Central Pontine Myelinolysis: A Rare and Life-Threatening Adverse Effect of Clobazam and Quetiapine
Gautam N Bedi, Sourya Acharya, Sunil Kumar, Smruti A Mapari, Rucha Sawant

TL;DR
A rare neurological condition called central pontine myelinolysis was linked to two medications in a patient without electrolyte issues.
Contribution
This case highlights that clobazam and quetiapine can cause CPM even without hyponatremia.
Findings
MRI confirmed central pontine myelinolysis in a patient on clobazam and quetiapine.
Discontinuation of the medications led to clinical improvement.
The case suggests medication-induced CPM can occur without electrolyte abnormalities.
Abstract
Central pontine myelinolysis (CPM) is a rare neurological disorder characterized by demyelination within the central portion of the pons. While hyponatremia is a well-known precipitating factor, other etiologies, including medication use, have been reported. We present a case of a 69-year-old male with a history of obsessive-compulsive disorder, stroke, and type 2 diabetes mellitus who developed confusion, altered sensorium, and weakness in all four limbs. An MRI brain imaging revealed characteristic findings suggestive of CPM. Despite normal serum sodium levels, discontinuation of clobazam and quetiapine, medications taken by the patient, led to clinical improvement. This case underscores the importance of considering medication-induced CPM in the differential diagnosis of patients presenting with neurological symptoms, even in the absence of electrolyte abnormalities.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
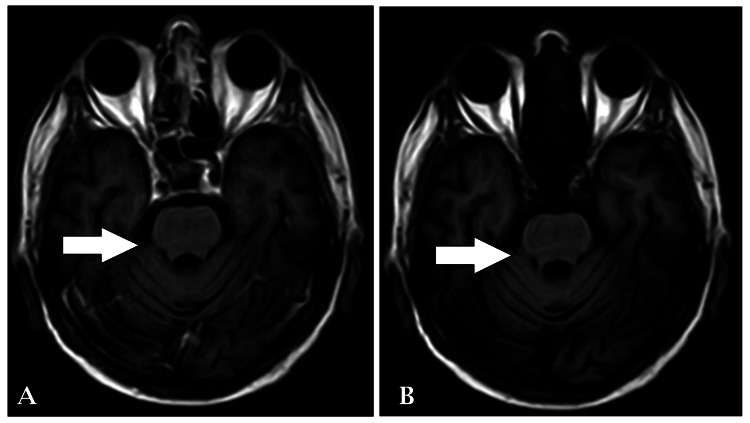 Figure 1
Figure 1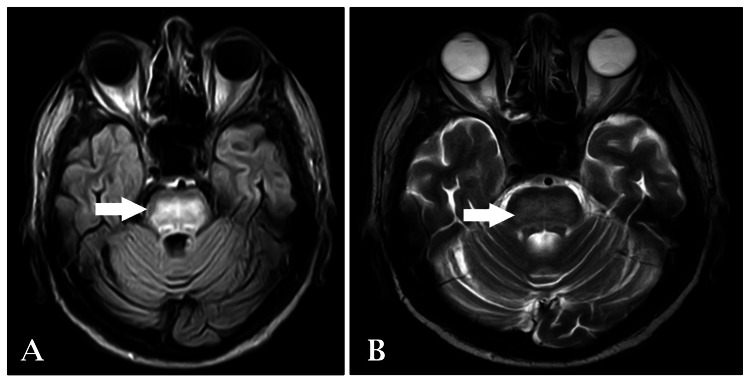 Figure 2
