Rapidly Growing Giant Squamous Cell Carcinoma of the Head: A Case Report
Zachary Leal, Mikayla Hobbs, Razia Gill, Megan Banfield, Mustapha Akhdar, Damian Casadesus

TL;DR
A rare case of a large, aggressive skin cancer on the head in an elderly man is reported, with a good prognosis if treated.
Contribution
This case report highlights the clinical presentation and management of a rare giant squamous cell carcinoma on the head.
Findings
A 70-year-old man presented with a 7.9 x 5.7 x 2.5 cm fungating mass on his scalp.
The biopsy confirmed poorly differentiated squamous cell carcinoma.
The prognosis is favorable with appropriate outpatient treatment.
Abstract
Giant squamous cell carcinoma (GSCC) of the skin arising on the head presents a distinctive clinical challenge due to its rarity, aggressive behavior, and potential for disfigurement. A male in his 70s with a history of tobacco cigarette use presented to the emergency department with a painful, bleeding mass on the right parietal scalp. On admission, a brain CT revealed a fungating mass with no cortical breakthrough or osseous erosion, measuring 7.9 x 5.7 x 2.5 cm. An ultrasound-guided tissue biopsy was performed and revealed poorly differentiated squamous cell carcinoma. The patient was discharged home with instructions from oncology to continue with outpatient treatment. At this time, the prognosis is good if treatment is received.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2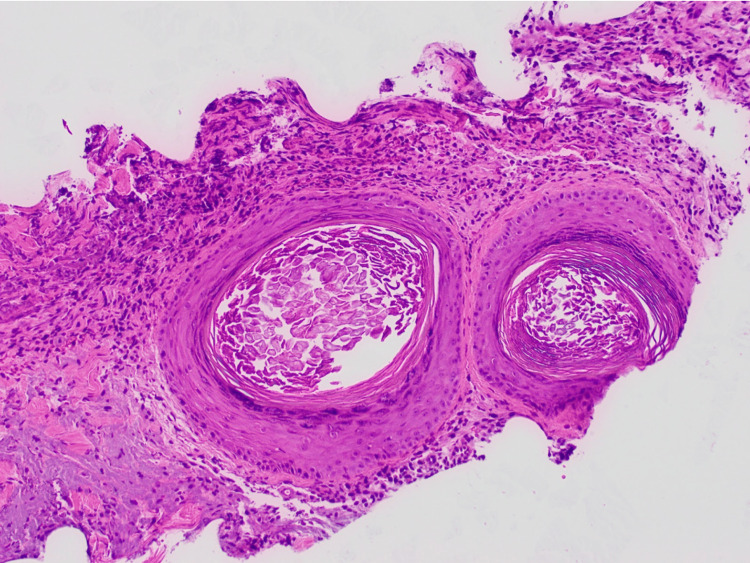 Figure 3
Figure 3| Laboratory test | Patient laboratory value | Normal laboratory range |
| White blood cells | 10,600/mm3 | 4500-11,000/mm3 |
| Hemoglobin | 12.3 g/dL | 13.5-17.5 g/dL |
| Hematocrit | 39% | 41-53% |
| Platelets | 179,000/mm3 | 150,000-400,000/mm3 |
| Potassium | 2.7 mEq/L | 3.5-5.0 mEq/L |
| Prothrombin time | 12.9 seconds | 11-15 seconds |
| Partial thromboplastin time | 32 seconds | 25-40 seconds |
| International normalized ratio | 0.96 | <1.1 |
| Red blood cells | 3.8 million/mm3 | 4.3-5.9 million/mm3 |
| Mean corpuscular volume | 95.3 mm3 | 80-100 mm3 |
| Lactic acid | 2.5 mmol/L | <2 mmol/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNonmelanoma Skin Cancer Studies · Cancer and Skin Lesions · Ear and Head Tumors
Introduction
The incidence of cutaneous squamous cell carcinoma (cSCC) has steadily been increasing and now accounts for 20% of nonmelanoma skin cancer (NMSC), making it the second most common skin malignancy in the United States [1]. When caught early, and treated appropriately, a majority of cSCC cases can be treated successfully. However, when neglected, severe disfigurement and growth may occur [2]. cSCC lesions have a broad clinical presentation. It may appear as papules, plaques, nodules, smooth in texture, scaly, ulcerated, pruritic, tender, or even asymptomatic [3]. Patients may also report neuropathic symptoms such as numbness, paresthesia, burning sensations, or paralysis which suggests perineural invasion of the tumor and a poorer prognosis [3]. Once cSCC tumors extend beyond 5 cm in diameter, they are classified as giant squamous cell carcinomas (GSCC) and become more complicated to treat, as well as more likely to present with metastasis or recurrence [2].
