Arterial structure and function in children with inflammatory bowel disease
Asha Jois, Diana Zannino, Anthony G Catto‐Smith, Meg Kaegi, Jonathan P Mynard, Jeremy Rosenbaum, Mark Oliver, Winita Hardikar, George Alex, David Burgner

TL;DR
This study found no evidence of early arterial changes in children with inflammatory bowel disease that would indicate increased cardiovascular risk.
Contribution
The study is the first to show that pediatric IBD does not yet cause measurable arterial dysfunction after a few years of disease duration.
Findings
Children with IBD did not show differences in arterial structure or function compared to healthy controls.
No significant differences were found between Crohn's disease and ulcerative colitis patients in arterial measurements.
Early IBD diagnosis may still allow for interventions to reduce future cardiovascular risk.
Abstract
People with inflammatory bowel disease (IBD) have an increased risk of cardiovascular disease, including in younger adulthood. This may arise in part from chronic, systemic low‐grade inflammation. The process of atherosclerosis may begin in childhood. We sought to determine whether pediatric IBD is associated with adverse changes in arterial structure and function as a marker of early increased cardiovascular risk. We performed a case–control study comparing children with IBD for a median disease duration of 2.49 (interquartile range 1.23, 4.38) years with healthy children. In a single visit, we collected baseline clinical and anthropometric data, and measured blood pressure, pulse wave velocity, carotid artery distensibility, and aortic and carotid intima‐media thickness. High‐sensitivity C‐reactive protein and fasting lipids were measured. We enrolled 81 children with IBD (40 with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
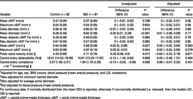 Figure 1
Figure 1| Variable | Control ( | IBD ( |
|
|---|---|---|---|
| Age at interview (years) | 11.88 (3.19) | 14.45 (2.88) | <0.001 |
| Time since diagnosis (years) | ‐ | 2.49 [1.23, 4.38] | ‐ |
| Sex—Male | 40 (49%) | 40 (49%) | >0.99 |
| BMI (kgm−2) | 19.10 (3.22) | 20.71 (3.96) | 0.005 |
| BMI | 0.39 (0.97) | 0.23 (1.12) | 0.335 |
| Waist hip ratio | 0.81 (0.06) | 0.83 (0.06) | 0.021 |
| Mean arterial blood pressure (mmHg) | 80.54 (7.59) | 82.10 (8.11) | 0.208 |
| Systolic blood pressure (mmHg) | 113.8 (9.7) | 116.6 (10.7) | 0.082 |
| Diastolic blood pressure (mmHg) | 65.4 (7.0) | 67.0 (6.9) | 0.146 |
| Triglycerides (mmol/L) | 0.78 (0.32) | 0.86 (0.36) | 0.133 |
| Total cholesterol (mmol/L) | 4.23 (0.70) | 3.96 (0.71) | 0.017 |
| LDL cholesterol (mmol/L) | 2.33 (0.62) | 2.21 (0.61) | 0.199 |
| HDL cholesterol (mmol/L) | 1.54 (0.40) | 1.36 (0.31) | 0.002 |
| Glucose (mmol/L) | 4.36 (0.43) | 4.42 (0.39) | 0.316 |
| High‐sensitivity CRP (mg/L) | 0.3 [0.15–0.6] | 0.8 [0.3–2.5] | <0.001 |
| Post pubertal ( | 22 (27%) | 51 (63%) | <0.001 |
| Variable | Control | IBD | Unadjusted | Adjusted | ||
|---|---|---|---|---|---|---|
| Difference (95% CI) |
| Difference (95% CI) |
| |||
| Mean cIMT (mm) | 0.47 (0.05) | 0.47 (0.05) | 0 (−0.01, 0.02) | 0.788 | 0 (−0.02, 0.01) | 0.56 |
| Maximum cIMT (mm) | 0.54 (0.05) | 0.54 (0.05) | 0 (−0.01, 0.02) | 0.654 | 0 (−0.02, 0.01) | 0.56 |
| Delta diameter (mm) | 0.95 (0.16) | 0.95 (0.19) | −0.01 (−0.07, 0.05) | 0.815 | 0 (−0.06, 0.07) | 0.89 |
| Mean diameter (mm) | 6.28 (0.46) | 6.62 (0.38) | 0.35 (0.21, 0.49) | <0.001 | 0.01 (−0.06, 0.09) | 0.77 |
| Mean diastolic cIMT Far (mm) | 0.49 (0.05) | 0.49 (0.05) | 0 (−0.02, 0.02) | 0.994 | 0 (−0.02, 0.01) | 0.78 |
| Max diastolic cIMT Far (mm) | 0.57 (0.05) | 0.57 (0.05) | 0 (−0.02, 0.02) | 0.962 | 0 (−0.02, 0.02) | 0.85 |
| Mean aIMT (mm) | 0.54 (0.08) | 0.58 (0.09) | 0.03 (0, 0.06) | 0.027 | 0.02 (−0.02, 0.05) | 0.363 |
