Outcomes from Early Experience with Laparoscopic Inguinal Hernia Repair Versus Open Technique: Navigating the learning curve
MA Raajeshwaren, Chellappa Vijayakumar, Souradeep Dutta, Vishnu PN Ramakrishnaiah

TL;DR
This study compares laparoscopic and open hernia repair techniques, finding faster recovery and fewer infections with laparoscopic surgery, but higher recurrence and chronic pain in early experience.
Contribution
The study provides insights into the outcomes of early laparoscopic hernia repair in a South Indian hospital, highlighting a learning curve effect.
Findings
Laparoscopic repair showed faster recovery and lower surgical site infections.
Chronic pain and recurrence rates were higher with laparoscopic repair.
The results suggest a learning curve effect in early laparoscopic hernia repair.
Abstract
This study aimed to evaluate the outcomes of laparoscopic inguinal hernia repair (LIHR) regarding postoperative pain, recurrence rates, duration of hospital stay and other postoperative outcomes within the context of a tertiary care teaching hospital in South India, and the initial experience of laparoscopic repairs. The current consensus in the literature often suggests LIHR as superior to open inguinal hernia repair (OIHR). This single-centre, retrospective, observational study was conducted at the Jawaharlal Institute of Postgraduate Education and Research, Puducherry, India, from January 2011 to September 2020. All patients who underwent elective OIHR and LIHR were included. Data on the patients demographics, comorbidities, hernia type, mesh characteristics, surgery duration, hospital stay and immediate postoperative complications were collected and analysed. A total of 2,690 OIHR…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
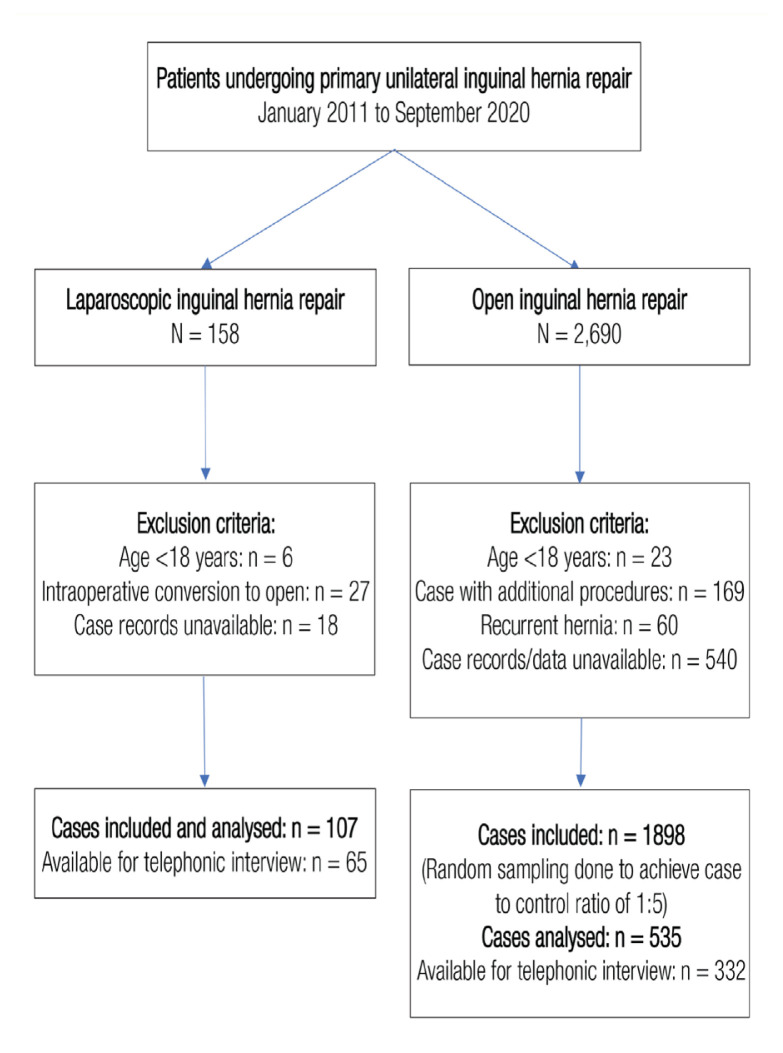 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Malformations and Hemangiomas
Inguinal hernias constitute a significant proportion of routine clinical encounters, representing approximately 75% of all abdominal hernias.1 Globally, inguinal hernia repair (IHR) is an extensively performed surgical procedure which is done on upwards of 20 million people.2 While surgery serves as the definitive treatment, the choice between laparoscopic and open techniques remains a topic of ongoing discussion. Contemporary studies suggest a decrease in postoperative pain following laparoscopic IHR (LIHR) and a higher incidence of surgical site infections (SSI) associated with open IHRs (OIHR).3,4 Notably, patient recovery following LIHR tends to be more expedient.
