Simultaneous bilateral reintervention using one-step endoscopic ultrasound-guided biliary drainage for severe acute cholangitis caused by malignant hilar biliary obstruction
Takeshi Ogura, Atsushi Okuda, Saori Ueno, Nobu Nishioka, Hiroki Nishikawa

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
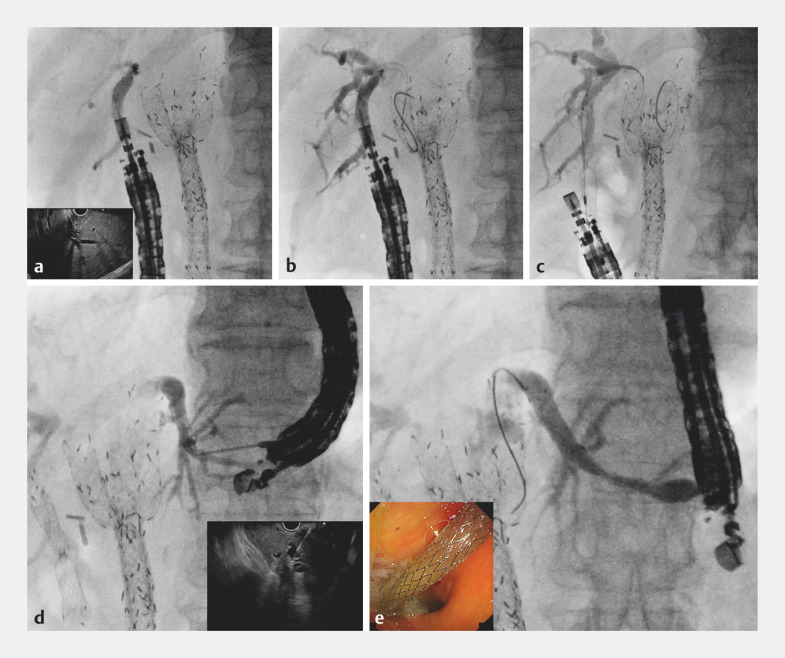 Fig. 1
Fig. 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pediatric Hepatobiliary Diseases and Treatments · Cholangiocarcinoma and Gallbladder Cancer Studies
Endoscopic retrograde cholangiopancreatography (ERCP) is a standard technique for endoscopic biliary drainage in malignant hilar biliary obstruction (MHBO). In cases of unresectable MHBO, the deployment of bilateral self-expandable metal stents (SEMSs) may be indicated 1 2 . However, with the recent development of systemic chemotherapy 3 and local tumor treatment by endoscopic radiofrequency ablation, the frequency of reintervention for stent dysfunction may increase and reintervention after bilateral SEMS deployment may be challenging. If reintervention under ERCP guidance is needed, percutaneous transhepatic biliary drainage (PTBD) is considered. As with other biliary drainage techniques, endoscopic ultrasound (EUS)-guided hepaticogastrostomy (HGS) and hepaticoduodenostomy (HDS) can be considered bilateral reintervention techniques 4 5 .
If patients have severe acute cholangitis, both biliary drainage techniques are rapidly needed. Furthermore, in acute cholangitis, there can be leakage of infected bile after tract dilation. Therefore, a one-step technique such as stent deployment without tract dilation may be helpful in preventing adverse events. If bilateral drainage is needed, the one-step technique is also preferable from the perspective of shorter procedure time. Recently, a novel partially covered SEMS with a fine-gauge stent delivery system (7 Fr; BileRush Advance, Piolax Medical, Kanagawa, Japan) has become available. This stent might be useful for one-step EUS-guided biliary drainage (EUS-BD). A case of simultaneous bilateral reintervention using one-step EUS-HGS and EUS-HDS for severe acute cholangitis due to MHBO is described.
An 89-year-old man underwent bilateral SEMS deployment for unresectable MHBO, and subsequently underwent several reinterventions for stent dysfunction. The patient was admitted with severe acute cholangitis caused by stent obstruction. Because of previous failed reintervention under ERCP guidance, EUS-BD was attempted. If EUS-HGS had been performed first, stent dislocation could have occurred during scope insertion into the duodenum and therefore EUS-HDS was attempted first. When detecting the right hepatic bile duct, it is important to prevent duodenal perforation, so the scope position was adjusted using fluoroscopic guidance. The posterior bile duct was punctured using a 19G needle and contrast medium was injected ( Fig. 1 a ). A 0.025-inch guidewire was deployed ( Fig. 1 b ). Insertion of the stent delivery system was attempted without tract dilation, and the stent was successfully deployed from the posterior bile duct to the stomach ( Fig. 1 c ). The echoendoscope was then pulled back into the stomach and the left intrahepatic bile duct was identified. After bile duct puncture had been performed with a 19G needle, cholangiography was performed with injection of contrast medium ( Fig. 1 d ). After guidewire deployment, stent deployment from the intrahepatic bile duct to the stomach was successfully performed without tract dilation ( Fig. 1 e , Video 1 ). The patient’s cholangitis was completely resolved by these drainage procedures without any adverse events being noted.
Fluoroscopic images showing: a injection of contrast medium after puncture of the posterior bile duct using a 19G needle (inset, endoscopic ultrasound [EUS] image); b deployment of a 0.025-inch guidewire; c successful deployment of a novel metal stent with a fine-gauge stent delivery system without tract dilation; d injection of contrast medium after puncture of the left intrahepatic bile duct using a 19G needle (inset, EUS image); e successful deployment of a novel metal stent with a fine-gauge stent delivery system without tract dilation (inset, endoscopic appearance of the stent).
Simultaneous bilateral reintervention is performed using a one-step technique under endoscopic ultrasound guidance with placement of novel metal stents that have a fine-gauge stent delivery system.Video 1
In conclusion, simultaneous bilateral reintervention using one-step EUS-HDS and EUS-HGS may be feasible and safe for such patients.
Endoscopy_UCTN_Code_TTT_1AS_2AH
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dumonceau JM Tringali A Papanikolaou IS Endoscopic biliary stenting: indications, choice of stents, and results: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline – Updated October 2017 Endoscopy 20185091093010.1055/a-0659-986430086596 · doi ↗ · pubmed ↗
- 2Lee TH Kim TH Moon JH Bilateral versus unilateral placement of metal stents for inoperable high-grade malignant hilar biliary strictures: a multicenter, prospective, randomized study (with video)Gastrointest Endosc 20178681782728479493 10.1016/j.gie.2017.04.037 · doi ↗ · pubmed ↗
- 3Kelley RK Ueno M Yoo C Pembrolizumab in combination with gemcitabine and cisplatin compared with gemcitabine and cisplatin alone for patients with advanced biliary tract cancer (KEYNOTE-966): a randomised, double-blind, placebo-controlled, phase 3 trial Lancet 20234011853186537075781 10.1016/S 0140-6736(23)00727-4 · doi ↗ · pubmed ↗
- 4Ogura T Onda S Takagi W Clinical utility of endoscopic ultrasound-guided biliary drainage as a rescue of re-intervention procedure for high-grade hilar stricture J Gastroenterol Hepatol 20173216316810.1111/jgh.1343727161286 · doi ↗ · pubmed ↗
- 5Minaga K Takenaka M Kitano M Rescue EUS-guided intrahepatic biliary drainage for malignant hilar biliary stricture after failed transpapillary re-intervention Surg Endosc 2017314764477210.1007/s 00464-017-5553-628424912 · doi ↗ · pubmed ↗