| Maximum aIMT (mm) | 0.63 (0.09) | 0.67 (0.10) | 0.03 (0, 0.07) | 0.044 | 0.02 (−0.02, 0.05) | 0.379 |
| Pulse wave velocity (m/s) | 4.43 (0.65) | 4.71 (0.75) | 0.28 (0.06, 0.5) | 0.012 | −0.04 (−0.24, 0.16) | 0.671 |
| Carotid artery distensibility (%) | 16.01 [14.02–18.46] | 15.81 [13.43–17.97] | −0.12 (−1.45, 0.83) | 0.858 | 0.45 (−0.46, 1.31) | 0.494 |
| Carotid artery compliance ×10−2 (mm/mmHg) | 2.07 [1.82–2.31] | 1.94 [1.75–2.26] | −0.13 (−0.25, −0.06) | 0.056 | 0.08 (−0.07, 0.22) | 0.401 |
- —National Health and Medical Research Council 10.13039/501100000925
- —State Government of Victoria Operational Infrastructure Support Program (non‐sp) 10.13039/501100004752
- —Gastroenterological Society of Australia 10.13039/501100001202
- —University of New England, Australia 10.13039/501100001772
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Health and Disease Prevention · Sodium Intake and Health · Inflammatory Bowel Disease
Introduction
Inflammation is key to the pathogenesis of atherosclerosis,1 which develops asymptomatically across the life course and results in cardiovascular disease (CVD) in adulthood. CVD is the leading cause of morbidity and mortality worldwide.2 Patients with inflammatory bowel disease (IBD) have an increased risk of CVD.3, 4 This may be mediated by chronic, systemic, low‐grade inflammation, in addition to a hypercoagulable state and altered gut microbiota.5, 6
Noninvasive cardiovascular measures predict CVD in adults and are used to assess risk from childhood onwards.6, 7, 8, 9 These measures include blood pressure (BP), pulse wave velocity (PWV), carotid artery distensibility, and large arterial structure (aortic and carotid intima‐media thickness, IMT). Childhood is a critical period for detecting potentially adverse vascular phenotypes, allowing intervention before changes become irreversible.10
There is evidence to suggest preclinical atherosclerosis occurs in young adults with IBD, yet data from children are scarce and conflicting. This may reflect methodological issues, such as considering Crohn's disease (CD) and ulcerative colitis (UC) together.11, 12 In adults, IBD has been associated with increased PWV (indicative of increased arterial stiffness);13 however, two studies in children with IBD found no association.14, 15
To address these knowledge gaps, we aimed to determine whether pediatric IBD is associated with differences in arterial structure and function as a marker of increased CVD risk. We hypothesized that patients with pediatric IBD would have increased aortic and carotid IMT, increased PWV, and decreased carotid distensibility and compliance compared with healthy controls.
Methods
Study population
Participants were enrolled between October 2013 and May 2018. Children aged 5–18 years with a diagnosis of IBD for at least 6 months duration were eligible. Forty participants had a diagnosis of CD, and 40 had UC, with one participant with unspecified IBD (IBDU), as classified by their treating gastroenterologist. Participants were recruited through the gastroenterology outpatient service at the Royal Children's Hospital (RCH, Melbourne, Australia), a major tertiary pediatric hospital. Informed consent was obtained from participants' parent or guardian. Participants with IBD were excluded if their disease was limited to proctitis or perianal disease, or they were admitted to hospital within the preceding month. Eighty control participants, also between 5 and 18 years, were recruited through outpatient departments at the RCH or referred through case participants (non‐relatives) or staff members working at RCH or affiliated institutions. Informed consent was also provided for this group. Participants were excluded if they had an inflammatory comorbidity.