A significant challenge with LIHR is its comparatively steep learning curve, underscoring the importance of surgical techniques in mitigating complications. Standardisation of LIHR is instrumental in reducing recurrence rates, expediting recovery and decreasing postoperative complications such as pain and SSI. The surgeon’s experience, thus, holds a critical influence on surgical outcomes.5,6 Recurrence rates with LIHR have been shown to decline with increasing surgeon experience and volume of hernia repairs performed.7 Against this backdrop, the current study aimed to analyse and compare the recurrence rates among patients undergoing LIHR and OIHR, specifically within the context of the early experience with laparoscopic techniques at the department of Surgery at the Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry, India.
The researchers hypothesise that LIHRs may demonstrate differences in outcomes such as recurrence rates, postoperative complications and chronic pain, compared to OIHR. Furthermore, the research posits that the experience level of the surgeon and the surgical approach may play a significant role in determining these outcomes.
Methods
This single-centre, retrospective, observational study took place at the Jawaharlal Institute of Postgraduate Education and Research, Puducherry, India, and included all patients who underwent elective OIHR and LIHR from January 2011 to September 2020 based on the hospital medical records. This study was conducted from July 2020 to April 2021 and the patients were interviewed over the telephone because of COVID-19 restrictions. The study excluded IHR done under local anaesthesia, laparoscopy converted open repair, hernia with hydrocele, giant hernia with a sliding component, scrotal abdomen and additional procedures such as bowel or omental resection.
This study also excluded emergency hernia repair (inguinoscrotal approach), recurrent hernia repair, bilateral hernia and femoral hernia repair. This study recorded baseline demographic parameters, intraoperative and immediate postoperative outcomes such as duration of hospital stay, intensive care unit stays, surgical complications and reoperations. This study identified immediate complications such as paralytic ileus, haematoma, seroma, SSI and urinary retention in the hospital medical records. Telephone interviews were conducted with each patient to help assess late postoperative outcomes such as recurrence, chronic pain and their characteristics. This telephone interview was the single point of contact between the patient and the investigator.
Recurrence was recorded as the appearance of the inguinal swelling in the previously operated site. This recurrence was graded as per the patient’s words—being smaller, bigger or the same size as the previous swelling before surgery. The precipitating factors for the recurrence, such as heavy weightlifting and chronic cough, were also recorded. Chronic pain was recorded as pain at rest and pain with movement. The frequency was assessed as no pain, rare pain, once or twice a week and continuous pain. The intensity of pain was graded as mild (tolerable pain not affecting daily routine), moderate (needed rest from the daily routine for relief) and severe (required painkillers for pain relief and affected daily routine). The preoperative, intraoperative and postoperative parameters which influenced the primary and secondary outcomes were noted for analysis.
The expertise of the surgeons who operated the LIHR was graded based on their years of experience in LIHR. The surgeons who had less than 3 years of experience were graded as level I. Those with 4–6 years of experience in LIHR were graded as level II, and those with more than 6 years of experience in LIHR were graded as level III. Based on this, the outcomes were analysed. Sub-group analysis of LIHR with robotic IHR was done for postoperative outcomes.
