A Systematic Review of Perinuclear Antineutrophil Cytoplasmic Antibody-Associated Glomerulonephritis Following Coronavirus Disease 2019 Vaccination: A 2024 Update
Ikponmwosa J Ogieuhi, FNU Suman, Nikita Kumari, Bai Manita, Dinkey Kumari, Joti Devi, Mohamed Abdalla, Eithar Shabbo, Utsav Patel, Iqra Samreen, Khalid H Mohamed, Zahoor Ahmed, Hira Nasir

TL;DR
This study reviews cases of a rare kidney disease linked to the immune system that occurred in some people after receiving a COVID-19 vaccine.
Contribution
The paper provides a 2024 update on the rare occurrence of p-ANCA-associated glomerulonephritis following COVID-19 vaccination.
Findings
35 cases of p-ANCA GN were reported after vaccination, with most patients responding well to treatment.
The mRNA vaccines were most commonly associated with this condition, and symptoms typically appeared after the second dose.
Most patients achieved remission, but a small number required dialysis or experienced relapse.
Abstract
Antineutrophil cytoplasmic antibody (ANCA)-associated glomerulonephritis (GN) is an immune-mediated kidney disease characterized by the inflammation of small blood vessels in the kidney, leading to renal impairment and potentially irreversible damage. Concerns have been raised over the reports of myeloperoxidase/perinuclear (MPO/p) ANCA GN following the coronavirus disease 2019 (COVID-19) vaccination. Our study provides a comprehensive insight into perinuclear anti-neutrophil cytoplasmic antibodies (p-ANCA) GN after COVID-19 vaccination. We conducted a comprehensive literature search on PubMed, Cochrane Library, and EMBASE using the Medical Subject Headings (MeSH) terms related to “covid-19 vaccine,” “glomerulonephritis,” “p-ANCA,” and “MPO-ANCA” up to March 5, 2024, to include cases of p-ANCA-associated GN following COVID-19 vaccination. Of the 4,102 articles, we included 29,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
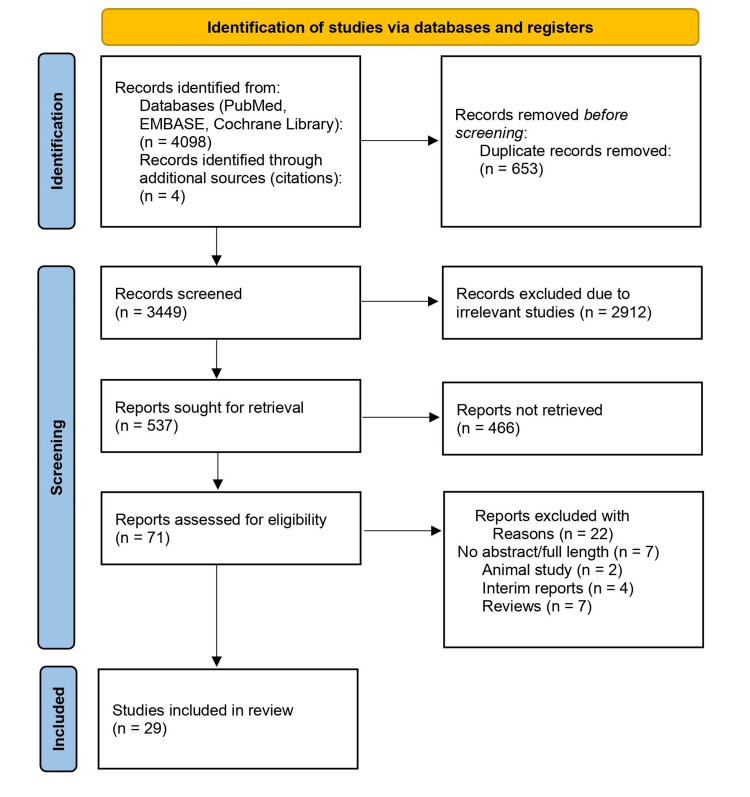 Figure 1
Figure 1| Viral component | Type of vaccine |
| Viral vector component | AstraZeneca |
| Sputnik V | |
| Johnson’s Janssen | |
| mRNA component | Pfizer-BioNTech |
| Moderna | |
| Protein subunit | Novavax |
| Side effect | Number | % |
| Injection-site pain | 7,734 | 77.34 |
| Fatigue | 4,300 | 43.00 |
| Myalgia | 3,967 | 39.67 |
| Local swelling | 3,357 | 33.57 |
| Headache | 3,327 | 33.27 |
| Authors | Age/Sex | Medical history | Vaccine type | Vaccine dose | New case/Relapse | Onset (days) | Symptoms | Hematuria | Baseline creatinine | Peak serum creatinine (mg/dL) | Urine protein | Extrarenal involvement | Diagnosis on biopsy | ANCA serologies | Treatment | Kidney pathology | Outcome |
| Uddin et al. [ | 59/M | HTN, IHD | Pfizer | Second | New | 17 | Fever, malaise, arthralgia | 1+ | NA | 3.5 | 2+ | NA | Yes | p-ANCA | Methylprednisolone, rituximab | Glomerulosclerosis, interstitial scarring | Remission |
| Javadian et al. [ | 32/F | NA | Sinopharm | Second | New | 17 | Fever, malaise, myalgia, fatigue | 2+ | NA | 3.5 | 2+ | Interstitial pneumonia | No | p-ANCA | Tocilizumab, plasmapheresis | No | Remission |
