Gestational diabetes mellitus as a risk factor for future Type-2 diabetes mellitus: An experience from a tertiary care diabetes hospital, Karachi - Pakistan
Musarrat Riaz, Nazish Waris, Akifa Saadat, Asher Fawwad, Abdul Basit

TL;DR
Women with gestational diabetes are at high risk of developing Type-2 diabetes within five years, with risk factors including family history and hypertension.
Contribution
This study identifies gestational diabetes as a strong predictor of future Type-2 diabetes in women, emphasizing early screening and lifestyle changes.
Findings
46% of women with gestational diabetes developed Type-2 diabetes within one year.
Family history of diabetes and hypertension during pregnancy were significant risk factors.
Most cases of gestational diabetes occurred in the second trimester and among multiparous women.
Abstract
To evaluate the history of gestational diabetes mellitus and other risk factors in women presenting with Type-2 diabetes mellitus at a tertiary care hospital. This cross-sectional study was carried out at Baqai Institute of Diabetology & Endocrinology (BIDE), Baqai Medical University (BMU), Karachi-Pakistan from July 2019 to May 2022. Women with Type-2 diabetes mellitus (T2DM) visiting outpatient department of BIDE with a previous history of GDM were recruited. Details were obtained on pre-designed questionnaire after taking informed written consent. A total of 378 women who had a prior history of GDM were included. Mean age (years) was 43.53±10.17. Mostly women were obese (BMI = 30.53±6.08) and have sedentary lifestyle. Mean HbA1c (%) was 9.08±2.24. This study found family history of T2DM and hypertension were common risk factors in women with GDM history. Mostly, women were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
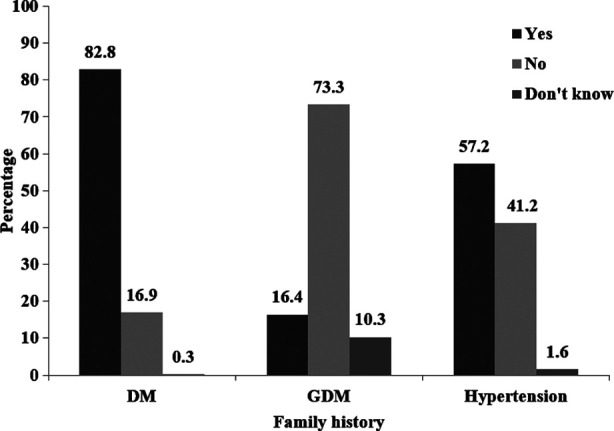 Fig.1
Fig.1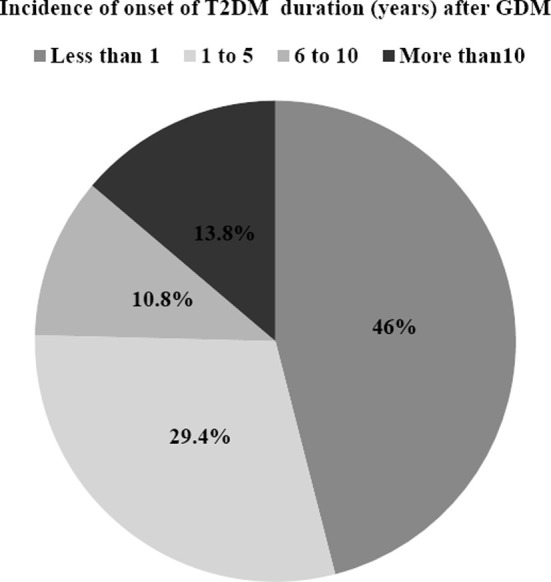 Fig.2
Fig.2| Parameters | n(%) or Mean ± SD |
|---|---|
| N | 378 |
| Age (years) | 43.53±10.17 |
| 25 and under | 4(1.1%) |
| 26 to 35 | 90(23.9%) |
| 36 and over | 283(75.1%) |
| BMI (kg/m2) | 30.53±6.08 |
| Systolic BP (mmHg) | 125.75±18.01 |
| Diastolic BP (mmHg) | 78±12.46 |
| Ethnicity | |
| Urdu speak/Muhajir | 266(70.4%) |
| Punjabi | 24(6.3%) |
| Sindhi | 18(4.8%) |
| Pathan | 47(12.4%) |
| Balochi | 9(2.4%) |
| Others | 14(3.7%) |
| Marital status | |
| Married | 357(94.4%) |
| Divorced/separated | 7(1.9%) |
| Widowed | 14(3.7%) |
| Exercise | |
| Sedentary | 184(48.9%) |
| Light | 128(34%) |
| Moderate | 53(14.1%) |
| Heavy | 11(2.9%) |
| Parameters | n(%) or Mean ± SD |
|---|---|
| N | 378 |
|
| |
| HbA1c (%) | 9.08±2.24 |
| <7% | 32((12.6%) |
| ≥7% | 222(87.4%) |
|
| |
| None | 6(1.6%) |
| Diet | 6(1.6%) |
| OHA | 328(86.8%) |
| insulin | 197(52.1%) |
|
| |
|
| |
| 1st trimester | 71(19.5%) |
| 2nd trimester | 153(42%) |
| 3rd trimester | 140(38.5%) |
|
| |
| 1st | 43(12.5%) |
| 2nd | 50(14.6%) |
| 3rd | 81(23.6%) |
| 4th and above | 169(49.3%) |
|
| |
| Yes | 164(46.5%) |
| No | 189(53.5%) |
|
| |
| Hypertension | 117(31%) |
| Urinary infection | 9(2.4%) |
| Jaundice | 2(0.5%) |
| Others | 17(4.5%) |
| No | 243(64.3%) |
|
| |
| babies alive | 367(97.1%) |
| still births | 95(25.1%) |
| miscarriage | 172(45.9%) |
| surgical abortions | 30(7.9%) |
