Chitotriosidase: Providing confirmation of cutaneous sarcoidosis when angiotensin converting enzyme fails
Carlie Reeves, Colleen D. Powers, Robert T. Brodell

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1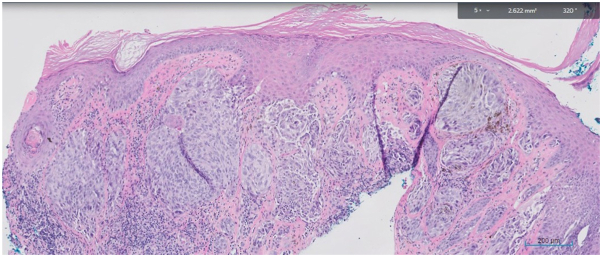 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoidosis and Beryllium Toxicity Research · Studies on Chitinases and Chitosanases · Vasculitis and related conditions
Introduction
Sarcoidosis is a state of granuloma formation that can occur in any organ system. Diagnosis relies on pathologic evidence of granulomas as well as a compatible clinical and radiographic presentation.1 The initial symptom is greatly varied, and many patients are asymptomatic, making diagnosis difficult. Chitotriosidase is a serologic marker that can assist in the diagnosis of patients with isolated cutaneous sarcoidosis in the absence of classic radiographic and serologic findings, such as hypercalcemia, elevated angiotensin converting enzyme (ACE) level, or hilar adenopathy. Chitotriosidase (chitinase 1) is a hydrolytic enzyme produced by macrophages that breaks down glycosidic bonds in chitin and plays a role in defense against fungi, insects, and nematodes.2 Our case report demonstrates the utility of chitotriosidase in diagnosing a patient with lupus pernio, a type of cutaneous sarcoidosis, when other work-up was inconclusive.
Case report
A 63-year-old African American woman presented with an 8- to 10-year history of slowly enlarging 2 mm slightly hyperpigmented papules on the tip of the nose and alar rim (Fig 1, A and B). A shave biopsy of the left nasal ala revealed islands of naked epithelioid granulomas (sarcoidal tubercles) with multinucleated giant cells and a slight admixture of lymphocytes throughout the dermis (Fig 2). Although ACE level was normal at 52 U/L (normal value: 16-85 U/L), chitotriosidase was elevated at 295 nmol/h/mL (normal value: 4.0-120.0 nmol/h/mL). Antinuclear antibody and antineutrophilic cytoplasmic antibodies were normal.Fig 1A, Indurated papules coalescing in a plaque on the nasal tip and alar rim bilaterally, demonstrating a cobblestone appearance. Erosion on left alar rim consistent with biopsy site. Erythematous to hypopigmented patches on medial aspect of the cheeks, sparing the nasolabial fold. B, Atrophic papules on the nasal tip and firm papules along the left nasal ala.Fig 2. Biopsy of the left nasal ala revealed islands of naked epithelioid granulomas with multinucleated giant cells and lymphocytes throughout the dermis.
Patient’s past medical history included a secondary spontaneous pneumothorax, with a computed tomography scan demonstrating very mild interstitial lung disease. A bronchoscopy was performed, which demonstrated inconclusive findings. Patient also had a distant 25 pack-year history of smoking.
The diagnosis of lupus pernio was based on her skin findings, sarcoidal granulomas, and elevated chitotriosidase level. Hydroxychloroquine 200 mg twice daily was initiated, and an ophthalmologic examination was scheduled as a baseline for monitoring of hydroxychloroquine retinopathy. Pulmonary function testing revealed moderate restriction and moderate decreased diffusing capacity of the lungs with carbon monoxide. Radiologic imaging demonstrated persistent lymphadenopathy and ground-glass opacities, findings suggestive of active inflammation. Therefore, prednisone was initiated at a dose of 20 mg for 6 weeks. The papules and plaques demonstrated 50% flattening of the cobblestone appearance over 6 months. Repeat chitotriosidase level 7 months after treatment initiation showed improvement to 131 nmol/h/mL.
Discussion
The percentage of sarcoidosis cases that present with cutaneous involvement varies widely across the literature, likely due to the differences in patient populations. Cutaneous involvement is seen in 20% to 35% of patients with sarcoidosis.3 Although erythema nodosum is the most common cutaneous manifestation of sarcoidosis, lupus pernio is the only pathognomonic cutaneous finding.4 Lupus pernio is most commonly seen in women aged 45 to 65 years of African descent. Other less common cutaneous manifestations of sarcoidosis include papular sarcoidosis, nodular sarcoidosis, and plaque sarcoidosis.5 Because of the wide array of skin presentations and variability in the initial presenting symptoms, the diagnosis is often delayed.5 In 20% of patients, skin lesions are the presenting signs of systemic sarcoidosis, but in 30% of patients, the skin lesions appear up to 10 years after the systemic disease has been documented.3 Skin and systemic symptoms appear simultaneously in 50% of patients.3 The diagnosis of sarcoidosis is often made after lymphadenopathy is noted incidentally on chest x-ray.6 Serologic studies can assist in diagnosing sarcoidosis when imaging is inconclusive, as demonstrated in our patient.