| El Hasbani et al. [ | 47/F | NA | Pfizer | First | New | 3 | Flank pain, hematuria, edema | 2+ | 0.8 | 2.1 | 1+ | NA | Yes | p-ANCA | Methylprednisolone | Crescentic GN, diffuse sclerosis | Remission |
| Gen et al. [ | 82/F | NA | Moderna | Third | New | 30 | Fever, malaise, hematuria, proteinuria | 1+ | 0.73 | 1.4 | 1+ | NA | Yes | p-ANCA | Prednisolone | Crescentic GN, rapidly progressive GN | Remission |
| Mazza et al. [ | 71/M | IHD | Pfizer | Third | New | 21 | Fever, hematuria | 1+ | 0.91 | 2.1 | 2+ | NA | Yes | p-ANCA | Dialysis, rituximab, steroids | Crescentic GN | Remission |
| Yoshino et al. [ | 56/M | NA | Pfizer | Second | New | 42 | Vomiting, abdominal pain | 2+ | 0.83 | 1.07 | 2+ | Aortitis, neuropathy | Yes | p-ANCA | Methylprednisolone, cyclophosphamide | Fibrinoid necrosis, Crescentic GN | Remission |
| Ting et al. [ | 63/F | Asthma | Pfizer | First | New | 27 | Renopulmonary syndrome | 1+ | NA | 7.02 | 3+ | NA | Yes | p-ANCA/c-ANCA | Steroids, cyclophosphamide, plasmapheresis | Crescentic GN | Remission |
| 51/M | HTN, HF | Pfizer | First | New | 21 | Renopulmonary syndrome | 2+ | NA | 31.4 | 1+ | NA | Yes | p-ANCA/c-ANCA | Steroids, cyclophosphamide, plasmapheresis | Crescentic GN | Remission with relapse | |
| 62/F | NA | Pfizer | First | New | 28 | Renopulmonary syndrome | 1+ | NA | 7.3 | 1+ | NA | Yes | p-ANCA/c-ANCA | Steroids, cyclophosphamide, plasmapheresis | Segmental GN | Remission with Relapse | |
| 70/M | HTN, DM, IHD | Moderna | Second | New | 42 | AKI | 1+ | NA | 6.7 | 3+ | NA | Yes | p-ANCA/c-ANCA | Steroids, cyclophosphamide, plasmapheresis | Fibrinoid necrosis, AIN | Remission | |
| Kawamura et al. [ | 71/F | NA | Pfizer | Third | New | 19 | Fever, malaise, AKI | 1+ | 0.71 | 3.5 | 2+ | Interstitial pneumonia | Yes | p-ANCA | Steroids | AIN, fibrinoid necrosis | Remission |
| Baier et al. [ | 57/F | NA | Pfizer | Third | New | 5 | Dyspnea, hemoptysis | NA | NA | NA | NA | Pulmonary hemorrhage | No | p-ANCA | Steroids | NR | Remission |
| Chen et al. [ | 70/F | NA | Moderna | First | New | 21 | Hematuria, hemoptysis, AKI | 3+ | 1 | 3.5 | 3+ | Bilateral peri bronchial consolidation | Yes | p-ANCA | Steroids, rituximab, plasmapheresis | Crescentic GN, vasculitis | Remission |
| Cai et al. [ | 54/F | Polyarthritis, OM | Pfizer | Second | New | 14 | Constitutional symptoms, Episcleritis, edema | 4+ | NA | 2.1 | 4+ | Eye involvement, discreet opacities in both lungs | Yes | p-ANCA | Steroids, rituximab | Crescentic GN | Remission |
| Dube et al. [ | 29/F | CF | Pfizer | Second | New | 16 | AKI, nephritis | 3+ | 0.8 | 1.9 | NA | No | Yes | p-ANCA | Steroids, cyclophosphamide | Crescentic GN, fibrocellular crescentic GN, glomerulosclerosis, mild AIN | Remission |
| Hakroush et al. [ | 79/F | HTN | Pfizer | Second | New | 14 | Weakness, Thigh pain | 2+ | 0.7 | 6.6 | 4+ | Rhabdomyolysis | Yes | p-ANCA | Steroids, cyclophosphamide | Crescentic GN, glomerulosclerosis, ATN, AIN | Remission |
