Myasthenia Gravis-Like Syndrome Resulting From Immune Checkpoint Inhibitors in a Patient With Urothelial Carcinoma
Alvaro J Vivas, Umar Chaudhry, Naveen Punchayil Narayanankutty, Ramon Lopez, Jorge Lamarche

TL;DR
A cancer patient developed a myasthenia gravis-like syndrome after receiving a combination of immune checkpoint inhibitors.
Contribution
Reports a novel case of severe autoimmune-like toxicity from a specific ICI combination in urothelial carcinoma.
Findings
The patient experienced severe multisystem autoimmune-like toxicity.
Myasthenia gravis-like syndrome was observed with the ICI combination therapy.
Combined immunotherapy may increase the risk of systemic and neurological autoimmunity.
Abstract
The widespread use of immune checkpoint inhibitors (ICIs) for the treatment of various types of cancer has led to increasing reports of associated adverse effects. The use of the ipilimumab/nivolumab/sacituzumab combination is currently under study in patients with metastatic urothelial carcinoma, given their potential synergism for immunogenic cell death. Information regarding the toxicity spectrum of this combination is lacking. Here, we describe a patient with urothelial carcinoma who had a severe multisystem autoimmune-like toxicity and myasthenia gravis-like syndrome in response to the ipilimumab/nivolumab/sacituzumab combination therapy. We also briefly describe the literature regarding the association between combined immunotherapy use and systemic and neurological autoimmunity.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
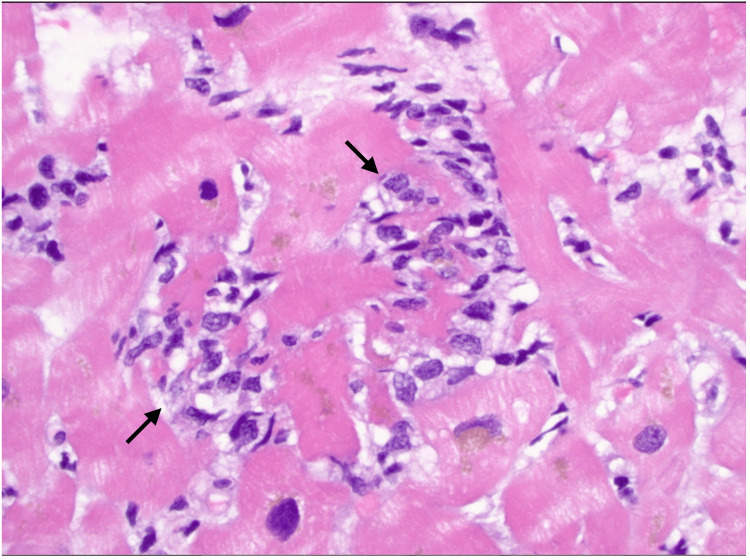 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMyasthenia Gravis and Thymoma · Cancer Immunotherapy and Biomarkers · Neuroendocrine Tumor Research Advances
Introduction
Immune checkpoint inhibitors (ICIs) are immunomodulatory antibodies that enhance anticancer immune response [1]. They target immunologic receptors on the surface of T lymphocytes [1]. Some of the primary targets include programmed cell death receptor 1 (PD-1), and cytotoxic T lymphocyte-associated antigen 4 (CTLA-4). Examples of antibodies targeting PD-1 include nivolumab, pembrolizumab, and cemiplimab. On the other hand, ipilimumab and tremelimumab target CTLA-4. During the last decade, immunotherapy has been approved for a wider range of malignancies, including different solid tumors [2]. Immune-related adverse effects (irAEs) are a mosaic of inflammatory responses that can involve different organs [3]. Rarely, immune-related neurological cases of toxicities can occur [4]. Sacituzumab govitecan is a monoclonal antibody composed of anti-trophoblast cell-surface antigen 2 (Trop-2). Several trials are exploring its activity in different malignancies (NCT04468061, NCT04448886, NCT05675579). Currently the ipilimumab/nivolumab/sacituzumab combination is under study, with promising results (NCT04863885). We describe the case of a urothelial carcinoma male patient who experienced a severe inflammatory response and myasthenia gravis-like syndrome after receiving ipilimumab plus nivolumab combined with sacituzumab.