Data collection
All participants were assessed at a single study‐dedicated visit. Demographic and anthropometric data (height, weight, waist, and hip circumference) were collected, using standard protocols described previously.16 Pubertal status was self‐reported using Tanner Staging. A blood sample was collected after a minimum 6‐h fast for measurement of high‐sensitivity C‐reactive protein (hsCRP) (Abbott Architect, IL, USA), glucose, triglycerides, total cholesterol, high‐density lipoprotein (HDL), and low‐density lipoprotein (LDL) cholesterol (Vitros 5600, Ortho‐Clinical diagnostics, NJ, USA).
Cardiovascular measures
Participants were placed supine for three measurements of carotid femoral pulse wave velocity (cfPWV) with the SphygmoCor® XCEL device (AtCor Medical Pty Ltd., NSW, Australia) after a 5‐min rest, as per the manufacturer's protocol. Participants remained supine for three BP measurements using the same device. Ultrasound images of the carotid artery and abdominal aorta were taken using a portable ultrasound machine Vivid‐I (General Electronics Healthcare, Chicago, IL, USA), with simultaneous ECG gating as described previously.17, 18 Participants were supine with head turned to 45° for optimal carotid artery positioning. For carotid images, we recorded cine loops of at least five cardiac cycles for offline analysis, focusing on the intima‐media complex of the posterior wall of the right common carotid artery. Aortic images focused on the posterior wall, just proximal to the femoral bifurcation.
Data analysis
Analyses of both the carotid artery and abdominal aorta IMT were performed using “Coast,” an in‐house code programmed in Matlab (R2022b, The Mathworks Inc., Natick, MA, USA) that uses a template registration segmentation algorithm and has been validated against manual measurements. For carotid analysis, three to five end‐diastolic images were used to calculate the mean and maximum IMT from a 4–10 mm segment of the far wall, measured 1 cm proximal to the carotid bulb. For aortic analysis, the same number of end‐diastolic images was used to calculate the mean and maximum IMT from a 10‐mm segment of the posterior wall. One or both of two graders, blinded to subject status, measured all IMTs. We measured the minimum carotid artery vessel diameter, distensibility [(maximum diameter − minimum diameter)/minimum diameter × 100%], and compliance [(maximum diameter − minimum diameter)/brachial pulse pressure]. These parameters could not be obtained from images of the abdominal aorta due to image quality. Intra‐class correlation (ICC) for inter‐rater reliability was 0.74 and 0.95 for cIMT and aIMT, respectively. The ICC for intra‐rater reliability was 0.84 and 0.98 for cIMT and aIMT, respectively.
Statistical analysis
Analysis was performed using R software (version 4.2.2, R Foundation, Vienna, Austria). For continuous data, mean (SD) or median (interquartile range with Q1, Q3) were reported. Categorical data were summarized by count and percentage of nonmissing data. Unadjusted comparisons were based on the two‐sample t‐test or Wilcoxon rank sum test. Cardiovascular measures were compared using linear regression models, and quantile regression models (with bootstrapped P‐values) for non‐normally distributed outcomes. Models were adjusted for age, sex, BMI z‐score, BP (apart from PWV), and LDL cholesterol.
Results
We enrolled 81 participants with IBD and 82 control participants. Of the IBD participants, 40 had CD (22 [55%] male, 14.58 [2.98] years), 40 had UC (17 [42%] male, 14.32 [2.84] years), and 1 had IBDU. Compared with controls, children with IBD were older, had a higher BMI, higher waist‐to‐hip ratio, lower total cholesterol, lower HDL cholesterol, higher CRP, and a higher proportion of children were post‐pubertal (Table 1). Participants with CD had a median (IQR) disease duration of 3.01 (1.56–4.35) years and those with UC had a median (IQR) of 2.08 (1.02–4.53) years. Eighteen (45%) of the patients with CD and 2 (5%) with UC were on biologic therapy, while 20 (50%) with CD and 19 (45%) with UC were on an immunomodulator (see Supplementary Data).
Unlike previous studies,11, 12 we analyzed arterial structure and function of children with UC and CD separately, which are provided in the Supplementary Data. Once we established there was no difference between the two groups, we were able to pool the results to increase statistical power. After adjusting for age, sex, BMI z‐score, BP, and LDL cholesterol, there was no difference in measures of arterial structure and function in children with IBD compared with controls (Table 2).
Children with CD had a lower waist‐to‐hip ratio than children with UC, but otherwise had comparable participant characteristics (see Table S1, Supporting information). Following adjustment, there was no difference in parameters of vascular structure or function between the two IBD subtypes (see Table S2).