| Parameters | Less and equal to 5 years | More than 5 years | P-value |
|---|---|---|---|
| n | 285 | 93 | - |
|
| |||
| Age (years) | |||
| 25 and under | 4(1.4%) | 0(0%) | <0.0001 |
| 26 to 35 | 81(28.5%) | 9(9.7%) | |
| 36 and over | 199(70.1%) | 84(90.3%) | |
|
| |||
| Yes | 239(83.9%) | 74(79.6%) | 0.161 |
| No | 46(16.1%) | 18(19.4%) | |
| Do not know | 0(0%) | 1(1.1%) | |
|
| |||
| Yes | 50(17.5%) | 12(12.9%) | 0.080 |
| No | 211(74%) | 66(71%) | |
| Do not know | 24(8.4%) | 15(16.1%) | |
|
| |||
| Yes | 158(56.2%) | 56(60.2%) | 0.670 |
| No | 119(42.3%) | 35(37.6%) | |
| Do not know | 4(1.4%) | 2(2.2%) | |
|
| |||
| <25 | 50(18.2%) | 12(13.2%) | 0.261 |
| ≥25 | 224(81.8%) | 79(86.8%) | |
|
| |||
| <140/90 | 185(67%) | 59(64.8%) | 0.701 |
| ≥140/90 | 91(33%) | 32(35.2%) | |
|
| |||
| <7 | 22(11.3%) | 10(16.9%) | 0.214 |
| 7 to 9 | 87(44.6%) | 30(50.8%) | |
| 10 or above | 86(44.1%) | 19(32.2%) | |
|
| |||
|
| |||
| yes | 147(55.7%) | 17(19.1%) | <0.0001 |
| No | 117(44.3%) | 72(80.9%) | |
| Complications during pregnancy | |||
| Hypertension | 92(32.3%) | 25(26.9%) | 0.038 |
| Urinary infection | 9(3.2%) | 0(0%) | 0.083 |
| Jaundice | 2(0.7%) | 0(0%) | 0.418 |
| Others | 11(3.9%) | 6(6.5%) | 0.295 |
| None | 180(63.2%) | 63(67.7%) | 0.423 |
|
| |||
| 1st trimester | 62(22.6%) | 9(10%) | 0.03 |
| 2nd trimester | 112(40.9%) | 41(45.6%) | |
| 3rd trimester | 100(36.5%) | 40(44.4%) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGestational Diabetes Research and Management · Bariatric Surgery and Outcomes · Pregnancy and preeclampsia studies
INTRODUCTION
Gestational diabetes mellitus (GDM) is an adverse pregnancy complication that carries unique diabetes-related risks and potential long-term consequences for mother and unborn baby. The approximate annual birth complications with hyperglycemia in pregnancy has been reported as 16%.1 GDM has now become a global public health burden that increases the risk of morbidity and mortality, birth traumas, neonatal hypoglycemia, and other severe health problems. It is a significant cause of congenital abnormalities and stillbirths. Annually, stillbirth is estimated to occur in 2.6 million pregnancies worldwide.2
It was also reported that the offspring are potentially at a higher risk of developing obesity, adiposity and disorders of glucose metabolism (insulin resistance and type-2 diabetes) later in life. Cesarean births and pregnancy-related hypertension are more common in women with GDM.3 T2DM is a rising health issue which reduces the life-expectancy as well as survivors’ quality of life.4 Women with GDM are nearly at a 10-fold higher risk of developing T2DM than those with a normoglycemic pregnancy.5
A further systematic review evaluated the rate of compliance with screening, and the prevalence of T2DM in Asian women, reporting incidences rate between 2.8% and 58% in women with previous GDM.6,7 Southeast Asia has the greatest prevalence of GDM, which is estimated to be 24.2%.8 In Bangladesh, the frequency has been reported varying from 13.2% to over 40%, and from 3.8 to 22% in different parts of India depending on the geographical location.9 In Pakistan, the incidence of GDM varies from 4.2 to 26% depending on the region and the diagnostic techniques used.