Case presentation
A 74-year-old patient with a past medical history of chronic kidney disease (CKD) stage three and urothelial carcinoma treated with cisplatin and radical prostatectomy 18 months prior presented to the hospital with a recurrence of his malignancy. He was cisplatin-ineligible due to decreased glomerular function rate (GFR). Therapy with ipilimumab, nivolumab, and sacituzumab was initiated. After three weeks of treatment, the patient presented with complaints of fatigue, muscle aches, nausea, double vision, and loose stools. On physical exam, he was hemodynamically stable, with bilateral diplopia and loss of visual acuity. The rest of the neurological exam was normal except for decreased bilateral hip flexor strength (+/+++++). The patient subsequently went into respiratory failure requiring intubation. Electrocardiogram showed a complete heart block, with a heart rate of 40 beats per minute. Suspicion for respiratory decompensation secondary to myasthenia gravis was considered.
On blood work myositis antibodies and acetylcholine receptor-binding antibodies were negative. Other pertinent labs included elevated serum creatinine of 1.9 mg/dL (baseline was 1.5 mg/dL) and creatine kinase of 16,000 units/L. Urinalysis showed mild proteinuria and pyuria. Troponin I (high sensitivity) was 13,441 ng/L, alanine aminotransferase (ALT) was 288 units/L, and aspartate aminotransferase (AST) was 218 units/L. The patient underwent cardiac catheterization that showed multivessel coronary artery occlusion with 70% left main coronary artery ostial disease. A temporary pacer was inserted. There was a concern for myocarditis, and the patient was started on methylprednisolone, belatacept, mycophenolate mofetil, and vasopressors. Endomyocardial biopsy revealed predominantly lymphohistiocytic inflammatory infiltrates suggestive of myocarditis (Figure 1).
Lymphohistiocytic inflammatory infiltrates among cardiomyocytes
Intravenous immunoglobulin (IVIG) was considered as a therapeutic option. However, the patient requested to be extubated and placed on comfort measures only. The patient passed away with his family at the bedside.
Discussion
ICIs are relatively novel therapeutic options for different malignancies, with growing evidence for solid tumors [5]. The nivolumab plus ipilimumab combination has been shown to be an effective treatment for urothelial carcinoma [6]. Systemic irAEs with the use of ipilimumab, nivolimumab, or their combination can occur. Reported phenomena include inflammatory skin reactions, diarrhea, colitis, and endocrinopathies [7]. Immune-related neurological adverse effects occur in up to 14% of patients [8]; these include Guillain-Barré syndrome, limbic encephalitis, transverse myelitis, and myasthenia gravis-like syndrome. The latter is very infrequent, with around 50 de novo cases described in the literature [9]. The incidence is higher in patients with combined CTLA-4 and PD-1 inhibition [8].
Sacituzumab govitecan is a monoclonal antibody composed of Trop-2. It has been shown to be superior (longer progression-free survival) than a single-agent chemotherapy among patients with metastatic triple-negative breast cancer [10]. Several trials are exploring its activity in different malignancies (NCT04468061, NCT04448886, NCT05675579). Currently, the ipilimumab/nivolumab/sacituzumab combination is under study, with promising results (NCT04863885). The most common adverse effects described for sacituzumab include nausea, diarrhea, fatigue, and neutropenia [11]. The evidence regarding its immune-related or neurological side effects is scarce, with some reported descriptions of induced speech disorder, muscle atrophy, hepatic failure, and myocardial infarction [12]. However, the consequences of using nivolumab plus ipilimumab combined with sacituzumab regarding adverse effects are unknown.