The sample size was calculated using the OpenEpi software, Version 3.1 (Emory University, Atlanta, Georgia, USA)—keeping the proportion of group 1 - LIHR patients with recurrence of hernia as 3.4% (exposed with the outcome) and the same in group 2 - OIHR as 5.2% (unexposed with the outcome), with 80% power and an alpha of 5%—as 1,652 in each group. From the medical record review, it was found that only 158 cases of laparoscopic hernia repairs for primary unilateral hernias had been done during the study period, and hence, a sample size of 1,652 was not achievable. Therefore, after inclusion and exclusion criteria for the above inguinal hernia repairs were performed, a total of 107 and 1,898 cases were analysed in the LIHR and OHR groups, respectively. Since there was a massive difference in the total number of cases between the two groups, the total number of cases taken was in the ratio 1:5 (i.e. 107 versus 535). This was considered as there was no significant difference in the P value for cases more than 4 times the control.
Statistical analysis was done using the Statistical Package for the Social Sciences (SPSS), Version 19.0 (IBM Corp, Armonk, New York, USA). The Mann-Whitney U test was used. All categorical variables were expressed as proportions. They were analysed appropriately with the Chi-squared test or Fischer’s exact test based on the normality evaluated by the Shapiro-Wilk test. The logistic regression analysis was done for the primary outcome, i.e. the recurrence. Independent variables were analysed for their association with recurrence and those which had a P value of <0.2 were used for multivariate regression.
The odds ratio with 95% confidence interval (CI) and P value was summarised and used to interpret the association of independent variables with outcome. A P value <0.05 was considered statistically significant. Ethical approval from the Institutional Ethics Committee of the hospital was obtained in 2019 (JIP/IEC/2019/529).
Results
A total of 158 cases of LIHR and 2,690 cases of OIHR were identified during the study period. Based on exclusion and inclusion criteria, 107 patients were chosen in the LIHR group and 1,898 in the OIHR group. However, given the discrepancy in the number of cases, the researchers analysed only 642 patients (107 in LIHR and 535 in OIHR) who underwent hernia surgery between January 2011 and September 2020 [Figure 1].
Most patients were older than 40 years (61.53%), with a median age of 47 years. The pattern of patient distribution was similar in both groups, except for the OIHR group having a greater proportion of smokers; 6.17% of the OIHR group patients were smokers compared to 2.80% in the LIHR group. The prevalence of benign prostate hypertrophy was similar in both groups (8.41% versus 7.66%; P = 0.79). The overall percentage of patients with comorbidities between the groups was similar [Table 1].
The usage of prophylactic antibiotics was subject to the surgeon’s discretion. This difference was statistically significant between the two groups (84.11% versus 69.53%; P <0.05). Out of the patients who received antibiotics, the majority of them received ≤3 doses of antibiotics. However, in this study, the usage of antibiotics did not affect SSI (P = 0.13). The indirect sac was most commonly identified in both groups accounting for 71.03% in the LIHR and 68.04% in the OIHR group. Approximately 96.82% of the patients in the OIHR used a 15 × 7 cm mesh. The mesh used for the entire cohort of the OIHR was made up of polypropylene. The difference between the groups was statistically significant (P <0.05). In the majority of the LIHR group (79.44%) the mesh was fixed using tackers. Almost the entire cohort of the OIHR cases (97.94%) had the mesh fixed with polypropylene sutures.
Most of the patients did not have any content in the hernia sac, majorly due to a reduction of the content preoperatively. The most commonly encountered content intraoperatively was omentum accounting for (17.76% and 22.24%) the LIHR and OIHR cases, respectively. The distal sac was reduced (66.36% versus 15.70%) primarily in LIHR, but it was transfixed (15.89% versus 74.02%) predominantly in the OIHR. The duration of the procedure was more for the LIHR than the OIHR. It was very clearly established that an open hernia needed less time to operate and the difference was statistically significant (150 versus 75 minutes; P <0.05). The median duration of hospital stay was also similar in both groups, i.e. 3 days with an Inter Quartile Range (IQR) of 3–4 days in the LIHR group and 2–3 days in the OIHR group (P <0.05) [Table 2].