GDM correlates with age; the incidence of GDM increases by approximately eight times, with an increase in the rate of women giving birth at a more advanced age. Several risk factors including body mass index, family history of diabetes, hypertension, the decrease in physical activity, and the adoption of modern lifestyles contribute to an increase in the prevalence of GDM.10 GDM has serious adverse implications for the health of current and future generations through genetic and environmental mechanisms.11 The condition also places a heavy financial burden on healthcare systems. Limited research has been conducted in Pakistan so far despite its alarming consequences. Therefore, this study was conducted to assess the history of gestational diabetes mellitus and other risk factors in women presenting with Type-2 diabetes mellitus at a tertiary care hospital.
METHODS
This cross-sectional study was conducted at Baqai Institute of Diabetology & Endocrinology (BIDE), a tertiary care hospital of Karachi, Pakistan.
Ethical Approval:
The study was approved by an Institutional Review Board of Dow University of Health Sciences (DUHS) (IRB- 1413/DUHS/Approval/2019).
Inclusion Criteria:
Using consecutive sampling technique, all the women who attended the diabetic outpatient department of BIDE from July 2019 to May 2022, with the history of GDM, were included. GDM was considered if the participants visited with any previous medical history reported by their physician and lab report. Current status of the participants with previous history of GDM were obtained on a pre-designed questionnaire through face-to-face interviews by a trained research officer after obtaining a written informed consent. Women having T1DM, T2DM before pregnancy and with T2DM having no previous history of GDM was excluded.
The proforma included the questions about age, educational background, ethnicity, physical activity, duration of diabetes, family history of T2DM and GDM, previous GDM in earlier pregnancies, and current treatment (oral hypoglycemic agents (OHAs) or insulin). Physical activity include exercise as sedentary (no exercise), light (home chores/little exercise), moderate (brisk walk for 30 minutes), and heavy (exercise > 30 minutes). Any complications during pregnancy like hypertension, urinary infection, jaundice etc. or complication during child birth were also investigated. Questions about stillbirth, miscarriage or abortion were also inquired.
Anthropometric measurements such as height and weight were noted. A calibrated and standardized digital scale was used to measure participants’ weight in kilograms (kg). Participants were weighed in light clothing and were also asked to remove shoes and socks. The height was measured with the help of a stadiometer in centimeter (cm). Participants were asked to remove shoes and stand straight in an upright position along their back towards wall. Body Mass Index (BMI) kg/m² was calculated by dividing weight (kg) by squared height (m). BMI was classified as per Asian-Pacific cutoff points as normal 18.5–22.9kg/m^2^, overweight 23.0– 24.9kg/m^2^ and obesity ≥25 kg/m^2^.12 Blood pressure was measured with mercury sphygmomanometer. Participants were requested to take 10 minutes rest in a sitting position before measurement of blood pressure to reduce variation. Mean of two readings were used in the study. Blood pressure <140/90mmHg was considered as normal and high blood pressure was considered as blood pressure ≥140/90mmHg.13 HbA1c was analyzed by high-performance liquid chromatography method using Bio-Rad D-10. HbA1c <7% was considered best control, and seven and above as uncontrolled glycemic or poor control.14
Statistical Analysis:
Analyses were performed using Statistical Package for Social Sciences (SPSS version 20.0). For continuous variables, statistics included n (number of observation), mean, standard deviation, as well as frequencies and percentages for categorical variables. P-value <0.05 considered as statistically significant.
