Balanced chaos: a 55-year journey with unrepaired D-transposition of great arteries, ventricular septal defect, and subvalvular and valvular pulmonary stenosis
Samah El-Mhadi, Hind Hibatouallah, Zakia Touati, Mohammed Cherti

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
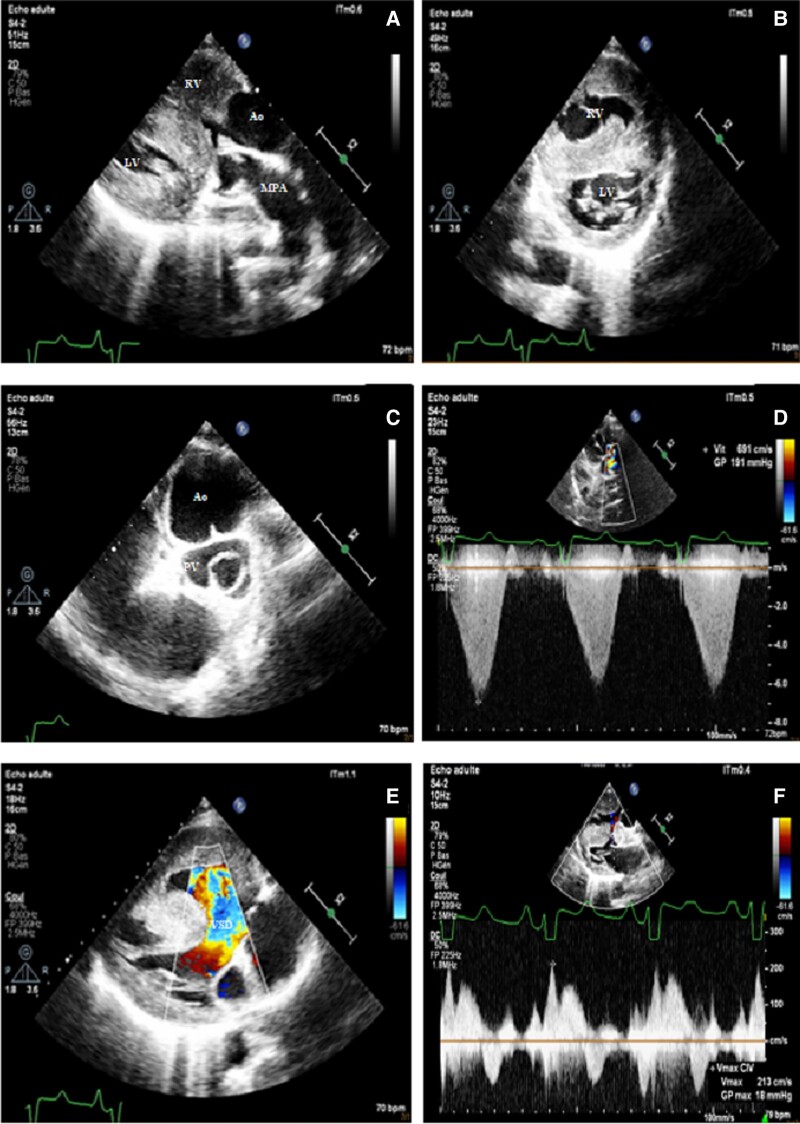 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Cardiac Valve Diseases and Treatments · Cardiovascular Function and Risk Factors
We report a case of a 55-year-old homeless patient with congenital heart disease (CHD) who lacked prior cardiac monitoring due to his precarious lifestyle.
He presented with worsening exertional dyspnoea, and on admission, had a blood pressure of 130/80 mmHg and heart rate of 70 b.p.m. Physical examination revealed digital clubbing, generalized cyanosis, and peripheral oxygen saturation of 85%. A holosystolic murmur was detected in the precordial area. ECG demonstrated sinus rhythm at 70 b.p.m. with evidence of bi-atrial and bi-ventricular hypertrophy.
Transthoracic echocardiography revealed D-transposition of the great arteries (d-TGA) (Figure 1A), with large and non-restrictive outlet ventricular septal defect causing left-to-right shunting in systole and right-to-left shunting in diastole (Figure 1E and F). Multi-level pulmonary obstruction was observed due to sub-pulmonary conus and a bicuspid pulmonary valve (Figure 1C and D), leading to hypertrophied right ventricle (Figure 1B).
Laboratory results indicated polycythaemia (haemoglobin: 22 g/dL), iron deficiency (ferritin: 57 mg/L), and hyperuricaemia at 160 mg/L with normal renal function.
Due to the delayed age of diagnosis, limited literature supporting long-term outcomes after d-TGA surgery in adulthood, the patient’s socioeconomic status, and limited access to specialized unit care for adults with CHD, right heart catheterization and surgical repair were not considered.
Palliative care approach was implemented (intravenous hydration, phlebotomies, iron supplementation, allopurinol, and preventive measures against infective endocarditis).
D-transposition of the great arteries is a rare and potentially fatal CHD, accounting for 5% of all congenital heart defects, with a 90% mortality rate within the first year of life.^1^ The presentation of unrepaired d-TGA in adulthood is exceedingly rare. The longest reported life expectancy of unoperated TGA was observed in a 40-year-old female.^2^ This case highlights the challenges faced by adults with complex CHD and vulnerable social contexts, emphasizing the importance of early diagnosis, tailored care plans, and comprehensive support structures to optimize outcomes.^3^
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ferencz C, Rubin JD, Mc Carter RJ, Brenner JI, Neill CA, Perry LW, et al Congenital heart disease: prevalence at livebirth. The Baltimore-Washington Infant Study. Am J Epidemiol 1985;121:31–6.3964990 10.1093/oxfordjournals.aje.a 113979 · doi ↗ · pubmed ↗
- 2Naganur SH, Tiwari A, Pruthvi CR. Mystery still unresolved: untouched “Blue heart” presenting at 40 yrs of age. Ann Pediatr Cardiol 2020;13:72–74.32030038 10.4103/apc.APC_149_18PMC 6979036 · doi ↗ · pubmed ↗
- 3Bajpai P, Shah S, Misri A, Rao S, Suresh P, Maheshwari S. Assessment of operability in d-transposition of great arteries with ventricular septal defect: a practical method. Ann Pediatr Cardiol 2011;4:41–4.21677804 10.4103/0974-2069.79622 PMC 3104532 · doi ↗ · pubmed ↗