%)28 (5.5%)2 (0.6%)2 (0.6%)Mean lesion diameter at conventional imaging (SD)20.9 mm (20.4)24.0 mm (20.3)0.0220.15118.0 mm (14.0)18.3 mm (13.4)0.7900.014Planned mastectomy after conventional imaging67 (13.5%)125 (24.7%) < 0.0010.28831 (10.0%)31 (10.0%)1.000 < 0.001SMD standardized mean difference, SD standard deviation, HRT hormone replacement therapy
Using the “MatchIt” package [39] on R (version 4.2.1, The R Foundation for Statistical Computing), nearest neighbor 1:1 matching with the rank-based robust Mahalanobis distance [40, 41] was performed with specifications chosen to optimize covariate balance by taking advantage of the large number of patients in the MIPA study: (i) exact 1:1 matching was enforced for the following categorical covariates: familial breast cancer risk, highest BI-RADS at conventional imaging, lesion presentation at conventional imaging, and surgical planning after conventional imaging; (ii) calipers were applied in the matching of the following continuous covariates: age (caliper width: ± 0.5 standard deviations), posterior-to-nipple diameter (caliper width: ± 2 standard deviations), maximum lesion diameter at conventional imaging (caliper width: ± 0.5 standard deviations). Matching was performed without replacement, and unmatched patients were discarded.
Covariate balance between the MRI and noMRI group was assessed before and after matching by calculating the standardized mean difference for all variables and by performing two-tailed Pearson’s χ^2^ or Fisher’s exact tests for categorical variables and the Mann–Whitney U test for continuous variables. In order to consider matching successful, a conservative combined balance threshold was applied, with all covariates having to display standardized mean differences ≤ 0.050 with p values ≥ 0.100 [42].
Comparison of surgical endpoints
Comparisons of the three surgical endpoints in the unmatched and matched cohorts were carried out with two-tailed Pearson’s χ^2^ or Fisher’s exact tests, as appropriate, after calculation of the respective ORs. To account for multiple testing, the Bonferroni correction was applied considering the 6 comparisons of surgical endpoints in the unmatched and matched cohorts, with an ensuing p < 0.008 threshold for statistical significance. All analyses were performed with R (version 4.2.1, The R Foundation for Statistical Computing) and STATA (version MP 17.1, StataCorp).
Results
Study population
As described in the study flowchart (Fig. 1), 5896 among the 7245 patients enrolled between June 2013 and November 2018 had sufficient information to be considered for this analysis. At least one lesion diagnosed as pure DCIS at CNB/VAB was present in 1098/5896 patients (18.6%): applying the exclusion criteria, 37/1098 (3.4%) patients were excluded because of the presence of a contralateral invasive cancer, 49/1098 (4.5%) because of the presence of another ipsilateral lesion diagnosed as invasive cancer, and 7/1098 (0.6%) because of the presence of bilateral pure DCIS. Thus, 1005 patients with pure unilateral DCIS at CNB/VAB were included in this analysis, 507/1005 (50.4%) in the MRI group and 498/1005 (49.6%) in the noMRI group.Fig. 1. Study flowchart and surgical outcomes in the matched cohorts
As detailed in Table 2, tissue sampling was most frequently prompted by mammographic findings (884/1005 patients, 87.9%), either alone (540/1005 patients, 53.7%) or in combination with US or MRI (344/1005 patients, 34.2%). A total of 658/1005 (65.5%) samplings were performed with VAB, while the remaining 347/1005 (34.5%) with CNB: accordingly, stereotaxis was the most frequent biopsy guidance (673/1005 patients, 67.0%), followed by US (310/1005 patients, 30.8%) and MRI (22/1005 patients, 2.2%).Table 2. Modality of detection of the findings prompting tissue samplingTissue sampling promptNumber%Mammography alone540/100553.7%US alone93/10059.3%MRI alone20/10052.0%Mammography + US194/100519.3%Mammography + MRI89/10058.8%US + MRI8/10050.8%Mammography + US + MRI61/10056.1%US ultrasonography, MRI magnetic resonance imaging
Unmatched cohorts—baseline characteristics
Before matching, different distributions between the noMRI and the MRI group were observed for six of the eight baseline descriptors (Table 1). Patients in the MRI group were younger than those in the noMRI group (mean age 56 years versus 59 years, p < 0.001) and also differed in DCIS presentation at conventional imaging, displaying larger lesions (mean diameter 24.0 versus 20.9 mm, p = 0.022) that were more frequently multifocal or multicentric (16.2% versus 13.0%, p = 0.014). Finally, patients in the MRI group had a + 11.2% difference in the referral to mastectomy after conventional imaging compared to patients in the noMRI group (125/507 patients in the MRI group, 24.7%, versus 67/498 patients in the noMRI group, 13.5%).