Discussion
In this single‐center, cross‐sectional case–control study, we found no evidence of differences in measures of cardiovascular structure or function in children with IBD compared with healthy controls. In addition, we did not observe any differences between those with CD and UC. Adverse cardiovascular measures in those with IBD may require a longer disease duration to become evident and may reflect whether a child with IBD has well‐controlled disease or ongoing inflammatory activity. For example, elevated cfPWV in adults with IBD was shown to reverse over time with adequate disease control.19
There are few prior studies that have investigated cardiovascular measures in children with IBD.11, 12, 14 One study found that children with IBD had increased cIMT compared with controls.11 Other parameters of vascular structure and function were not assessed.11 In another study with a younger cohort with a shorter disease duration, mean aIMT was higher in IBD patients than controls, with no difference in cIMT.12 Neither study adjusted for potential confounders. cfPWV has not previously been shown to differ in children with IBD compared with controls,14, 15 consistent with our findings.
Our study's limitations include its cross‐sectional nature, and lack of standardized data on disease classification, severity, and disease activity including fecal calprotectin and erythrocyte sedimentation rate. Disease activity indices are limited by only reflecting a single time point. Our sample size was insufficient to allow sensitivity analyses by treatment modality. Despite these limitations, to the best of our knowledge, this is one of the largest cohorts of children with IBD to be investigated for arterial structure and function. Our study is the first in children to measure and adjust for major confounding, which may explain the conflicting results in the literature to date.
We did not show any differences in arterial structure and function in children with IBD compared with healthy controls. While pre‐atherosclerotic changes have been reported in patients with IBD in early adulthood, it likely takes years of poorly controlled disease with chronic inflammation for these changes to develop. IBD diagnosed in childhood may present a window of opportunity to actively reduce cardiovascular risk and promptly induce sustained remission, to potentially prevent future adverse cardiovascular outcomes. Longitudinal studies, over a prolonged duration and with a larger sample size, are required to confirm our findings and inform preventative strategies and intervention targets.
Ethical approval
This study was approved by the RCH Human Research Ethics Committee (reference number 33065).
Patient consent
Informed consent for participation in the study was obtained from participants' parent or guardian.
Supporting information
Data S1 Supporting information.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Libby P . Inflammation in atherosclerosis. Nature. 2002; 420: 868–874.12490960 10.1038/nature 01323 · doi ↗ · pubmed ↗
- 2Roth GA , Mensah GA , Johnson CO et al. Global burden of cardiovascular diseases and risk factors, 1990‐2019: update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020; 76: 2982–3021.33309175 10.1016/j.jacc.2020.11.010PMC 7755038 · doi ↗ · pubmed ↗
- 3Kristensen SL , Ahlehoff O , Lindhardsen J et al. Disease activity in inflammatory bowel disease is associated with increased risk of myocardial infarction, stroke and cardiovascular death—a Danish nationwide cohort study. P Lo S One. 2013; 8: e 56944.23457642 10.1371/journal.pone.0056944 PMC 3574079 · doi ↗ · pubmed ↗
- 4Sun HH , Tian F . Inflammatory bowel disease and cardiovascular disease incidence and mortality: a meta‐analysis. Eur. J. Prev. Cardiol. 2018; 25: 1623–1631.30074405 10.1177/2047487318792952 · doi ↗ · pubmed ↗
- 5Cainzos‐Achirica M , Glassner K , Zawahir HS et al. Inflammatory bowel disease and atherosclerotic cardiovascular disease: JACC review topic of the week. J. Am. Coll. Cardiol. 2020; 76: 2895–2905.33303079 10.1016/j.jacc.2020.10.027 · doi ↗ · pubmed ↗
- 6Järvisalo MJ , Jartti L , Näntö‐Salonen K et al. Increased aortic intima‐media thickness: a marker of preclinical atherosclerosis in high‐risk children. Circulation. 2001; 104: 2943–2947.11739310 10.1161/hc 4901.100522 · doi ↗ · pubmed ↗
- 7Poredos P . Intima‐media thickness: indicator of cardiovascular risk and measure of the extent of atherosclerosis. Vasc. Med. 2004; 9: 46–54.15230488 10.1191/1358863 x 04vm 514ra · doi ↗ · pubmed ↗
- 8Lorenz MW , Gao L , Ziegelbauer K et al. Correction: predictive value for cardiovascular events of common carotid intima media thickness and its rate of change in individuals at high cardiovascular risk – results from the PROG‐IMT collaboration. P Lo S One. 2018; 13: e 0204633.30235339 10.1371/journal.pone.0204633 PMC 6147579 · doi ↗ · pubmed ↗