The unique anatomical considerations of the head region contribute to the complexities of managing these tumors, as their proximity to vital structures poses a risk of functional impairment and aesthetic compromise. The diagnosis of GSCC on the head relies on a combination of clinical assessment and histopathological confirmation. Given the potential for mimicking benign lesions or other skin conditions, a thorough biopsy is essential. Along with the diagnosis of SCC, it is crucial to stage the lesion and determine the extent of cancer spread. Multiple imaging modalities are used to determine such important aspects of the cancer. Lymph node biopsies are used to evaluate potential metastasis, while CT and MRI scans are useful for assessing the spread and involvement of distant organs. The main therapeutic approach for this variant of squamous cell carcinoma (SCC) is surgical excision with radiation often employed as an adjuvant therapy. The prognosis of this variant of cancer may vary, and it is important to involve various medical specialties to tailor a collaborative and individualized treatment plan. We present a patient with a rapidly growing, highly vascularized, and poorly differentiated GSCC of the head.
Case presentation
A male in his 70s with a past medical history of coronary artery disease with STEMI status post percutaneous coronary intervention, hypertension, and tobacco cigarette use presented to the emergency department (ED) due to unbearable pain associated with a mass on the right side of his scalp. He first noticed the mass in the mirror two months prior, which at the time was painless and the size of a quarter. The mass continued to rapidly grow, eventually becoming painful, and started bleeding about one month before the ED visit. It had continued to bleed every day since then. The patient stated the pain progressed over time and described his current pain as constant with a rating of 17/10. He denied fever, ear pain, vision changes, eye pain, and throat pain. He was seen by his primary care physician for the mass and was given several courses of antibiotics and analgesics, which did not result in improvement. He was scheduled to see a dermatologist in the next month, but the pain became unbearable causing him to seek care earlier. The patient is a tobacco smoker and reports drinking 1-2 beers per week. The only medication the patient reported taking at home was Pepcid.
On physical exam, vitals were stable with a blood pressure of 125/61 mmHg, a temperature of 36.9°C, a heart rate of 64 beats per minute, a respiratory rate of 20 breaths per minute, and an oxygen saturation of 98% on room air. The patient appeared in distress due to pain. The examination of the head showed a tender 6 × 5 cm fungating violaceous mass draining serosanguineous fluid on the right parietal scalp (Figure 1). The rest of the physical examination was unremarkable.
Fungating violaceous mass (6 × 5 cm) with serosanguineous fluid on the right parietal scalp.
Relevant laboratory results on admission were remarkable for normocytic anemia, critical hypokalemia, and lactic acidosis (Table 1). Differential diagnoses included a collection of fluid, osteomyelitis, keratoacanthoma, sebaceous carcinoma, SCC, and other malignancies. The patient was admitted to the hospital and started treatment with pain management and correction of potassium levels. A CT of the head revealed a 7.9 x 5.7 x 2.5 cm heterogeneously enhancing, fungating mass overlying the right parietal scalp, with no cortical breakthrough, no osseous erosion, no enhancing masses of the cerebral parenchyma, and no mass effect or midline shift (Figure 2). An ultrasound-guided tissue biopsy was performed, and the patient was discharged home with the primary doctor and dermatology follow-up. The histopathological study revealed a poorly differentiated SCC (Figure 3). The patient returned to the hospital a month later because of increased pain. After treatment, the patient was scheduled for oncological treatment; however, the patient was lost to follow-up.
CT of the head with contrast showing mass overlying the right parietal scalp.
Histopathological study of scalp mass showing poorly differentiated squamous cell carcinoma.
Discussion
SCC is most common in white populations that have a fair complexion, blue eyes, and blonde/red hair, with most patients being white males in their 60s [1]. Factors that predispose patients to develop cSCC include light skin, exposure to sunlight, ultraviolet radiation, immunosuppression, human papillomavirus, chronic conditions that lead to scarring, genetic syndromes, and certain environmental exposures [4]. The main high-risk prognostic markers for cSCC include the tumor size, site, history of radiotherapy, immunosuppression, and perineural invasion [5].
