Left Hemifacial Spasms Due to Left Vertebrobasilar Dolichoectasia
Sanjay M Khaladkar, Prajakta P KirdatPatil, Aryaman Dhande, Neeha A Jhala, Suhas M

TL;DR
This paper describes a case where left-sided hemifacial spasms were caused by left vertebrobasilar dolichoectasia, a condition involving abnormal arterial dilation.
Contribution
The novelty lies in identifying VBD as a rare cause of HFS, supported by specific imaging findings.
Findings
Left-sided HFS was linked to left vertebrobasilar dolichoectasia.
Imaging confirmed arterial dilatation and tortuosity in the affected region.
This case highlights the importance of considering VBD in HFS diagnosis.
Abstract
Hemifacial spasm (HFS) arises from involuntary, recurrent, irregular tonic-clonic-like contractions of the muscles innervated by the facial nerve. Typically, compression of the facial nerve root exit on the same side is attributed to either a vascular loop or a mass located in the cerebellopontine (CP) angle. Dolichoectasia, alternatively termed dilated arteriopathy, is characterized by arterial dilatation, elongation, and tortuosity. Here, we present a case involving vertebrobasilar dolichoectasia (VBD) as the cause of HFS, alongside relevant imaging findings.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
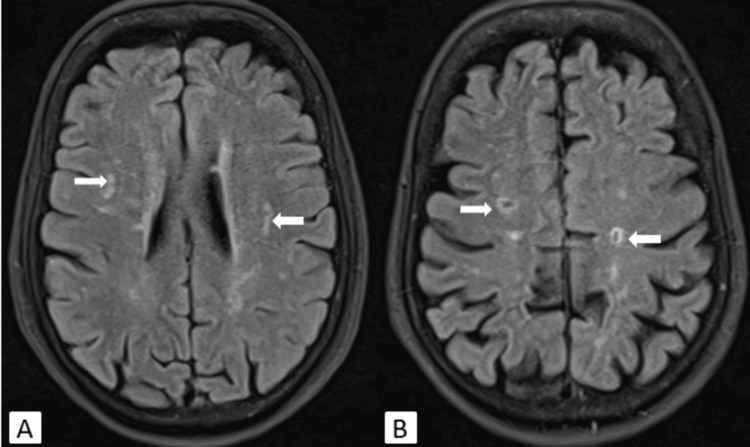 Figure 1
Figure 1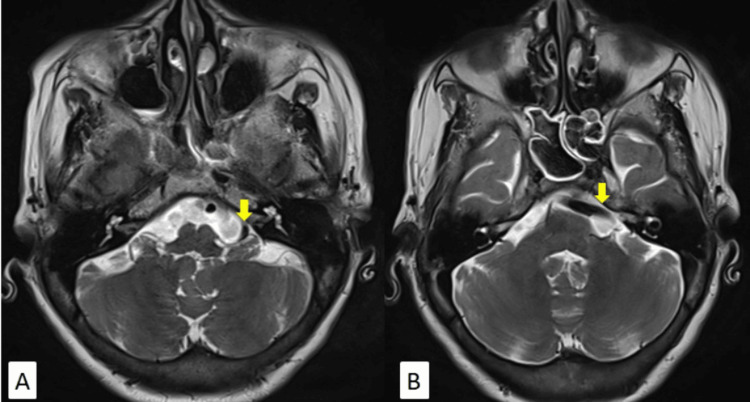 Figure 2
Figure 2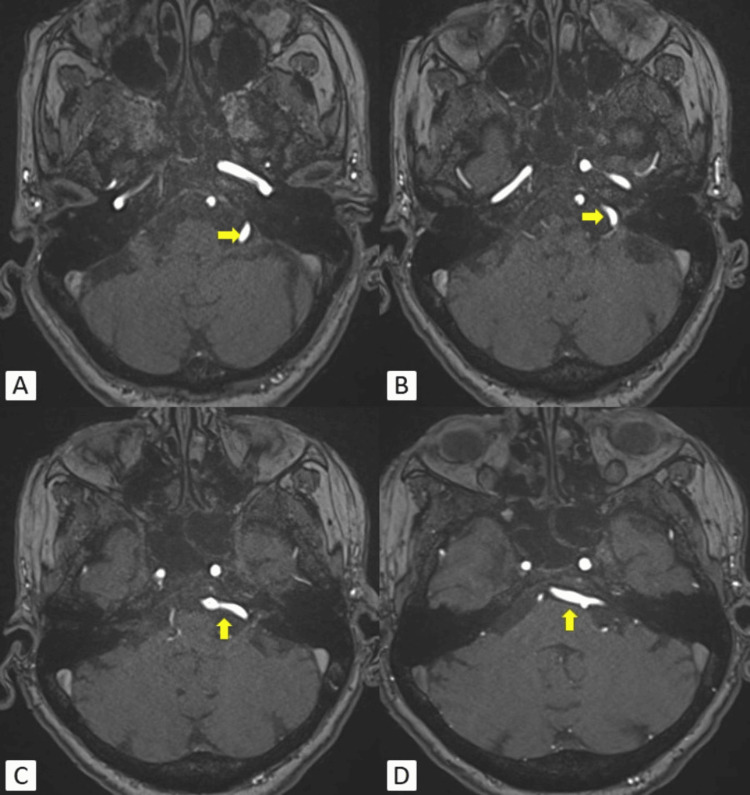 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrigeminal Neuralgia and Treatments · Intracranial Aneurysms: Treatment and Complications · Vascular Malformations Diagnosis and Treatment
Introduction
Hemifacial spasm (HFS) is characterized by involuntary, repetitive, and irregular contractions of the facial muscles innervated by the facial nerve, resulting in involuntary and painless spasms. It usually starts with spasms affecting the orbicularis oris muscle and gradually extends to affect other facial muscles. Its occurrence in the United States varies from 0.5 to 2.4 per 100,000 people [1]. Tortuous blood vessels, specifically the posterior inferior cerebellar artery (PICA) and anterior inferior cerebellar artery (AICA), are the primary culprits for the compression of the facial nerve [2]. Vertebrobasilar dolichoectasia (VBD) causing direct compression is a rare cause of facial nerve compression. The usual complications of VBD include ischemic stroke (17.6%), brainstem compression (10.3%), and transient ischemic attack (10%) [3]. Cerebral microbleeds are also commonly observed in patients with VBD.
Case presentation
A 70-year-old female presented with a left HFS persisting for the past six months. She reported no upper or lower limb weakness and no other neurological deficits. No other relevant complaints were disclosed by the patient. The patient was a known hypertensive for the past 20 years.