Figure 2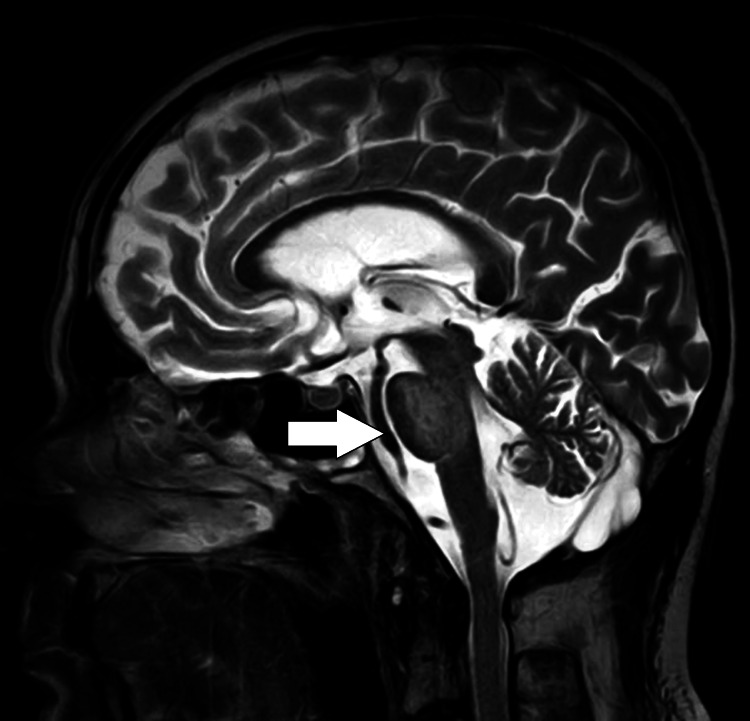 Figure 3
Figure 3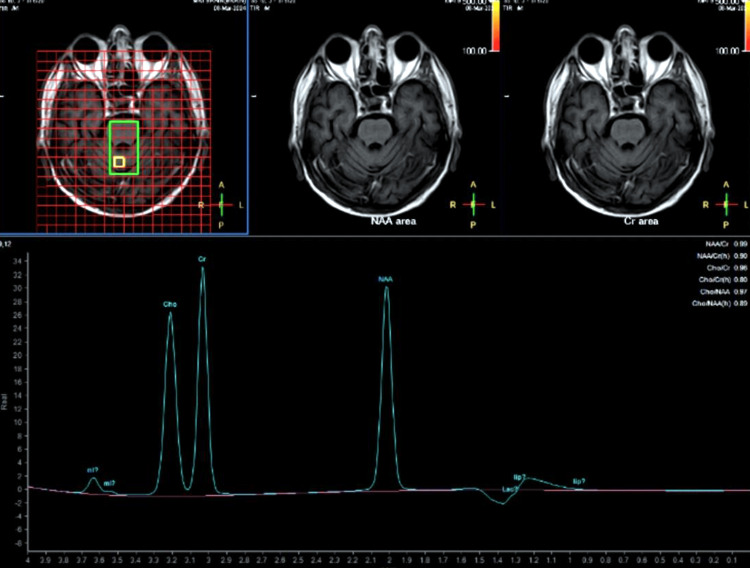 Figure 4
Figure 4| Investigations | Reference range | Value on admission | Value on discharge |
| Serum sodium (mmol/L) | 135-147 | 142 | 140 |
| Serum potassium (mmol/L) | 3.5-5.1 | 4.29 | 4.5 |
| Serum calcium (mg/dL) | 4.5-5.6 | 4.24 | 4.3 |
| Urine sodium (mmol/L) | 75-200 | 154 | 160 |
| Urine potassium (mmol/L) | 10-20 | 16 | 18 |
| Urine calcium (mg/dL) | 4.6-5.3 | 4.8 | 5.2 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsElectrolyte and hormonal disorders · Infectious Encephalopathies and Encephalitis · Bipolar Disorder and Treatment
Introduction
Central pontine myelinolysis (CPM) is a rare neurological disorder characterized by demyelination within the central portion of the pons, often resulting in severe neurological deficits. Originally described by Adams et al. in 1959, CPM was primarily associated with rapid correction of hyponatremia, particularly in the setting of chronic alcoholism or liver transplantation [1]. However, it has become increasingly recognized that CPM can also occur in the absence of significant electrolyte disturbances, particularly in patients with predisposing factors such as alcoholism, liver disease, malnutrition, and certain medications [2]. One such medication implicated in the development of CPM is clobazam, a benzodiazepine derivative commonly used in the management of various neurological and psychiatric disorders, including epilepsy and anxiety disorders. While clobazam is generally well-tolerated, there have been reported cases of CPM associated with its use, particularly in patients with underlying risk factors such as electrolyte imbalances or liver dysfunction [3].
