Rash and Fever in a Returned Traveler
Helena Kons, Elliott D. Herron, Zachary S. Pacheco, Erin F. Shufflebarger

TL;DR
A young woman who traveled to Ghana developed fever and rash, leading to a dengue diagnosis, highlighting the importance of considering tropical diseases in returning travelers.
Contribution
This case emphasizes the need for emergency physicians to consider dengue and other tropical illnesses in febrile returning travelers.
Findings
A 21-year-old female with fever and rash was diagnosed with dengue after returning from Ghana.
Physical exam findings like petechiae and rash can guide the diagnosis of dengue in travelers.
Emergency physicians should maintain a broad differential for febrile illnesses in returned travelers.
Abstract
A 21-year-old, otherwise healthy female presented to the emergency department with fever among other nonspecific symptoms after recently returning from Ghana. On physical exam, she had a characteristic upper extremity rash, and a tourniquet test revealed numerous petechiae. The diagnosis of dengue was suspected and subsequently confirmed. Dengue is one of many viral illnesses that should be considered in returning travelers presenting with fever and other nonspecific symptoms. Emergency physicians must keep a broad differential when evaluating fever in returned travelers and prioritize history and physical exam findings to help narrow the diagnosis and provide appropriate management and supportive care while awaiting further confirmatory testing.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
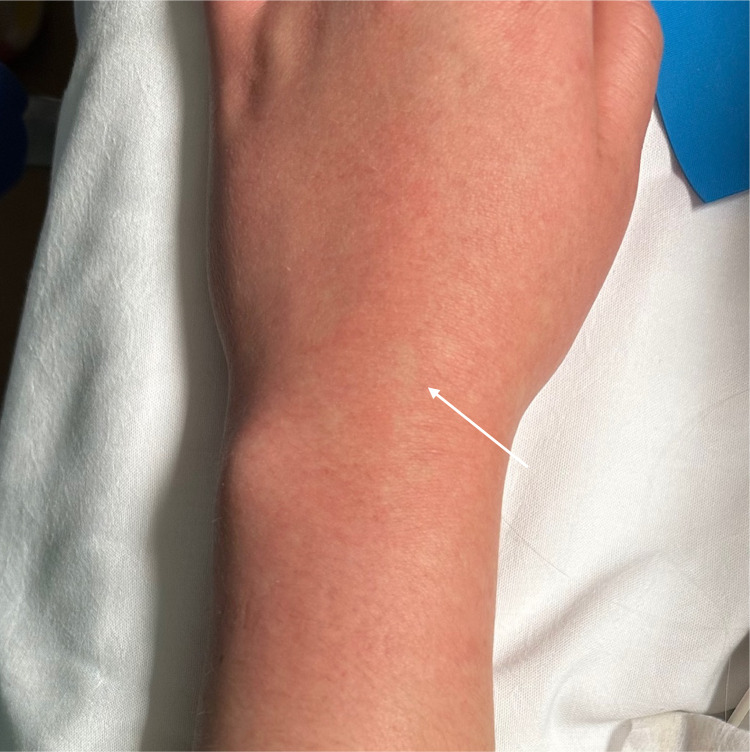 Image 1
Image 1 Image 2
Image 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTravel-related health issues · Mosquito-borne diseases and control · Viral Infections and Vectors
CASE PRESENTATION
A 21-year-old, otherwise healthy female presented to the emergency department (ED) with fever after recently returning from Ghana. She reported intermittent fever, headache with photophobia, diarrhea, joint pains, and generalized weakness. She also noticed a diffuse, intermittently pruritic rash. While in Ghana, she volunteered at a refugee hospital, ate local street food, and had exposure to local animals including dogs, sheep, and a monkey.