Magnetic resonance imaging (MRI) of the brain revealed multiple hyperintense foci in the fronto-parietal periventricular white matter and centrum semiovale region on long repetition time (TR) images and fluid-attenuated inversion recovery (FLAIR). These foci did not show diffusion restriction on diffusion-weighted imaging (DWI), indicative of chronic ischemic changes (Fazekas score 1). Old lacunar infarcts were noted in the bilateral corona radiata and centrum semiovale regions (Figure 1). No acute infarct or intracerebral hemorrhage was observed on DWI and susceptibility-weighted imaging (SWI) sequences, respectively.
MRI of the brain axial FLAIR images showing white matter ischemic changes (A) and old lacunar infarcts (B) in the bilateral periventricular white matter and centrum semiovale region (white arrows).FLAIR: fluid-attenuated inversion recovery; MRI: magnetic resonance imaging
Axial T2-weighted imaging (T2WI) showed an ectatic left vertebral artery encroaching left cerebellopontine (CP) angle cistern causing mild compression over the left VII-VIII nerve complex (Figure 2).
(A, B) MRI of the brain axial T2WI showing dolichoectasia of the left vertebral artery (yellow arrows) compressing the left VII-VIII nerve complex in the left CP angle cistern.T2WI: T2-weighted imaging; CP: cerebellopontine; MRI: magnetic resonance imaging
Magnetic resonance angiography (MRA) of the brain using 3D time of flight (TOF) revealed dolichoectasia of the left vertebral artery. It was encroaching and causing mild compression of the cisternal segment of the left VII-VIII nerve complex (Figure 3). Type 2 left AICA was also noted. The rest of the study showed normal findings.
(A-D) 3D TOF MRI of the brain angiography showing dolichoectasia of the left vertebral artery (yellow arrows) extending in the left CP angle cistern causing mild compression over the left VII-VIII nerve complex.TOF: time of flight; CP: cerebellopontine; MRI: magnetic resonance imaging
MRA of the brain maximum intensity projection (MIP) image shows dolichoectasia of the left vertebral artery extending in the left CP angle cistern (Figure 4).
MRA of the brain MIP image showing dolichoectasia of the left vertebral artery (yellow arrow) extending in the left CP angle cistern.MIP: maximum intensity projection; MRA: magnetic resonance angiography; CP: cerebellopontine
Using an insulin syringe, the patient received an injection of botulinum toxin (50 units in 1.1 ml of normal saline), which provided symptomatic relief for three months. However, during the follow-up after three months, the patient started experiencing similar symptoms and opted for Ayurvedic treatment instead.