| Schaubshlager et al. [ | 77/F | HTN | Moderna | Second | New | 84 | AKI | NA | 0.9 | 2.9 | NA | No | Yes | p-ANCA | Steroids, Rituximab | Crescentic GN, fibrocellular crescentic GN, glomerulosclerosis, fibrinoid necrosis | Remission |
| Shakoor et al. [ | 78/F | HTN | Pfizer | Second | New/Follow-up | 12 | Nausea, vomiting, diarrhea | 3+ | 0.8 | 1.3/3.5 | 2+ | No | No | p-ANCA | No treatment/Steroids, rituximab | Crescentic GN, fibrinoid necrosis, AIN | Remission with relapse |
| Villa et al. [ | 63/M | NA | AstraZeneca | First | New | 7 | Hemoptysis, rapidly progressive GN | 2+ | Normal | 2.9 | 2+ | Interstitial pneumonia | Yes | p-ANCA | Steroids, cyclophosphamide | Crescentic GN | Remission |
| David et al. [ | 75/M | NA | AstraZeneca | First | Follow-up | 35 | Hemoptysis | 3+ | 2.6 | 7 | 3+ | Pulmonary hemorrhage | Yes | p-ANCA | Steroids, rituximab, Hemodialysis | Crescentic GN | Dialysis |
| 74/M | NA | AstraZeneca | Second | New | 14 | AKI | NA | 0.9 | 10 | NA | No | Yes | p-ANCA | Steroids, cyclophosphamide, hemodialysis | Crescentic GN with vasculitis | Remission | |
| Sekar et al. [ | 47/F | NA | Pfizer | First | New | 3 | Flank pain, weakness | 3+ | 0.8 | 2.9 | NA | No | Yes | p-ANCA | Steroids, Azathioprine | fGN | Remission |
| Kim et al. [ | 72/F | NA | Moderna | Third | New | 18 | Constitutional symptoms, AKI | NA | 0.8 | 4.7 | +3 | Otologic symptoms, gastritis | Yes | p-ANCA | Steroids, cyclophosphamide | fibrocellular crescentic GN, glomerulosclerosis, AIN | Remission |
| Loo et al. [ | 75/F | HF | Moderna | First | New | 77 | AKI | NA | NA | 6.3 | 2+ | No | Yes | p-ANCA | Steroids, rituximab, hemodialysis | Crescentic GN | Remission |
| Ma et al. [ | 70/F | HTN, dyslipidemia | CoronaVac | First | New | 10 | Constitutional symptoms, foamy urine | NA | 0.5 | 5.4 | 2+ | No | Yes | p-ANCA | Steroids, cyclophosphamide | Crescentic GN, fibrocellular crescentic GN, fGN | Remission |
| Noel et al. [ | 62/F | SSC, HTN, DM | Pfizer | Second | New | 28 | AKI | 3+ | 1.0 | 5.2 | NA | No | Yes | p-ANCA | Steroids, cyclophosphamide, mycophenolate mofetil | Crescentic GN, fibrocellular crescentic GN | Remission |
| Obata et al. [ | 84/M | Stroke | Pfizer | Second | New | 14 | Constitutional symptoms, cough | 3+ | 1.2 | 1.2 | 1+ | Interstitial pneumonia | Yes | p-ANCA | Steroids | Crescentic GN, glomerulosclerosis, fibrinoid necrosis | Remission |
| Ramezanzade et al. [ | 15/M | NA | Sinopharm | Second | New/follow-up | 30 | Constitutional symptoms, flank pain, nausea | 4+ | NA | 3 | 3+ | No | Yes | p-ANCA | Steroids, mycophenolate mofetil | Crescentic GN, necrotizing GN, ATN | Remission with relapse |
| So et al. [ | 42/M | NA | Pfizer | Second | New | 63 | Constitutional symptoms, gross hematuria | NA | 1.0 | 3.1 | 4+ | No | Yes | p-ANCA | Steroids, rituximab, PEX | Crescentic GN, fGN, mild interstitial infiltration | Remission |
| Suzuki et al. [ | 72/M | Prostatic hypertrophy | Pfizer | Second | New | 1 | Constitutional symptoms, AKI | 3+ | Normal | 7.4 | 1+ | No | Yes | p-ANCA | Steroids, rituximab, hemodialysis | Crescentic GN, segmental necrosis, fibrinoid necrosis | Remission |