GSCC is defined by its substantial size, often exceeding 5 cm or even 10 cm in diameter. Grossly GSCC often manifests as a large, ulcerated, exophytic mass with irregular borders and hemorrhage or weeping of the tumor mass frequently observed [6]. Histologically, GSCC exhibits features typical of conventional cSCC demonstrating marked cellular atypia, pleomorphism, and high mitotic activity, with keratin pearls and intercellular bridges [7]. GSCC is also characterized by its disproportionately large size and rapid growth rate, often leading to extensive tissue necrosis and inflammatory infiltrates.
The main feature that makes our patient rather notable is the remarkably rapid rate of tumor growth he experienced. Although a great amount of literature has been published discussing SCC, there remains to be limited literature that specifically discusses tumor growth rate and what affects it. Several hypotheses include states of immunosuppression, increased age, variations in gene expression signatures, unhealed prior cutaneous lesions, and smoking. Billingsley et al. hypothesized that tumor growth rate may be influenced by states of immunosuppression and may be due to a viral etiology [8]. Our patient, however, was not immunosuppressed. Another study found the rate of tumor progression to grow exponentially with increasing age, with an asymptote at the eighth decade of life [9]. This study may perhaps be a good explanation of our patient's rapid growth rate, as our patient was in fact in his eighth decade of life and, according to the study, indicates that patients at his age would experience the fastest rate of tumor growth compared to other age groups. Another study concluded that the use of gene expression profile testing such as DecisionDX-SCC demonstrated a high degree of analytical precision in risk classification after analyzing gene expression of primary tumor tissue, indicating that variations in genetic mutations may alter tumor progression and prognosis [10]. Another common feature seen in much of the published literature regarding rapidly growing cSCC is that the tumors in those patients may have progressed from prior cutaneous lesions, which did not appear to be the case in our patient. One study discussed a patient who developed aggressive cSCC and had a history of recurrent unhealed ulcerative scalp lesions [11]. Another risk factor in our patient that possibly impacted his tumor progression is his history of smoking, although it is unclear to what degree. There are numerous reports linking smoking to cSCC; however, one study found it had little to no association with development on the scalp [12].
Conclusions
GSCC has the potential to be detected earlier with surveillance, follow-up, and early treatment. This tumor is known to have a great prognosis; however, the prognosis can be dismal if left untreated. Optimal treatment of GSCC consists of wide local excision with tumor-free margins, Mohs micrographic surgery, chemotherapy, radiation therapy, or a combination of the four. Physicians should be aware that an unresolved mass or lesion needs a timely biopsy for correct diagnosis to improve the survival of the patient. In our patient, constrained access to healthcare and a lack of comprehension regarding his medical condition contributed to a delayed diagnosis, potentially compromising the continuity of care and, consequently, leading to a potentially more unfavorable prognosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cutaneous squamous cell carcinoma of the head and neck J Skin Cancer Gurudutt VV Genden EM 502723201120112146138710.1155/2011/502723 PMC 3064996 · doi ↗ · pubmed ↗
- 2A giant squamous cell carcinoma of the skin of the thoracic wall: a case report and review of the literature J Med Case Rep Misiakos EP Damaskou V Koumarianou A Gouloumi AR Patapis P Zavras N Machairas A 1361120172849481610.1186/s 13256-017-1281-8PMC 5426016 · doi ↗ · pubmed ↗
- 3Cutaneous squamous cell carcinoma Clin Lab Med Parekh V Seykora JT 5035253720172880249810.1016/j.cll.2017.06.003 · doi ↗ · pubmed ↗
- 4Cutaneous squamous cell carcinoma: incidence, risk factors, diagnosis, and staging J Am Acad Dermatol Que SK Zwald FO Schmults CD 2372477820182933270410.1016/j.jaad.2017.08.059 · doi ↗ · pubmed ↗
- 5Aggressive cutaneous squamous cell carcinoma of the head and neck: a review Curr Oncol Desai N Divatia MK Jadhav A Wagh A 663466473020233750434710.3390/curroncol 30070487 PMC 10378287 · doi ↗ · pubmed ↗
- 6Squamous cell carcinoma of the skin: epidemiology, classification, management, and novel trends Int J Dermatol Kallini JR Hamed N Khachemoune A 1301405420152542822610.1111/ijd.12553 · doi ↗ · pubmed ↗
- 7Cutaneous squamous cell carcinoma: from pathophysiology to novel therapeutic approaches Biomedicines Fania L Didona D Di Pietro FR 171920213357237310.3390/biomedicines 9020171 PMC 7916193 · doi ↗ · pubmed ↗
- 8Rapidly growing squamous cell carcinoma J Cutan Med Surg Billingsley EM Davis N Helm KF 193197319991036639310.1177/120347549900300406 · doi ↗ · pubmed ↗