On arrival to the ED, she had a temperature of 39.4° Celsius and was tachycardic at 126 beats per minute. Her other vital signs were within normal limits. Physical exam revealed an uncomfortable-appearing female with a maculopapular rash to the extremities and chest, confluent erythema noted in some areas (Image 1), and scattered papules with some surrounding excoriation around the ankles, which the patient stated were mosquito bites. Initial lab results revealed mildly elevated transaminases with alanine transaminase 58 units per liter (U/L) (reference range 7–52 U/L), aspartate aminotransferase 42 U/L (12–39 U/L), thrombocytopenia with platelets 125.3 × 10^3^ per cubic millimeter (mm^3^) (150–400 × 10^3^/mm^3^), and leukopenia with white blood cells 2.78 × 10^3^/cmm (4–11 × 10^3^/mm^3^). A bedside tourniquet test1 was performed (Image 2) to assess for capillary fragility.
Rash on upper extremity with characteristic confluent erythema and small areas of spared skin (arrow).
Appreciable petechiae visible in the antecubital fossa after inflating a blood pressure cuff around the upper arm for five minutes at a pressure halfway between the patient’s systolic and diastolic blood pressure. This “tourniquet test” is deemed positive if more than 10 petechiae are present within a square inch of skin, suggesting capillary fragility.1
The patient received intravenous fluids and acetaminophen for fever and was started on empiric oral doxycycline to cover for tick-related illness prior to admission for observation. Her labs remained stable, and her symptoms, including fever, improved during her 36-hour hospital stay. Approximately one week after discharge from the hospital, both the dengue fever virus antibodies immunoglobulin G and M resulted positive.
DISCUSSION
Dengue is an acute viral febrile illness transmitted by the Aedes aegypti mosquito.2 It is endemic to Southeast Asia, Latin America, and Africa.2 Within the United States, it remains an uncommon diagnosis, with 814 documented cases reported in 2021.3 Dengue commonly presents with nonspecific symptoms including fever, headache, vomiting, transient macular rash, myalgias and arthralgias.2 This nonspecific presentation mimics other viral, bacterial, and parasitic illnesses, making it difficult to diagnose in the acute setting. For example, chikungunya symptoms can mirror those of dengue with fever, rash, and myalgias.4 Malaria is also mosquito-borne and can present with fever and thrombocytopenia.4
Focusing on specific details including region(s) visited, timing of fever relative to incubation period, exposures encountered, symptoms experienced, physical exam findings, and lab results can narrow down the pathogen.4 Detection of dengue virus antigens remains the diagnostic gold standard; however, this requires time and specialized equipment.5 Therefore, emergency physicians must keep a broad differential when evaluating fever in returned travelers and prioritize history and physical exam findings to help narrow the diagnosis and provide appropriate management while awaiting confirmatory testing.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Grande AJ Reid H Thomas E et al . Tourniquet test for dengue diagnosis: systematic review and meta-analysis of diagnostic test accuracy. P Lo S Negl Trop Dis. 2016;10(8):e 0004888.27486661 10.1371/journal.pntd.0004888 PMC 4972435 · doi ↗ · pubmed ↗
- 2World Health Organization . Dengue and severe dengue. 2023. Available at: https://www.who.int/en/news-room/fact-sheets/detail/dengue-and-severe-dengue. Accessed September 29, 2023.
- 3Centers for Disease Control and Prevention . Dengue: historic data (2010–2022). 2022. Available at: https://www.cdc.gov/dengue/statistics-maps/2020.html. Accessed August 1, 2023.
- 4Thwaites GE Day N . Approach to fever in the returning traveler. N Engl J Med. 2017;376(6):548–60.28177860 10.1056/NEJ Mra 1508435 · doi ↗ · pubmed ↗
- 5Yow KS Aik J Tan EY et al . Rapid diagnostic tests for the detection of recent dengue infections: an evaluation of six kits on clinical specimens. P Lo S One. 2021;16(4):e 0249602.33793682 10.1371/journal.pone.0249602 PMC 8016316 · doi ↗ · pubmed ↗