| Zamoner et al. [ | 58/F | Hypothyroidism | AstraZeneca | First | New | 5 | Constitutional symptoms, foamy urine, arthralgia | 1+ | NA | 2.2 | 4+ | No | Yes | p-ANCA | Steroids, cyclophosphamide, azathioprine | crescentic GN, fibrocellular crescentic GN, fGN | Remission |
| Bansal et al. [ | 67/F | HTN | Covaxin/BBV152 | Second | New | 14 | Edema, nausea, vomiting, decreased appetite | NA | 1.2 | 6.4 | 3+ | No | Yes | p-ANCA | Steroids, cyclophosphamide, hemodialysis | Fibrinoid necrosis, focal GN, crescentic GN | Remission |
| Thammathiwat et al. [ | 76/F | DM, HTN, dyslipidemia | AstraZeneca | Second | New | 20 | Fever, weight loss, cough, edema | 2+ | 1.5 | 3.5 | 2+ | Interstitial pneumonia | Yes | p-ANCA | Steroids, cyclophosphamide, Hemodialysis | Glomerulosclerosis, crescentic GN | Dialysis |
| 69/F | HTN | Pfizer | Third | New | 28 | Constitutional symptoms, AKI, hearing loss | 1+ | 0.7 | 7.1 | 4+ | Sensorineural hearing loss | Yes | p-ANCA | Steroids, cyclophosphamide, plasmapheresis | AIN, crescentic GN | Remission | |
| 84/F | HTN, dyslipidemia | Moderna | Third | New | 30 | Constitutional symptoms, AKI, | 1+ | 0.9 | 5.1 | 3+ | Optic neuritis, valerian degeneration | Yes | p-ANCA | Steroids, IV immunoglobulin, hemodialysis | AIN, Fibrinoid necrosis, crescentic GN | Remission |
| Characteristics | Mean | SD |
| Age (years) | 63.22 | 16.00 |
| Sex | N | % |
| Male | 12 | 34.3% |
| Female | 23 | 65.7% |
| Past medical history | ||
| Hypertension | 13 | 37.14% |
| Diabetes mellitus | 3 | 8.6% |
| Kidney disease | 2 | 5.7% |
| No history/Not reported | 15 | 42.9% |
| Vaccine type | N | % |
| Pfizer | 19 | 54.28 |
| Moderna | 7 | 20 |
| AstraZeneca | 5 | 14.28 |
| Sinopharm | 2 | 5.7 |
| CoronaVac | 1 | 2.9 |
| Covaxin | 1 | 2.9 |
| mRNA vaccine | 26 | 74.28 |
| Inactivated vaccine | 4 | 11.42 |
| Adenovirus vector vaccine | 5 | 14.28 |
| Vaccine dose | ||
| First | 11 | 31.43 |
| Second | 17 | 48.57 |
| Third | 7 | 20 |
| Days to first symptom onset | ||
| Day <2 | 1 | 5.7 |
| Day 2–7 | 5 | 14.28 |
| Day >7 | 29 | 82.86 |
| Symptoms | N | % |
| Acute kidney injury | 15 | 42.85 |
| Constitutional symptoms | 19 | 54.28 |
| Edema | 3 | 8.52 |
| Hemoptysis | 4 | 11.42 |
| Renopulmonary syndrome | 3 | 8.52 |
| Extrarenal manifestations | ||
| Lung (interstitial pneumonia, pulmonary hemorrhage) | 7 | 20 |
| Gastrointestinal | 1 | 2.86 |
| Eye | 2 | 5.71 |
| Neuromuscular | 3 | 8.57 |
| ENT | 2 | 5.71 |
| Renal function test parameter | ||
| Serum creatinine (mg/dL) | ||
| Mean baseline | 0.96; SD = ±0.39 | |
| Mean peak | 4.98; SD = ±5.02 | |
| N | % | |
| Proteinuria | ||
| Grade ≤2 | 16 | 45.71 |
| Grade >2 | 13 | 37.14 |
| Hematuria | ||
| Grade ≤2 | 17 | 48.57 |
| Grade >2 | 10 | 28.57 |
| ANCA serologies | N | % |
| MPO/ANCA (p-ANCA) | 31 | 88.6 |
| p-ANCA + c-ANCA (dual positive) | 4 | 11.4 |
| Histopathology findings | ||
| Crescentic GN | 27 | 77.14 |
| Fibrocellular crescentic GN | 6 | 17.14 |
| Glomerulosclerosis | 8 | 22.86 |
| Acute interstitial nephritis | 8 | 22.86 |
| Fibrinoid necroses | 9 | 25.71 |