Discussion
VBD is an intra-arterial condition characterized by the elongation and dilatation of the vertebral and basilar arteries. It can be acquired or hereditary. Risk factors for acquired intra-arterial dolichoectasia include aging, hypertension, and male gender. VBD can lead to various symptoms, such as HFS, tinnitus, and brainstem compression [4]. HFS, although rare, can be a cause of movement disorder and may induce psychological stress [5]. Therefore, accurate diagnosis and appropriate management are crucial [6]. Worldwide, its prevalence is reported to be 14.5 per 1 lakh in women and 7.4 per 1 lakh in men. Compression of the facial nerve can be attributed to tortuous arteries such as the AICA, PICA, and superior cerebellar artery (SCA) [6-8]. Direct compression by VBD is rare, with only 0.7% of cases reported in a study involving 1642 cases of HFS [9,10]. Advances in imaging techniques allow for the diagnosis of this condition by visualizing the compression of the facial nerve at its root entry zone as it emerges from the brainstem. MRI and MRA with thin T2 constructive interference in steady-state (CISS) sequences are highly effective in diagnosing this condition. When the root entry zone is compressed, it generates antidromic impulses, which lead to HFS. The result is an excitation of the face nucleus, known as a kindling phenomenon [11]. HFS caused by vascular compression by VBD presents two treatment options: botulinum toxin injection, known for its low incidence of adverse effects, which prolongs the duration of treatment for up to 20 years, and microvascular decompression. Microvascular decompression offers a definitive treatment but carries complications such as facial palsy and hearing impairment. It serves as a viable and effective option for patients previously treated with botulinum toxin. Botulinum toxin injections around the eye and cheek provide symptomatic relief with minimal side effects. However, the disadvantage lies in the need for repeated injections every few months indefinitely. On the other hand, surgical microvascular decompression offers the advantage of a permanent solution but comes with serious complications, including deafness (2.7%), facial paralysis (1.7%), cerebellar hematoma (0.5%), brainstem infarct (0.3%), and death (0.1%) [12].
Conclusions
HFS commonly arises from facial nerve root exit compression, frequently attributed to vascular loops or masses situated in the CP angle. VBD is characterized by the elongation and dilatation of the vertebral and basilar arteries, either acquired or hereditary. It can lead to various symptoms, including HFS, tinnitus, and brainstem compression. The prevalence of HFS caused by VBD is rare, but accurate diagnosis is crucial for appropriate management. Advances in imaging techniques, such as MRI and MRA with thin T2 CISS sequences, facilitate the diagnosis of VBD and its compression of the facial nerve.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hemifacial spasm caused by vertebral artery dolichoectasia Am J Ophthalmol Rahman EA Trobe JD Gebarski SS 85485613320021203669310.1016/s 0002-9394(02)01387-9 · doi ↗ · pubmed ↗
- 2Hemifacial spasm, vertebrobasilar dolichoectasia and neurofibromatosis type 1J Clin Neurosci de Pablo-Fernández E Correas-Callero E Sierra-Hidalgo F Posada IJ 104610471920122248068210.1016/j.jocn.2011.05.033 · doi ↗ · pubmed ↗
- 3Clinical course and treatment of vertebrobasilar dolichoectasia: a systematic review of the literature Neurol Res Wolters FJ Rinkel GJ Vergouwen MD 1311373520132345257510.1179/1743132812 Y.0000000149 · doi ↗ · pubmed ↗
- 4Intracranial arterial dolichoectasia Front Neurol Del Brutto VJ Ortiz JG Biller J 344820172876987210.3389/fneur.2017.00344 PMC 5511833 · doi ↗ · pubmed ↗
- 5Morphological characteristics of the vertebrobasilar artery system in patients with hemifacial spasm and measurement of bending length for evaluation of tortuosity Clin Neurol Neurosurg Ding S Yan X Guo H 10614419820203293202710.1016/j.clineuro.2020.106144 · doi ↗ · pubmed ↗
- 6Hemifacial spasm: the past, present and future J Neurol Sci Chaudhry N Srivastava A Joshi L 273135620152611143010.1016/j.jns.2015.06.032 · doi ↗ · pubmed ↗
- 7An unusual cause of hemifacial spasm Br J Neurosurg Doherty CM Briggs G Quigley DG Mc Carron MO 1071092920152505859410.3109/02688697.2014.940841 · doi ↗ · pubmed ↗
- 8Facial myokymia and hemifacial spasm in multiple sclerosis: a descriptive study on clinical features and treatment outcomes Neurologist Marin Collazo IV Tobin WO 162320182926603610.1097/NRL.0000000000000163 · doi ↗ · pubmed ↗