Unmatched cohorts—surgical endpoints
As detailed in Table 3, the + 11.2% difference in the referral to mastectomy in the MRI group after conventional imaging rose to + 19.2% in the evaluation of first-line surgery: specifically, the first-line mastectomy rate was 33.5% in the MRI group (170/507 patients) compared to 14.3% (71/498 patients) in the noMRI group (OR 3.03, p < 0.001). While the 12.4% (63/498 patients) reoperation rate of the MRI group was significantly lower (− 7.7%, OR 0.56, p = 0.001) than the 20.1% reoperation rate of the noMRI group (100/498 patients), the overall rate of mastectomy in the MRI group (190/507 patients, 37.5%) was still 17.2% higher (OR 2.36, p < 0.001) than that of the noMRI group (101/498 patients, 20.3%).Table 3. Comparison of surgical outcomes in the unmatched and matched cohortsUnmatched cohorts1005 patientsMatched cohorts618 patientsnoMRI group498 patientsMRI group507 patientsDifference for the MRI groupnoMRI group309 patientsMRI group309 patientsDifference for the MRI group%ORp%ORpFirst-line mastectomy71 (14.3%)170 (33.5%)+ 19.2%3.03< 0.00134 (11.0%)62 (20.1%)+ 9.1%2.030.003Reoperation100 (20.1%)63 (12.4%)− 7.7%0.560.00168 (22.0%)31 (10.0%)− 12.0%0.40< 0.001Overall mastectomy (first-line + second-line)101 (20.3%)190 (37.5%)+ 17.2%2.36< 0.00155 (17.8%)72 (23.3%)+ 5.5%1.400.111MRI magnetic resonance imaging, OR odds ratio
Matched cohorts—baseline characteristics
A total of 618 patients were matched, 309 in each group. As detailed in Table 1, matched patients had a median age of 57 years, being mostly post-menopausal (380/618, 61.5%). At conventional imaging, the most frequent BI-RADS classifications were BI-RADS 4 in 476/618 patients (77.0%) and BI-RADS 5 in 126/618 patients (20.4%). The vast majority of matched patients (572/618, 92.6%) had unifocal presentation at conventional imaging, 42/618 (6.8%) having multifocal DCIS, and only 4/618 patients (0.6%) presenting with multicentric DCIS.
Matched cohorts—surgical endpoints
Starting from the matched 10.0% rate of referral to mastectomy at conventional imaging (31/309 patients in both groups; Table 3), the MRI group still had a significantly higher first-line mastectomy rate (20.1%, 62/309 patients, OR 2.03) compared to the noMRI group (11.0%, 34/309 patients, p = 0.003). However, the reoperation rate in the MRI group (10.0%, 31/309 patients, OR for reoperation 0.40) was less than half that of the noMRI group (22.0%, 68/309 patients, p < 0.001), corresponding to a 2.53 OR of avoiding reoperation for women in the MRI group. This resulted in a non-significant difference (p = 0.111) in the overall mastectomy rate for the MRI group (23.3%, 72/309 patients, OR 1.40) compared to the noMRI group (17.8%, 55/309 patients).
Discussion
This subgroup analysis of the MIPA study focused on 1005 patients with pure unilateral DCIS at CNB/VAB who underwent (507 patients, 50.4%) or did not undergo (498 patients, 49.6%) preoperative MRI, evaluating differences in surgical outcomes between the MRI and noMRI groups. After 1:1 patient matching according to eight covariates concerning demographic, clinical, and imaging characteristics, 309 patients were matched in each group; the significantly higher first-line mastectomy rate of the MRI group (20.1% versus 11.0% in the noMRI group) was counterbalanced by an even higher decrease of reoperations (10.0% in the MRI group versus 22.0% in the noMRI group), culminating in a 5.5% increase in the overall mastectomy rate for the MRI group (23.3% vs 17.8% in the noMRI group) that will need to be clinically contextualized with follow-up data.