RESULTS
A total of 378 women who had a prior history of GDM were included. Current status of baseline characteristics of the study participants is presented in Table-I. Mean age (years) was 43.53±10.17. Among these, 4(1.1%) women were below 25 years, 90(23.9%) were between 26 to 35 years and 283(75.1%) women were ≥ 36 years. Mean BMI was 30.53±6.08(kg/m^2^) and systolic/diastolic blood pressure (mmHg) was 125.75±18.01/78±12.46. Most of the women had sedentary lifestyle. The current status of glycemic index and medical history related to GDM is shown in Table-II. Current status of mean HbA1c (%) was found to be 9.08±2.24 (12.6% were observed with <7% HbA1c and 87.4% were found with ≥ 7% HbA1c). Majority of women were being treated with OHA for type-2 diabetes after GDM. Upon asking previous history it was found that mostly, women were diagnosed as GDM during second trimester (42%) and was mainly seen in multiparous women (occur in fourth and above pregnancy). Around 46.5% women used insulin during pregnancy. Hypertension was the common complication during pregnancy 117(31%).
Frequency of potential familial associated risk factors are shown in Fig.1. It was noted that most of the women had family history of T2DM (82.8%) and family history of hypertension (57.2%) as common associated risk factors. Family history of GDM was reported in 16.4% women. The onset of T2DM from GDM is presented in Fig.2. It was found that 46% women developed T2DM within one year of GDM diagnosis, 29.6% between one to five years and 10.8% between six to ten years duration.
Frequency of associated familial risk factors for GDMDM: diabetes mellitus, GDM: gestational diabetes mellitus.
Incidence of onset of T2DM duration (years) after GDM.GDM: gestational diabetes mellitus, T2DM: type-2 diabetes mellitus.
Association of potential risk factors of participants with current status and previous history with duration of T2DM from GDM are shown in Table-III. Current status of women who developed T2DM from GDM suggesting that age (p-value <0.0001) and family history of diabetes (p-value = 0.034) are statistically significantly potential associated risk factor, while history of GDM suggesting that insulin use during pregnancy (p-value <0.0001), trimester of GDM diagnosis (p-value=0.03), and hypertension during pregnancy (p-value=0.038) are also the significantly potential associated risk factors in developing T2DM from GDM.
DISCUSSION
The onset of T2DM from GDM in majority of women was within five years of diagnosis. GDM to T2DM implies a possible complication after postpartum. Early progression of T2DM with GDM history consistent to Bengtson et al. who reported that up to 50% of women with history of GDM progress to T2DM within five years of postpartum.15 Our findings are also in agreement with Kim et al. study who showed a higher cumulative incidence of T2DM in the first five postpartum years.16
It was earlier studied that genetic and behavioral factors are involved with family history of hypertension and diabetes and in women it may be predisposed to an increased preeclampsia risk.10 In this study, we found a family history of T2DM and hypertension are the common associated risk factors in GDM women progressing to T2DM. We also found hypertension as a complication during pregnancy was significantly high in women with below five years duration of diabetes progression. Lee et al reported that women had rising trend of hypertension during pregnancy.17 Our results are in consistent with Li et al who found an association between GDM and family history of diabetes mellitus.18 Our findings are also in agreement with Wagan et al who reported family history of diabetes mellitus and age as a classic risk factors associated with less than five years duration of GDM progression to T2DM.19 Risk of GDM increases with increasing age is in line with Vounzoulaki et al. study.4
Similar to previous reported data, insulin use during pregnancy is also the significant potential associated risk factor in women with less duration of GDM onset to T2DM.20 Noctor et al. and Dunne et al. also reported that women with use of insulin during pregnancy were more prone of future progression to diabetes and/or abnormal glucose tolerance.20 We found most of the women with GDM diagnosis in second trimester and were multiparous women (occur in fourth and above pregnancy). However, Brand et al reported that women who diagnosed with a third trimester were usually older, obese, having hypertensive disorder of pregnancy and were more often multiparous.21 According to recent estimates in Pakistan 58% women had generalized obesity and 62.7% had central obesity that have a pivotal role in GDM and T2DM development.12,22 Literature suggest that after pregnancy 7% increment occur in weight.23 We also found most of the women in current state were overweight and or obese that can be significantly associated to an increase in the number of T2DM.24 Though, we found non-significant results for BMI with duration of diabetes. However, urgent lifestyle modification strategies to manage this high risk cardio metabolic risk factor are necessary.25
It was noted that number of women were not checking blood glucose levels after delivery which may results in late diagnosis of T2DM. So, it is important to regularly monitor blood glucose levels post-partum so that diagnosis of T2DM is not delayed and early management can be started.26 Our results also suggest that women who are at high risk should use their worthwhile time window for preventing GDM progression to T2DM and prioritized preventative interventions such as diet, physical activity, breastfeeding and postpartum weight management.27 In consequence, free-of-cost GDM screening and postpartum diabetes screening awareness programs are needed and dietary and lifestyle interventions can be a significant step towards diabetes prevention and related complications in this region of the world to overcome the burden of diabetes. Education session regarding importance of breastfeeding and weight management in women with history of GDM should also be the necessary steps.28 Future researches are required across heterogeneous populations to evaluate the effectiveness and cost effectiveness of preventive interventions over long term period.