| Used treatment | N | % |
| Steroids | 30 | 85.71 |
| Rituximab | 10 | 28.57 |
| Plasmapheresis | 8 | 22.86 |
| Dialysis | 10 | 28.57 |
| Treatment outcomes | ||
| Remission | 29 | 82.86 |
| Remission with relapse | 4 | 11.42 |
| Maintenance dialysis | 2 | 5.72 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSARS-CoV-2 and COVID-19 Research · Vasculitis and related conditions · Heparin-Induced Thrombocytopenia and Thrombosis
Introduction and background
The rapid development and deployment of the coronavirus disease 2019 (COVID-19) vaccines against the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have represented a significant milestone in the global effort to mitigate the COVID-19 pandemic [1]. These vaccines have shown promising results in preventing severe morbidity, viral transmission, and mortality. Although COVID-19 vaccines have established efficacy, continuous evaluation and monitoring of potential adverse events related to the COVID-19 vaccine are warranted to ensure the vaccine’s safety profile. Many vaccines have been developed against COVID-19 viral components, including mRNA, protein subunits, or viral vectors (Table 1) [2,3].
Although each vaccine has shown promising results in preventing viral transmission and reducing the severity of the disease, vaccine-associated side effects and complications have also been highlighted. The reported complications depend on the dosing and type of the COVID-19 vaccine. The most reported side effects include injection-site pain, headache, myalgia, fatigue, malaise, and flu-like symptoms (Table 2) [4].
COVID-19 vaccine can potentially affect any body organ system, and involvement of gastrointestinal, cardiovascular, and nervous systems has also been reported [5,6]. Renal complications of the COVID-19 vaccine, including acute kidney injury (AKI), glomerulonephritis (GN), acute interstitial nephritis, minimal change disease, and renal failure, have also been published [7]. Antineutrophil cytoplasmic antibody (ANCA)-associated GN is a devastating and noteworthy adverse event of the COVID-19 vaccine that is rarely reported [8].
ANCA GN is an immune-mediated kidney disease characterized by the inflammation of small blood vessels in the kidney, leading to renal impairment and potentially irreversible damage [9]. There are two types of ANCA GN based on the staining pattern on indirect immunofluorescence microscopy: cytoplasmic ANCA (c-ANCA) and perinuclear ANCA (p-ANCA). In c-ANCA, the primary antigen target is proteinase 3 (PR3), and myeloperoxidase (MPO) is the main antigen target in p-ANCA. COVID-19 vaccine has been reported to induce both types of ANCA GN [10]. p-ANCA GN is commonly associated with microscopic polyangiitis, drug-induced vasculitis, and eosinophilic granulomatosis with polyangiitis. Recent reports have provided a possible link between the COVID-19 vaccine and developing p-ANCA GN [11,12]. This systematic review provides detailed insights to consolidate and analyze the evidence of p-ANCA GN as an adverse event of the COVID-19 vaccine.