As already mentioned, the interpretation of our results must consider methodological peculiarities and limitations both of this study and of previous ones. In the unmatched cohorts, data from all three surgical outcomes (first-line mastectomy, reoperation, overall mastectomy) are in line with pooled data of previous cohort studies reported by the working groups of the European Commission Initiative on Breast Cancer [27]: in our study—before patient matching—preoperative MRI led patients with pure DCIS at CNB/VAB to an even lower OR for reoperation (0.56 versus a pooled 0.72) but to higher OR for first-line mastectomy (3.03 versus a pooled 2.04) and overall mastectomy (2.36 versus a pooled 1.58).
Importantly, in the matched cohort, data from our study confirmed the results obtained by previous studies where randomization [11] or propensity score matching [15] were implemented to deal with confounding factors. As shown in Fig. 2, the 2.03 OR for first-line mastectomy of women in the MRI group was higher than the 1.18 OR obtained by Yoon et al [15] but lower than the 2.37 OR in the IRCIS trial [11]: of note, adding our data to the pooling, the ensuing 1.71 pooled OR reached statistical significance (p = 0.007), substantiating the association between MRI and first-line mastectomy. However, a similar finding could be observed for the protective effect of MRI towards reoperation, underlined by the 0.40 OR in our study, slightly higher than the 0.30 OR obtained by Yoon et al [15] but almost half of the 0.72 OR in the IRCIS trial [11]: adding our data to the pooling confirmed the protective effect of MRI for reoperation, with a significant 0.48 pooled OR (p = 0.003). For the last endpoint (i.e., overall mastectomy), the 1.40 OR of MRI found in our study was higher than the protective 0.92 OR found by Yoon et al [15] and the 1.02 OR found in the IRCIS trial [11]. Nonetheless, as in these two studies, the confidence interval of this OR crosses the no-effect line, not reaching statistical significance (p = 0.111, pooled OR 1.71 with p = 0.279). Notably, our overall mastectomy rates in the matched cohorts (23.3% in the MRI group, 17.8% in the noMRI group) were about half of those found by Yoon et al (38.7% in the MRI group, 40.6% in the noMRI group) [15] and closely comparable to those of the IRCIS trial (17.6% in the MRI group, 17.3% in the noMRI group) [11].Fig. 2. Explorative comparison of surgical outcomes with previous controlled analyses. Odds ratios (OR) refer to women with DCIS undergoing preoperative MRI, with the noMRI group as the reference
At an overall appraisal, results from our study emphasize that when CNB/VAB yields a DCIS diagnosis, women undergoing preoperative MRI have a 2.03 OR of receiving mastectomy as their first-line surgery that is counterbalanced by the 2.53 OR of avoiding reoperation. The focus on biopsy data represents a strong point of our study and allows for the translation of these results into clinical practice, as multidisciplinary teams (and surgeons in particular) do not know in advance the final pathology report—where the case under discussion would be confirmed as a pure DCIS or a DCIS associated with an invasive cancer—but base their decision-making on CNB/VAB results and on what is suggested by imaging findings, in particular extent of calcifications on mammograms, hypoechoic findings at US, or enhancement at MRI. Finally, the non-significant 1.40 OR of the MRI group for overall mastectomy—also due to the loss of cases from the matching process—leaves open the question on whether this OR and the absolute percentage differences found for this surgical outcome (5.5% in our study, 1.9% and 0.3% in the other two studies [11, 15]) are clinically relevant (also in a long-term perspective that will be explored with follow-up data) and justify the conduction of studies adequately powered to detect significant differences in this endpoint, as highlighted by a cost-effectiveness analysis conducted on data from the IRCIS trial [43].