Strengths and Limitations:
We used a consecutive sampling method; a single centered and recall bias are the limitations. However, reporting duration and long term risk factors of T2DM progression in women with history of GDM in Pakistan is strength of this study.
CONCLUSION
Majority of women with GDM developed T2DM within five years of diagnosis. The potential associated risk factors were age, family history of diabetes, insulin use during pregnancy, trimester of GDM diagnosis, and hypertension during pregnancy. These findings suggest a need for epidemiological studies in developing countries. Awareness and life style modifications along with regular post-partum follow up with screening for T2DM should be part of GDM management to prevent or delay the occurrence of this serious complication.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zhao D Yuan S Ma Y An YX Yang YX Yang JK Associations of maternal hyperglycemia in the second and third trimesters of pregnancy with prematurity Medicine (Baltimore)20209917 e 19663 doi:10.1097/MD.00000000000196633233261010.1097/MD.0000000000019663 PMC 7220749 · doi ↗ · pubmed ↗
- 2Aminu Mvan den Broek N Stillbirth in low-and middle-income countries:addressing the ‘silent epidemic’Int Health 2019114237239 doi:10.1093/inthealth/ihz 0153108189310.1093/inthealth/ihz 015PMC 6635884 · doi ↗ · pubmed ↗
- 3Auvinen AM Luiro K Jokelainen JJärveläI Knip M Auvinen J Type-1 and Type-2 diabetes after gestational diabetes:a 23-years cohort study Diabetologia 2020631021232128 doi:10.1007/s 00125-020-05215-33272528010.1007/s 00125-020-05215-3PMC 7476985 · doi ↗ · pubmed ↗
- 4Vounzoulaki E Khunti K Abner SC Tan BK Davies MJ Gillies CL Progression to type-2 diabetes in women with a known history of gestational diabetes:systematic review and meta-analysis BMJ 202013369373 doi:10.1136/bmj.m 136110.1136/bmj.m 1361 PMC 721870832404325 · doi ↗ · pubmed ↗
- 5Diaz-Santana MVO'Brien KM Park YM Sandler DP Weinberg CR Persistence of risk for type 2 diabetes after gestational diabetes mellitus Diabetes Care 2022454864870 doi:10.2337/dc 21-14303510432510.2337/dc 21-1430 PMC 9016728 · doi ↗ · pubmed ↗
- 6Wali AS Rafique R Iftikhar S Ambreen R Yakoob MY High proportion of overt diabetes mellitus in pregnancy and missed opportunity for early detection of diabetes at a tertiary care centre in Pakistan Pak J Med Sci 20203613843 doi:10.12669/pjms.36. ICON-Suppl.172310.12669/pjms.36.ICON-Suppl.1723 PMC 694310331933605 · doi ↗ · pubmed ↗
- 7Riaz M Nawaz A Masood SN Fawwad A Basit A Shera AS Frequency of gestational diabetes mellitus using DIPSI criteria, a study from Pakistan Clin Epidemiol Glob Health 201972218221 doi:10.1016/j.cegh.2018.06.003
- 8Singh A Rai YK Misra A Rathi P Gupta S Prevalence of Gestational diabetes mellitus in NCR, India Eur J Mol Clin Med 2022903 Available on: https://go.gale.com/ps/i.do?id