Review
Methodology
We conducted a systemic and comprehensive literature search following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol to ensure transparency in the search process (Figure 1) [13]. We conducted an initial search using major databases, including PubMed, Cochrane Library, and EMBASE. We used the Medical Subject Headings (MeSH) terms and keywords related to “COVID-19 vaccine,” “glomerulonephritis,” “p-ANCA,” and “MPO-ANCA” with the date of inception to March 5, 2024. We conducted our search without any language or geographical restrictions. Additionally, we also screened the references of included studies to identify all pertinent articles. We imported all citations to EndNote version 12.0 for comprehensive screening and extracting relevant data. Exclusion criteria involved studies non-relevant to COVID-19 vaccine-associated p-ANCA GN, review articles, editorials, and animal studies.
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart.
Based on the initial search, 4,102 articles were extracted, and two authors independently screened the titles and abstracts of the articles based on inclusion and exclusion criteria. Two authors assessed the eligibility of full-text articles of potentially relevant studies. Two independent authors evaluated the quality of the included studies based on the critical appraisal tool of the Joanna Briggs Institute for case studies. Relevant data, including study characteristics (author and publication year), patient demographics (age and sex), previous medical history, COVID-19 vaccine type, vaccine dose, time to onset of p-ANCA associated glomerulonephritis following vaccination, clinical presentation, laboratory findings, histopathological features, treatment modalities, and clinical outcomes was extracted from the eligible studies on pre-defined Microsoft Excel (Microsoft Corp., Redmond, WA, USA) datasheet. Data were extracted by two independent authors, and SPSS version 23.0 (IBM Corp., Armonk, NY, USA) was applied to demonstrate the numerical data as mean and standard deviation (SD) and categorical data as proportions (%). Discrepancies were solved through discussion and mutual consensus. A Measurement Tool to Assess Systematic Reviews 2 tool was used to assess the quality of our study [14].
Results
Of the 4,102 articles, 71 were assessed for eligibility, and 29 articles, including case reports and case series, were included in the review, reporting 35 patients with COVID-19 vaccine-induced p-ANCA GN. Each study’s characteristics (author and publication year), patient demographics (age and sex), previous medical history, COVID-19 vaccine type, vaccine dose, time to onset of p-ANCA-associated GN post-vaccination, clinical presentation, laboratory findings, histopathological features, treatment modalities, and clinical outcomes are tabulated in Table 3 [8,10-12,15-39].
In our study, 23 (65.7%) were females, and 12 (34.3%) patients were male with a median age of 69 years (mean ± SD = 63.22 ± 16). Thirteen patients reported hypertension as a previous medical history, and two patients had a history of kidney disease on initial presentation (Table 4).
Our study also revealed that among the patients with COVID-19 vaccine-induced p-ANCA GN, 19 (54.28%) received Pfizer, and seven (20%) received the Moderna vaccine. Twenty-six (74.28%) patients received the mRNA vaccine (Pfizer plus Moderna), and four (11.42%) patients received the inactivated COVID-19 vaccine. Regardless of the type of the COVID-19 vaccine, 17 (48.57%) patients presented with p-ANCA GN after the second dose of the COVID-19 vaccine, and 11 (31.43%) patients presented after the first dose of the COVID-19 vaccine. Most cases presented with a median gap of 19 days (range = 1-84), and the majority of the patients (82.86%) presented after seven days of receiving the COVID-19 vaccine (Table 5).
Constitutional symptoms (fever, malaise, myalgia, nausea, and vomiting) were the most reported manifestations in patients with vaccine-induced p-ANCA GN (54.28%), followed by AKI (42.85%), with 15 (42.85%) patients presented with extrarenal manifestations of p-ANCA (Table 6). Among laboratory findings, the mean baseline serum creatinine was 0.96 ± 0.39 mg/dL, and the mean peak serum creatinine was 4.98 ± 5.02 mg/dL. Hematuria was present in 27 (77.14%) patients, and protein urea was present in 29 (82.85%) patients (Table 7).
On serological testing, MPO/p-ANCA was positive in 31 (88.6%) patients, and dual-positive ANCA was detected in four (11.4%) patients. All patients were diagnosed with biopsy, and crescentic GN was the most common finding reported in 27 (77.14%) patients, followed by fibrinoid necrosis (25.71) (Table 8).
All patients were managed in accordance with the Kidney Disease Improving Global Outcomes 2021 guidelines for the management of glomerular diseases [41]. Steroids were prescribed in 30 (85.71%) patients, followed by rituximab (28.57%) and plasmapheresis (22.86%). Most patients responded well to treatment, and 29 (82.86%) patients achieved complete remission and relapse in four (11.42%) patients. Two patients were hemodialysis-dependent in non-remission, with no mortality reported (Table 9).
