Bull's-Eye Signs: Rapid Appearance of Diffuse Lung Cancer Metastases in the Stomach
Daniella Mikhail, Ping He, Colton Smith, Anish Vinit Patel

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
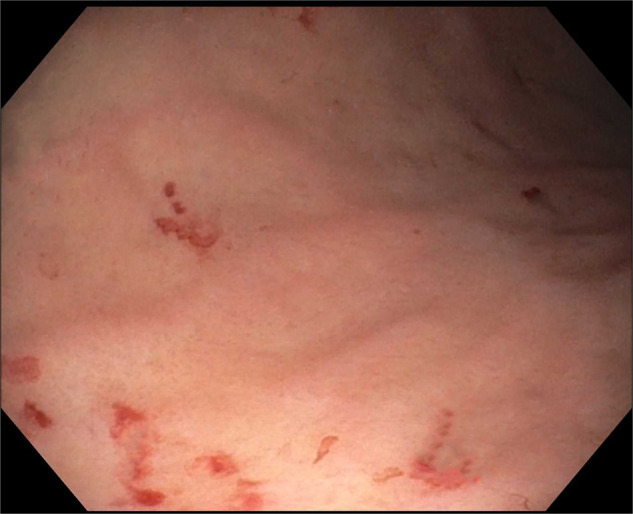 Figure 1
Figure 1 Figure 2
Figure 2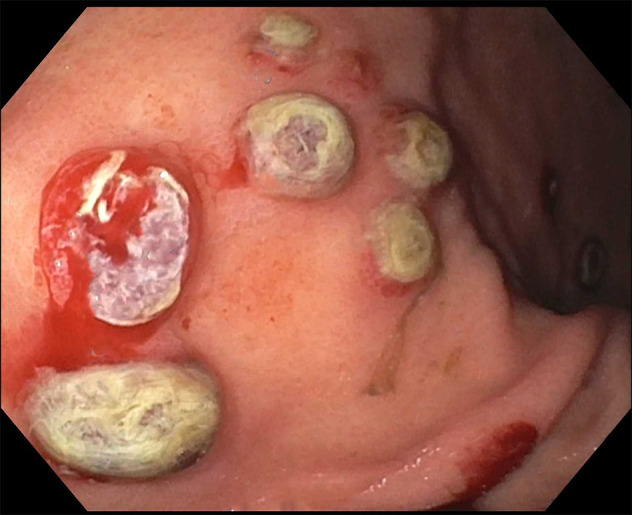 Figure 3
Figure 3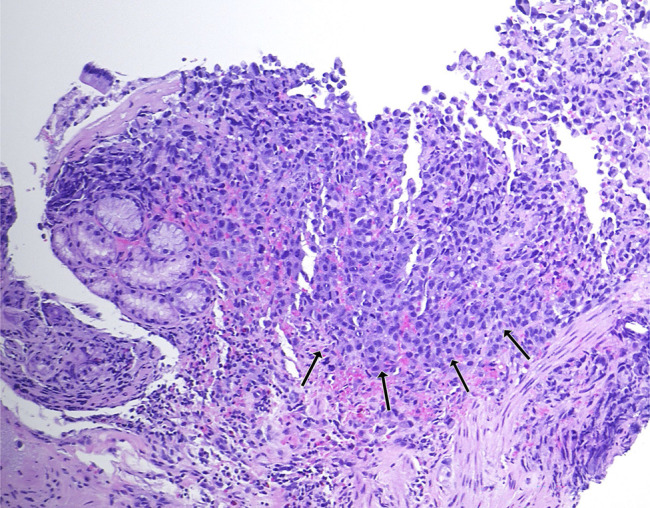 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMetastasis and carcinoma case studies · Cancer Diagnosis and Treatment · Oral and Maxillofacial Pathology
CASE REPORT
A 50-year-old man was recently diagnosed with right upper lobe lung invasive poorly differentiated adenocarcinoma (95% programmed cell death ligand 1 positivity) with metastases to the adrenals and femur. He underwent an upper endoscopy for evaluation of normocytic anemia (hemoglobin 8.6 g/dL, iron 72 mcg/dL) with findings of superficial gastritis alone with biopsies showing chronic active inflammation (Figure 1). The patient then developed melena 2 weeks later with acute blood loss anemia. Hemoglobin declined to 5.9 g/dL with no iron deficiency. He did not receive chemotherapy or radiation therapy in the interim. A repeat upper endoscopy was performed and visualized numerous 5–10 mm-sized mucosal nodules scattered diffusely throughout the gastric body and antrum (Figures 2–3). The nodules demonstrated characteristic bull's-eye signs—central ulcerations covered by adherent fibrinous material. Biopsies were taken and returned as infiltration of the gastric mucosa by a poorly differentiated adenocarcinoma composed of large pleomorphic tumor cells with predominantly fine nuclear chromatin and prominent nucleoli (hematoxylin & eosin stain, 40×) with morphology identical to the patient's known lung adenocarcinoma—indicative of metastatic lesions (Figure 4). He was maintained on acid suppression. Unfortunately, his clinical status deteriorated, and he was eventually transitioned to comfort measures.
Previous esophagogastroduodenoscopy 2 weeks prior performed for evaluation of anemia with only findings of superficial gastritis, with biopsies showing chronic active inflammation.
Esophagogastroduodenoscopy visualized numerous 5–10 mm-sized mucosal nodules scattered diffusely throughout the gastric body and antrum. The nodules demonstrated characteristic bull's-eye signs.
Mucosal nodules were biopsied for diagnosis.
Biopsies showed infiltration of the gastric mucosa by a poorly differentiated adenocarcinoma (arrows) composed of large pleomorphic tumor cells with predominantly fine nuclear chromatin and prominent nucleoli (hematoxylin & eosin stain, 40×) with morphology identical to the patient's known lung adenocarcinoma—indicative of metastatic lesions.
Lung cancer commonly metastasizes to the brain, liver, bones, and adrenal glands. Gastric metastases of lung cancer are rare and usually clinically silent. It may be diagnosed at the time of autopsy and is only infrequently captured endoscopically.^1^ Our case demonstrates that lung cancer can quickly progress, presenting with gastrointestinal bleeding and can appear as ulcerative nodules in an endoscopic evaluation.
DISCLOSURES
Author contributions: All authors contributed to the conception, design, drafting, revision, and approval of the final article. AV Patel is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.