The limitations of this work can be ascribed to two macro-areas, i.e., general limitations of the MIPA study itself and limitations specifically pertaining this subgroup analysis. As for the general limitations of the MIPA study, its nonrandomized observational design remains the chief obstacle to a controlled evaluation of surgical outcomes. However, we addressed this issue with the aid of patient matching according to a large number of covariates, also employing conservative matching methods with strict criteria. While this represents a potential solution to avoid some issues of randomized controlled trials such as high costs, statistical power issues, and poor external validity and representativeness of results obtained in highly controlled settings [44, 45], we acknowledge that our analysis could not account for several other patient-specific or institutional potentially confounding factors. Of these, the most difficult to model remains the effect of the surgical habits at each institution and even of each surgeon in a given institution [46–50]. Another general limitation of the MIPA study is its wide enrolment timeframe, during which the quick expansion of the role of digital breast tomosynthesis and of MRI itself in the diagnostic setting could have created hidden imbalances between and inside subgroups.
The main specific limitation of this targeted analysis on needle biopsy–diagnosed DCIS is the fact that the MIPA study database did not collect information on DCIS grade and receptor status at CNB/VAB, acquiring these data only from surgical pathology. Had it been available, DCIS grade at CNB/VAB would have represented a covariate for matching, considering not only its prognostic implications [51] but also its specific influence on the accuracy of MRI [52] and on the interplay between preoperative MRI and surgical outcomes [10, 12, 16]. Again referring to the 2013–2018 enrolment timeframe of the MIPA study, this subgroup analysis could not account for the impact of the progressive clinical introduction of 3-T MRI systems, which are known to improve DCIS differential diagnosis and the accuracy of lesion sizing [53–55], nor for the potential competition in the preoperative setting between MRI and other contrast-enhanced imaging modalities, such as contrast-enhanced mammography [56–58].
In conclusion, this subgroup analysis of the MIPA study showed that, when surgical outcomes of women diagnosed with pure DCIS at CNB/VAB are compared in matched cohorts, the increase in the overall mastectomy rate engendered by preoperative MRI is less than half the corresponding reduction in reoperation rates.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Grimm LJ Rahbar H Abdelmalak M Hall AH Ryser MD Ductal carcinoma in situ: state-of-the-art review Radiology 202230224625510.1148/radiol.21183934931856 PMC 8805655 · doi ↗ · pubmed ↗
- 2van Seijen M Lips EH Thompson AM Ductal carcinoma in situ: to treat or not to treat, that is the question Br J Cancer 201912128529210.1038/s 41416-019-0478-631285590 PMC 6697179 · doi ↗ · pubmed ↗
- 3Solin LJ Management of ductal carcinoma in situ (DCIS) of the breast: present approaches and future directions Curr Oncol Rep 2019213310.1007/s 11912-019-0777-330834994 · doi ↗ · pubmed ↗
- 4Wright JL Rahbar H Obeng-Gyasi S Carlos R Tjoe J Wolff AC Overcoming barriers in ductal carcinoma in situ management: from overtreatment to optimal treatment J Clin Oncol 20224022523010.1200/JCO.21.0167434813345 PMC 8760161 · doi ↗ · pubmed ↗
- 5Allen LR Lago-Toro CE Hughes JH Is there a role for MRI in the preoperative assessment of patients with DCIS?Ann Surg Oncol 2010172395240010.1245/s 10434-010-1000-920217259 · doi ↗ · pubmed ↗
- 6Itakura K Lessing J Sakata T The impact of preoperative magnetic resonance imaging on surgical treatment and outcomes for ductal carcinoma in situ Clin Breast Cancer 201111333810.3816/CBC.2011.n.00621421520 PMC 4508001 · doi ↗ · pubmed ↗
- 7Davis KL Barth RJ Gui J Dann E Eisenberg B Rosenkranz K Use of MRI in preoperative planning for women with newly diagnosed DCIS: risk or benefit?Ann Surg Oncol 2012193270327410.1245/s 10434-012-2548-322911365 PMC 3809001 · doi ↗ · pubmed ↗
- 8Kropcho LC Steen ST Chung AP Sim M-S Kirsch DL Giuliano AE Preoperative breast MRI in the surgical treatment of ductal carcinoma in situ Breast J 20121815115610.1111/j.1524-4741.2011.01204.x 22211816 · doi ↗ · pubmed ↗