Discussion
Considering the ongoing emerging data between the COVID-19 vaccine and kidney diseases, public concerns have risen regarding the potential kidney adverse events. COVID-19 vaccine-associated renal complications include AKI, acute interstitial nephritis, minimal change disease, renal vasculitis, immunoglobulin A nephropathy, and membranous nephropathy [7]. p-ANCA GN is a life-threatening complication of the COVID-19 vaccine, which is not widely reported [14]. A systematic review of renal side effects of the COVID-19 vaccine reported only 16 patients of ANCA out of 128 patients. Seven of the 16 patients were diagnosed with p-ANCA GN triggered by the COVID-19 vaccine. Most patients presented with constitutional symptoms and acute kidney disease after the second dose of the COVID-19 vaccine, with a median onset time of 14 days, consistent with our study’s result [7]. Campos et al. [40] reported 11 cases of p-ANCA GN following the COVID-19 vaccine, and mRNA vaccines were the main culprits in triggering GN. Of the 11 cases, nine were female, and the patients presented with non-specific symptoms with an average of 18 days of the vaccine. All patients responded to treatment except for two who remained on dialysis [41]. Thammathiwat et al. reported a case series of three patients who presented with non-specific symptoms and AKI following the COVID-19 vaccine. After laboratory evaluations and biopsy findings, the patients were diagnosed with p-ANCA GN induced by the COVID-19 vaccine. Immunosuppressant therapy and plasmapheresis resulted in complete remission [8].
Our study revealed that COVID-19 vaccine-induced p-ANCA GN was predominant in females with a median age of 69 years, and hypertension was the most common comorbidity among these patients, consistent with published data and highlighting the importance of considering underlying medical conditions in the context of vaccine-related side effects. Our study also highlighted that the Pfizer vaccine was most frequently implicated in p-ANCA GN, and the majority of cases occurred after the second dose of the COVID-19 vaccine, consistent with other studies. This temporal association underscores the need to closely monitor patients following vaccination and promptly evaluate any concerning symptoms. Clinical presentations and laboratory findings revealed characteristic features of renal involvement, including elevated renal function tests, hematuria, and proteinuria. Serological testing demonstrated positivity for p-ANCA in patients, suggesting an autoimmune etiology of the disease, and histopathological examination of renal biopsies further supported the diagnosis of p-ANCA GN. Patients in our study were managed following the treatment guidelines for glomerular diseases, focusing on immunosuppressive therapy. Most patients responded well to treatment, with a high proportion achieving complete remission. Despite the favorable treatment response in the majority of patients, a subset of patients experienced relapse, emphasizing the extended monitoring and management of vaccine-induced p-ANCA GN [8].
COVID-19 vaccines, especially mRNA vaccines, have been linked to an increased prevalence of p-ANCA GN, mainly due to their high immunogenicity and global use [7,42]. Lipid-based nanoparticles of mRNA COVID-19 vaccines induce activation of CD4+ and CD8+ T-cell lymphocytes and enhance an increased production of B cells in the germinal centers, leading to increased secretion of inflammatory mediators, such as interferons and interleukin-2 (IL-2). DNA adenoviral vaccine induces CD4+ and CD8+ cytotoxic T cells and induces B-cell lymphocytes to enhance antibody production, mainly immunoglobulins G1-G4. Viral spike proteins have also been linked to glomerular injury [43].
Compared to drug-induced ANCA GN, COVID-19 vaccine-induced ANCA GN presents a remarkably shorter median onset, often occurring after second or booster doses of the COVID-19 vaccine, suggesting a potential booster effect, contributing to a higher absolute risk of GN [8]. The underlying mechanism of vaccine-induced ANCA GN remains undefined. It is postulated that antiviral-neutralizing antibodies may induce an autoimmune response, resulting in ANCA production [11,44]. Another mechanism may involve molecular mimicry activating B and T cells via Toll-like receptors and causing a robust immune response, potentially priming ANCA production. Furthermore, an innate immune response triggered by vaccine adjuvants such as factor MF59 in the AstraZeneca COVID-19 vaccine may also contribute to developing immune-mediated GN [9,45]. Additionally, immune response results in a cascade of inflammatory events by inflammatory cytokines, including IL-6, interferon-gamma, and the formation of neutrophil extracellular traps containing MPO and PR3, further mediating glomerular injury. The interplay between COVID-19 vaccine-induced ANCA GN and autoantibodies suggests a complex relationship that warrants further exploration [20].