Although lupus pernio itself is not life-threatening, initiating treatment promptly is important for curtailing disfigurement. Hydroxychloroquine is the preferred initial therapy for cutaneous sarcoidosis, whereas prednisone is preferred for treating the lungs. In this patient, the diagnosis led to monitoring of pulmonary status through repeat pulmonary function tests and high-resolution computed tomography scans.
The ACE level has been the most frequently used laboratory test for patients with sarcoidosis.7 ACE is elevated in 60% of patients with sarcoidosis and is an indication of the total body granuloma burden.7 Chitotriosidase can assess disease activity in sarcoidosis with an approximate sensitivity of 88.6% and specificity of 92.8%.2 This is in contrast to a sensitivity of 66% and specificity of 54% seen in ACE.7 The chitotriosidase test is performed using a blood sample, from which the plasma is separated in a laboratory. The level of chitotriosidase enzyme in the plasma is then measured. It is not routinely available at most hospital laboratories and thus is a send-out test.
Seven months after initiation of treatment in our patient, a repeat chitotriosidase was mildly elevated at 131 nmol/h/mL, which had decreased significantly from 295 nmol/h/mL. A study found that chitotriosidase is seen at its highest levels in patients treated with systemic steroids who have persistent disease.2 Concentrations of chitotriosidase decreased dramatically after steroid dose was increased or new immunosuppressant therapy was administered.2 As a result, the decrease in chitotriosidase seen in our patient may explain the good response of systemic inflammation to therapy, given that chitotriosidase remained low months after the last dose of prednisone was taken.
This case is novel because it demonstrates the utility of chitotriosidase in diagnosing cutaneous sarcoidosis. The literature on chitotriosidase has only been in reference to systemic sarcoidosis, not its cutaneous manifestations. In addition, there is very little mention of chitotriosidase in the dermatologic literature. One article found chitotriosidase to be a marker of systemic inflammation in psoriasis, but associations between chitotriosidase and cutaneous sarcoidosis have not been reported.8 Because skin lesions are the manifesting symptoms in 20% of patients with sarcoidosis, chitotriosidase is a marker that dermatologists should use in the diagnostic work-up for cutaneous sarcoidosis.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Soto-Gomez N.Peters J.I.Nambiar A.M.Diagnosis and management of sarcoidosis Am Fam Phys 9310201684084827175719 · pubmed ↗
- 2Bargagli E.Maggiorelli C.Rottoli P.Human chitotriosidase: a potential new marker of sarcoidosis severity Respiration 762200823423810.1159/00013400918487875 · doi ↗ · pubmed ↗
- 3Anjaneyan G.Vora R.Lupus pernio without systemic involvement Indian Dermatol Online J 44201331431710.4103/2229-5178.12065624350015 PMC 3853900 · doi ↗ · pubmed ↗
- 4Afacan Yıldırım E.Aladağ Öztürk P.Adışen E.Köktürk N.The relationship between erythema nodosum and prognosis in systemic sarcoidosis: a retrospective cohort study An Bras Dermatol 975202260661110.1016/j.abd.2021.09.01135811196 PMC 9453497 · doi ↗ · pubmed ↗
- 5Williams J.R.Frey C.Cohen G.F.Cutaneous sarcoidosis in skin of color J Drugs Dermatol 227202369569710.36849/JDD.700837410043 · doi ↗ · pubmed ↗
- 6Garland S.Falk N.Wilk A.Less common respiratory conditions: sarcoidosis FP Essent 5022021182233683850 · pubmed ↗
- 7PopevićS.Šumarac Z.JovanovićD.Verifying sarcoidosis activity: chitotriosidase versus ACE in sarcoidosis - a case-control study J Med Biochem 354201639040010.1515/jomb-2016-001728670191 PMC 5471634 · doi ↗ · pubmed ↗
- 8İlanbey B.ElmasÖ.F.Sözmen E.Y.A novel marker of systemic inflammation in psoriasis and related comorbidities: chitotriosidase Turk J Med Sci 51420212318232310.3906/sag-2101-13733819975 · doi ↗ · pubmed ↗