Similarly, quetiapine, an atypical antipsychotic agent widely prescribed for the treatment of schizophrenia, bipolar disorder, and major depressive disorder, has also been linked to the development of CPM. Although the exact mechanisms underlying quetiapine-induced CPM remain unclear, it is hypothesized that its anticholinergic effects and potential for causing electrolyte disturbances may contribute to myelinolysis in susceptible individuals [4]. Given the increasing recognition of medication-induced CPM, clinicians must remain vigilant for neurological symptoms in patients receiving these medications, particularly those with underlying risk factors. Prompt recognition and cessation of the offending agents and supportive management are essential in preventing further neurological deterioration and optimizing patient outcomes.
Case presentation
A 69-year-old male presented to the emergency department with chief complaints of confusion, altered sensorium, and weakness in all four limbs, persisting for six hours. His medical history revealed a diagnosis of obsessive-compulsive disorder over the past three months, managed with a stable regimen of clobazam 10 mg twice daily and quetiapine 50 mg once daily. Additionally, he had a known history of stroke and type 2 diabetes mellitus, for which he was prescribed voglibose GM3 twice daily. Random blood sugar levels obtained in the emergency department were 110 mg/dL, falling within the normal range. There was no recent history of illness, head trauma, or significant electrolyte abnormalities reported.
Upon physical examination, the patient appeared drowsy. Vital signs revealed a heart rate of 88 beats per minute, blood pressure of 120/80 mmHg, and oxygen saturation of 99% on room air. Neurological examination showed normal tone with 4/5 power in both lower limbs and bilateral plantar flexor response.
The patient's medications, clobazam and quetiapine, were considered potential contributors to the development of CPM. Consequently, both medications were promptly discontinued. Blood investigations were ordered, and the results are outlined in Table 1.
An MRI brain imaging contrast with spectroscopy revealed a non-enhancing altered signal intensity noted in the pons, extending to both sides of the midline. The lesion appeared isointense in T1-weighted images (Figure 1) and hyperintense in T2-weighted/fluid-attenuated inversion-recovery (FLAIR) images (Figures 2-3), with no restriction on diffusion-weighted imaging (DWI) and high signal on apparent diffusion coefficient (ADC), suggestive of osmotic demyelination. Age-related atrophic changes were noted in various brain structures, along with small vessel ischemic changes observed in bilateral subcortical and periventricular deep white matter.
T1WI and T1+C axial section of brain showing non-enhancing lesion in ponsT1WI: T1-weighted imaging; T1+C: T1-weighted imaging with contrast
T2-weighted and FLAIR axial section of brain showing hyperintense lesion in pons extending to both sides of the midlineFLAIR: fluid-attenuated inversion-recovery
T2WI sagittal section of brain showing hyperintense lesion in ponsT2WI: T2-weighted imaging
The spectroscopy showed elevated N-acetyl aspartate (NAA) and creatinine (Cr) peak levels with a decreased NAA/Cr ratio (0.99) (Figure 4).
Magnetic resonance spectroscopy showing the raised NAA peak and Cr peak with decreased NAA/Cr ratio (0.99)NAA: N-acetyl aspartate; Cr: creatinine
Serum sodium levels, as well as urinary sodium and potassium levels, were within normal limits. This effectively ruled out the possibility of the syndrome of inappropriate secretion of antidiuretic hormone (SIADH). Despite diabetes mellitus being a triggering factor for CPM, the patient's diabetes was well-controlled, leading to the conclusion of a direct association between clobazam and quetiapine and the development of CPM.
The treatment focused on providing symptomatic relief and supportive management, including antibiotics, analgesics, antacids, antiemetics, antidiabetic medications, and hydration and electrolyte monitoring. Alternative antipsychotic agents with a lower propensity for metabolic side effects were considered. The patient's care involved multiple specialties utilizing a multidisciplinary approach, leading to a positive response to treatment.
Discussion
CPM is a rare and potentially life-threatening neurological disorder characterized by demyelination within the central portion of pons. It typically presents with a spectrum of neurological symptoms, including confusion, altered sensorium, and weakness, as observed in our patient [5]. While the exact pathogenesis of CPM remains incompletely understood, it is commonly associated with rapid correction of hyponatremia, particularly in patients with chronic alcoholism, liver disease, or malnutrition [2]. In our case, the patient developed CPM despite normal serum sodium levels and the absence of electrolyte abnormalities. This is consistent with reports in the literature suggesting that other factors, such as medication use, may contribute to the development of CPM [6]. Indeed, both clobazam and quetiapine, medications taken by our patient, have been implicated in the pathogenesis of CPM [7,8].