Our study has many implications for public health policy, vaccination strategies, and risk communication. Continuous monitoring and reporting of vaccine-induced complications, including ANCA GN, are mandatory [4,13]. Our study also highlights the need for standardized diagnostic criteria to diagnose vaccine-induced ANCA GN and comprehensive management guidelines. Ongoing research endeavors are obligatory to uncover the pathological mechanisms of vaccine-induced ANCA GN, mainly mRNA vaccines triggering immune-mediated GN. Collaborative research initiatives, genetic analyses, inflammatory pathways, and thorough autoimmune response after a vaccine are required to unravel the complex interplay of this vaccine-induced rare adverse event.
Despite valuable implications, our systematic review has a few limitations, including generalizability due to small sample data, incomplete understating of pathophysiological mechanisms, and reporting bias. Our study has no control group, limiting the ability to establish direct causal relationships between ANCA GN and the COVID-19 vaccine. Additionally, most patients reported no history of COVID-19 infection or kidney disease. These limitations provide insights for further research to improve the understanding of COVID-19 vaccine-induced ANCA GN.
Conclusions
COVID-19 vaccine-induced p-ANCA GN represents an uncommon but significant adverse event after vaccination. Our study provides valuable insights into the clinical characteristics, management, and outcomes of COVID-19 vaccine-induced p-ANCA GN. Timely recognition, probable diagnosis, and effective management are crucial in optimizing patient outcomes and ensuring effective surveillance. Physicians should remain vigilant regarding potential renal complications of the COVID-19 vaccine, particularly p-ANCA GN, and it should be included in the differential diagnosis of patients presenting with non-specific symptoms and AKI after the vaccine, mainly in the context of mRNA COVID-19 vaccine. Further research is warranted to unravel the underlying pathophysiology of COVID-19 vaccine-induced p-ANCA GN.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Effectiveness and safety of SARS-Co V-2 vaccine in real-world studies: a systematic review and meta-analysis Infect Dis Poverty Liu Q Qin C Liu M Liu J 1321020213477601110.1186/s 40249-021-00915-3PMC 8590867 · doi ↗ · pubmed ↗
- 2Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-Co V-2 and variants of concern: a narrative review Clin Microbiol Infect Fiolet T Kherabi Y Mac Donald CJ Ghosn J Peiffer-Smadja N 2022212820223471534710.1016/j.cmi.2021.10.005PMC 8548286 · doi ↗ · pubmed ↗
- 3The potential vaccine component for COVID-19: a comprehensive review of global vaccine development efforts Cureus Khan I Ahmed Z Sarwar A Jamil A Anwer F 012202010.7759/cureus.8871 PMC 738707532754408 · doi ↗ · pubmed ↗
- 4Pfizer-Bio N Tech COVID-19 vaccine (BNT 162b 2) side effects: a systematic review Cureus Dighriri IM Alhusayni KM Mobarki AY 014202210.7759/cureus.23526 PMC 903917135494952 · doi ↗ · pubmed ↗
- 5Adverse reactions of COVID-19 vaccines: a scoping review of observational studies Int J Gen Med Dhamanti I Suwantika AA Adlia A Yamani LN Yakub F 6096181620233684534110.2147/IJGM.S 400458 PMC 9951602 · doi ↗ · pubmed ↗
- 6The association of acute kidney injury with disease severity and mortality in COVID-19: a systematic review and meta-analysis Cureus Menon T Sharma R Kataria S 013202110.7759/cureus.13894 PMC 804556233880250 · doi ↗ · pubmed ↗
- 7Renal side effects of COVID-19 vaccination Vaccines (Basel) Zhang J Cao J Ye Q 17831020223636629210.3390/vaccines 10111783 PMC 9696189 · doi ↗ · pubmed ↗
- 8ANCA associated glomerulonephritis following SARS-Co V-2 vaccination: a case series and systematic review Vaccines (Basel) Thammathiwat T Banjongjit A Iampenkhae K Townamchai N Kanjanabuch T 9831120233724308710.3390/vaccines 11050983 PMC 10223042 · doi ↗ · pubmed ↗