Here, we describe a rare case of the ipilimumab/nivolumab/sacituzumab combination-induced myasthenia gravis-like syndrome plus severe multisystem autoimmune-like toxicity. In a systematic review of the literature, 58 de novo cases of immunotherapy-induced myasthenia gravis-like syndrome were identified, of which 37% experienced concurrent myositis [9]. Our patient presented with myositis, myocarditis, and myasthenia gravis-like syndrome, a triad that has been named “3M triad.” Patients presenting with this triad have a particularly high mortality, up to 60% [13]. Despite negative myositis-specific antibodies and acetylcholine receptor antibodies, myasthenia gravis-like syndrome and myositis could not be excluded considering immunotherapy-related seronegative cases have been described [4]. Myocarditis was corroborated on histopathological findings.
In addition, our patient presented with a particularly severe multisystemic response, including acute kidney injury, elevation in aminotransferases, and cardiogenic shock. The latter was caused due to both a complete heart block and a myocardial infarction. The estimated prevalence of immunotherapy-associated cardiotoxicity is around 2%, of which 7% comprise conduction disorders. Myocarditis has the highest mortality rates of all irAEs, up to 50% [14].
Different mechanisms have been postulated regarding how ICIs induce irAEs. These include local reduction of T-reg cells, loss of peripheral tolerance, and the release of potential antigens from the tumor that resemble normal tissue (e.g., cardiac muscle) [14]. Risk factors include genetic predisposition, pre-existing autoimmune disease, duration of therapy, and combined checkpoint blockade [15].
Combining nivolimumab with ipilimumab is associated with higher incidence of irAEs [8]. The risk of this therapy combined with sacitizumab remains largely unknown, as sacituzumab is currently an experimental therapy. Treatment strategies for irAEs include the interruption of ICIs, use of corticosteroids, IVIG, and plasma exchange [16]. IVIG was considered for our patient; however, he elected to go for comfort care.
Conclusions
This case describes the potential of severe adverse effects for the ipilimumab/nivolumab/sacituzumab combination treatment. Early recognition of these manifestations is important to reduce the probability of complications and mortality. Thorough discussion with the patient considering risks and benefits should always be considered.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Immune checkpoint inhibitors in cancer therapy Curr Oncol Shiravand Y Khodadadi F Amin Kashani S 304430602920223562163710.3390/curroncol 29050247 PMC 9139602 · doi ↗ · pubmed ↗
- 2Increasing cure rates of solid tumors by immune checkpoint inhibitors Exp Hematol Oncol Ma W Xue R Zhu Z 101220233664716910.1186/s 40164-023-00372-8PMC 9843946 · doi ↗ · pubmed ↗
- 3Immune-related adverse events of immune checkpoint inhibitors: a review Front Immunol Yin Q Wu L Han L 11679751420233730430610.3389/fimmu.2023.1167975 PMC 10247998 · doi ↗ · pubmed ↗
- 4Immune checkpoint inhibitor-induced myasthenia gravis Front Neurol Huang YT Chen YP Lin WC Su WC Sun YT 11202010.3389/fneur.2020.00634 PMC 737837632765397 · doi ↗ · pubmed ↗
- 5Assessing the future of solid tumor immunotherapy Biomedicines Guha P Heatherton KR O'Connell KP Alexander IS Katz SC 6551020223532745610.3390/biomedicines 10030655 PMC 8945484 · doi ↗ · pubmed ↗
- 6Nivolumab alone and with ipilimumab in previously treated metastatic urothelial carcinoma: Check Mate 032 nivolumab 1 mg/kg plus ipilimumab 3 mg/kg expansion cohort results J Clin Oncol Sharma P Siefker-Radtke A de Braud F 160816163720193110003810.1200/JCO.19.00538 PMC 6879315 · doi ↗ · pubmed ↗
- 7Ipilimumab and its toxicities: a multidisciplinary approach Oncologist Fecher LA Agarwala SS Hodi FS Weber JS 7337431820132377482710.1634/theoncologist.2012-0483 PMC 4063401 · doi ↗ · pubmed ↗
- 8Neurologic autoimmunity and immune checkpoint inhibitors: autoantibody profiles and outcomes Neurology Sechi E Markovic SN Mc Keon A 05295202010.1212/WNL.0000000000010632 PMC 768291132796130 · doi ↗ · pubmed ↗