Dysphagia Megalatriensis: An Uncommon Cardiac Mimicker of Gastroesophageal Dysphagia
Leonard Palatnic, Ross Robert Moyer, Clive Jude Miranda

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
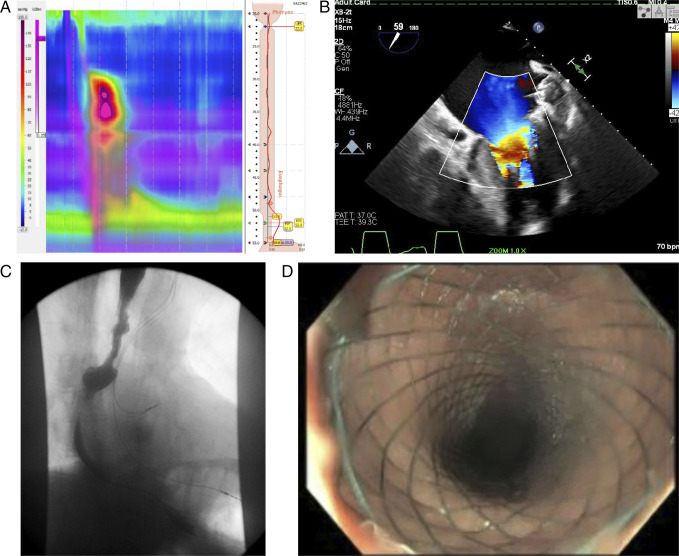 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTracheal and airway disorders · Esophageal and GI Pathology · Gastroesophageal reflux and treatments
CASE REPORT
An 82-year-old man with permanent atrial fibrillation status after atrioventricular nodal ablation and Watchman device placement presented for recurrent abdominal pain and dysphagia unresponsive to dietary modification or medications. He underwent esophageal manometry testing, which demonstrated findings concerning for grade III achalasia (Figure 1). To rule out pseudoachalasia, a computed tomography angiogram of the torso was obtained, revealing left atrium (LA) enlargement with mass effect causing compression of the lower one-third of the esophagus, resulting in mild obstruction and dilation of the proximal esophagus. A transthoracic echocardiogram then demonstrated severe LA dilation and bowing of the interatrial septum consistent with elevated LA pressures (Figure 1). With continued dysphagia, an upper gastrointestinal series revealed esophageal dysmotility and pulsion diverticulum in the mid-esophagus just above the LA (Figure 1). The patient underwent an esophagogastroduodenoscopy with esophageal stent placement (Figure 1). Notably, extrinsic compression of the mid-esophagus at the level of the LA was noted peri-procedure. This case illustrates the importance of always considering cardiac disease as an underlying etiology for persistent dysphagia. First described in 1969, dysphagia megalatriensis remains a challenging diagnosis.^1^ However, cardiac workup is warranted when there is true clinical suspicion.
(A) Esophageal manometry showing findings concerning for grade III achalasia. (B) Echocardiogram revealing severe left atrial dilation and bowing of the interatrial septum. (C) Upper gastrointestinal series revealing esophageal dysmotility and pulsion diverticulum in the mid-esophagus just above the left atrium. (D) Post-esophageal stent placement.
DISCLOSURES
Author contributions: L Palatnic, RR Moyer, and CJ Miranda compiled a literature review and wrote up the manuscript. CJ Miranda is the article guarantor.
Financial disclosure: None to report.
Previous presentation: Case presented at the American College of Gastroenterology Annual Scientific Meeting; October 23, 2023; Vancouver, BC, Canada.
Informed consent was obtained for this case report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.