Clobazam is a benzodiazepine commonly used in the management of various neurological disorders, including epilepsy and anxiety disorders. While it is generally well-tolerated, there have been reports linking clobazam use with the development of CPM, particularly in elderly patients or those with underlying risk factors [7]. Similarly, quetiapine, an atypical antipsychotic agent, has been associated with CPM in several case reports [8]. The mechanism by which these medications contribute to the development of CPM is not fully elucidated. However, it is speculated that they may disrupt the osmotic balance within the brain, leading to cellular swelling and subsequent demyelination [9]. Additionally, patients with pre-existing neurological conditions, such as stroke, as seen in our patient, may be at increased risk of developing CPM when exposed to these medications [10].
The diagnosis of CPM in our patient was supported by characteristic findings on MRI brain imaging, including hyperintensity on T2-weighted/FLAIR images and the absence of diffusion restriction on DWI. Furthermore, spectroscopy revealed biochemical alterations consistent with demyelination, further supporting the diagnosis [11]. CPM management primarily involves discontinuing the offending agent and supportive care to alleviate symptoms. In our case, the cessation of clobazam and quetiapine was promptly initiated, leading to clinical improvement. Supportive measures were also provided, including hydration, electrolyte monitoring, and symptomatic relief.
Conclusions
In conclusion, our case highlights the importance of considering medication-induced CPM as a potential complication in patients presenting with neurological symptoms, even in the absence of classical risk factors such as hyponatremia. The prompt recognition of CPM and discontinuation of the offending medications, clobazam and quetiapine in this instance, are paramount to prevent further neurological deterioration. While the pathogenesis of medication-induced CPM remains incompletely understood, it underscores the need for heightened vigilance among clinicians prescribing medications with potential neurotoxic effects, particularly in patients with underlying neurological comorbidities. Additionally, our case underscores the value of a multidisciplinary approach to patient care involving various specialties to ensure comprehensive management and favorable outcomes. Further research is warranted to elucidate the mechanisms underlying medication-induced CPM and to develop strategies for its prevention and management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Central pontine myelinolysis: a hitherto undescribed disease occurring in alcoholic and malnourished patients AMA Arch Neurol Psychiatry Adams RD Victor M Mancall EL 154172811959 https://pubmed.ncbi.nlm.nih.gov/13616772/13616772 · pubmed ↗
- 2Central pontine and extrapontine myelinolysis: the osmotic demyelination syndromes J Neurol Neurosurg Psychiatry Martin RJ 22287520041531604110.1136/jnnp.2004.045906 PMC 1765665 · doi ↗ · pubmed ↗
- 3Immunoglobulins are effective in pontine myelinolysis Clin Neuropharmacol Finsterer J Engelmayer E Trnka E Stiskal M 1101132320001080380210.1097/00002826-200003000-00009 · doi ↗ · pubmed ↗
- 4Quetiapine, Q Tc interval prolongation, and torsade de pointes: a review of case reports Ther Adv Psychopharmacol Hasnain M Vieweg WV Howland RH 130138420142505734610.1177/2045125313510194 PMC 4107702 · doi ↗ · pubmed ↗
- 5Central pontine myelinolysis in a case of alcohol dependence syndrome Ind Psychiatry J Chatterjee K Fernandes AB Goyal S Shanker S 1982012420152721282910.4103/0972-6748.181732 PMC 4866352 · doi ↗ · pubmed ↗
- 6Central pontine and extrapontine myelinolysis: a systematic review Eur J Neurol Singh TD Fugate JE Rabinstein AA 144314502120142522087810.1111/ene.12571 · doi ↗ · pubmed ↗
- 7Osmotic demyelination syndrome Am J Med Sci King JD Rosner MH 56156733920102045363310.1097/MAJ.0b 013e 3181 d 3cd 78 · doi ↗ · pubmed ↗
- 8Central pontine myelinolysis Stat Pearls [Internet] Danyalian A Heller D Treasure Island (FL)Stat Pearls Publishing 2024 https://www.ncbi.nlm.nih.gov/books/NBK 551697/31869161 · pubmed ↗