Endoscopic recanalization of a completely obstructed colorectal anastomosis using magnets
Willian F. Igi, Isabela Andrina Ribeiro da Silva

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
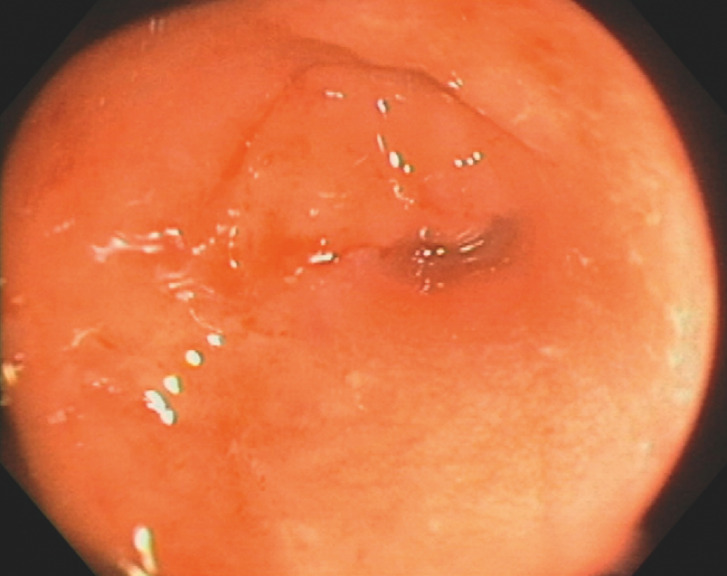 Fig. 1
Fig. 1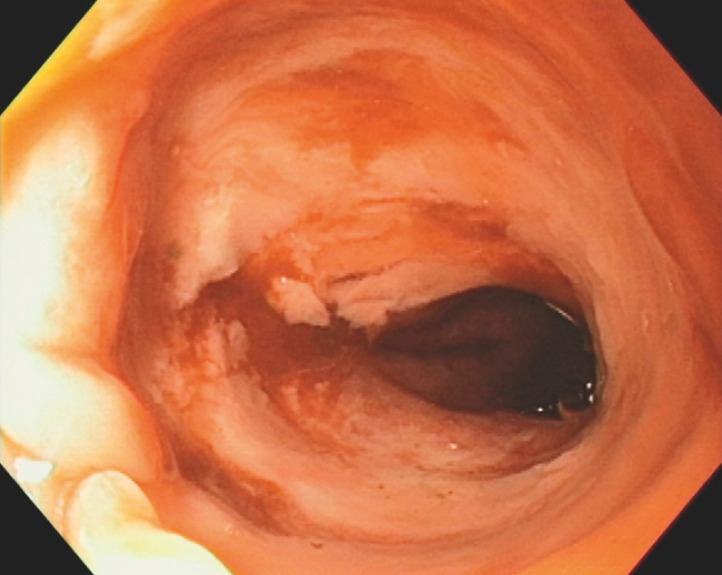 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHuman Rights and Immigration · Labor Law and Work Dynamics · Employment, Labor, and Gender Studies
A male patient who had undergone emergency loop colostomy because of intestinal obstruction secondary to a sigmoid colon tumor subsequently underwent elective rectosigmoidectomy. Endoscopy prior to bowel reconstruction revealed complete stenosis of the colorectal anastomosis ( Fig. 1 ). A previous attempt at recanalization using a needle-knife was aborted due to perforation. Following a multidisciplinary discussion, the decision was made to perform magnetic compression anastomosis.
Endoscopic view of oral aspect of completely obstructed colorectal anastomosis, following emergency loop colostomy and subsequent rectsigmoidectomy.
Two 10 × 5-mm neodymium magnets were inserted endoscopically through the efferent loop and rectum and positioned on the oral and rectal sides of the completely obstructed anastomosis. After 4 days, a follow-up colonoscopy revealed recanalization of the stenosis ( Fig. 2 , Video 1 ). Additionally, balloon dilation using a 15-mm-diameter hydrostatic balloon was performed to achieve an optimal caliber. The patient underwent bowel transit reconstruction after 6 months and remained asymptomatic at the 1-year follow up.
Colonoscopic appearance of the colorectal anastomosis recanalized using magnetic compression.
Endoscopic recanalization using two magnets positioned on the oral and rectal sides of the obstructed anastomosis in a male patient with intestinal obstruction secondary to a sigmoid colon tumor.Video 1
Magnetic compression anastomosis is widely performed in the biliary tract and esophagus but is still in the developmental stage for the gastrointestinal segment. A previous case series indicated its safety and effectiveness 1 . Case reports have described colorectal anastomosis recanalization through techniques such as stricturotomy 2 or in combination with endoscopic ultrasound 3 . Nevertheless, when access to both sides of the obstructed anastomosis is possible, the use of magnets emerges as a technically easier alternative.
Endoscopy_UCTN_Code_TTT_1AQ_2AF
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kamada T Ohdaira H Takeuchi H New technique for magnetic compression anastomosis without incision for gastrointestinal obstruction J Am Coll Surg 20212321701770033190786 10.1016/j.jamcollsurg.2020.10.012 · doi ↗ · pubmed ↗
- 2Lin D Liu W Chen Z Endoscopic stricturotomy for patients with postoperative benign anastomotic stricture for colorectal cancer Dis Colon Rectum 20226559059834775404 10.1097/DCR.0000000000001944 · doi ↗ · pubmed ↗
- 3Ni J Zhang L Mao Y Endoscopic recanalization of complete fibrotic colorectal anastomosis using an endoscopic ultrasound-guided hybrid approach Endoscopy 202456 E 43E 4410.1055/a-2216-104238232768 PMC 10794084 · doi ↗ · pubmed ↗