None of the patients in the LIHR group developed SSI. This finding was statistically significant (P <0.05). A total of 12 patients had scrotal edema following OIHR surgery, while none in the LIHR group developed it (P <0.05). The most encountered immediate complication in the LIHR was subcutaneous emphysema; this was statistically significant (P <0.05). This study found that patients who developed SSI were in the OIHR (3.55%) group and not in the LIHR group (0.00%). Urinary retention was similar in both groups in this study [Table 3]. The data on the late postoperative outcomes could be obtained only from 65 and 332 patients, in the LIHR and OIHR groups, respectively, via telephone conversations. In this, the recurrence rate between the two groups was 9.23% (n = 6) in the LIHR group and 3.61% (n = 12) in the OIHR group. The recurrences were significantly more in terms of numbers, but they were not statistically significant (P = 0.09). The difference in chronic pain between the groups was statistically significant (41.53% versus 13.55%; P <0.05) [Table 4].
The time taken for the patients to do their normal routine activities was 6 days and 8 days for the LIHR and OIHR groups, respectively. The distribution was again a non-normally distributed one with a few outliers in the group. This was mainly due to the development of complications. The 25th percentile was 4 and 6 for LIHR and OIHR groups, while the 75th percentile was 10 for both groups. The difference between the groups was statistically significant (P <0.05). The odds of developing chronic pain with movement were 5.28 times more for LIHR with a 95% CI of 2.91–9.59 and, thus, significant. The odds of recurrence were 2.69 times higher for the LIHR group than for the OIHR group. However, the 95% CI was wide (0.97–7.46), which makes it an insignificant value. Similarly, the odds of developing a seroma or chronic pain at rest were 2.61 and 0.83 times for the LIHR group and the OIHR group, respectively. However, the CI was wide (0.23–29.29 and 0.24–2.89, respectively).
The odds of recurrence were higher with diabetes mellitus (DM), followed by time to return to normal activities and SSI. DM, superficial SSI and time to return to normal activities had P <0.05. In a multivariate regression analysis, the significant variables in the LIHR group were: history of smoking, presence of DM, duration of the procedure, mesh fixation with tackers, the number of doses of antibiotics, time to return to normal activities and the presence of superficial SSI. This analysis showed that the presence of DM, time to return to normal activities and superficial SSI were factors that had a significant influence on the recurrence of the hernia (adjusted odds ratio = 19.01, 1.16 and 8.15, respectively) [Tables 5 & 6].
Recurrence was found only in 1 out of 26 patients operated by level III surgeons. However, recurrence was reported in 5 out of 40 cases performed by level II and level I surgeons. A total of 9 out of 21 patients operated by level I surgeons developed chronic pain with movement. The same was reported in 9 out of 19 patients for level II surgeons and 9 out of 26 patients in level III surgeons.
Discussion
Inguinal hernia consistently ranks as a common condition faced in general practice. Surgical interventions such as LIHR and OIHR form the definitive therapeutic approach. In the current study, both techniques shared a similar hospital stay duration averaging approximately 3 days. Importantly, LIHR demonstrated a significantly faster recovery time back to normal activities. Nonetheless, complication rates between the two groups were similar, while recurrence and chronic pain were observed more frequently in the LIHR cohort. These findings, perhaps, could be reflective of the institution’s relative early experience with LIHR as compared to OIHR, suggesting the significance of the surgical learning curve in impacting outcomes.
On examination of the demographic data, it became clear that comorbidity prevalence profoundly impacted postoperative complication development. The current study as well as the study by Ruhl et al. found a predominance of patients older than 40.9 years.8 Additionally, right-sided hernias were more common, likely due to the later closure of the processus vaginalis on this side. Notably, lifestyle factors and comorbidities such as tobacco use, alcohol and DM were implicated in structural remodelling of the inguinal region, thereby increasing the incidence of inguinal hernia.9
In the realm of intraoperative parameters, the current study mirrored prior research, showing a greater prevalence of indirect than direct sacs.10,11 The majority of patients had no hernia sac content intraoperatively, mainly due to preoperative reduction efforts. Interestingly, after overcoming the learning curve, surgeons demonstrated no significant differences in operating times between techniques.12,13 Regarding antibiotic prophylaxis, the need for a balance between minimising SSI rates and avoiding unnecessary antibiotic use became evident.2,14
Concerning early postoperative complications, the occurrence of subcutaneous emphysema was higher in the LIHR group, attributed to the nature of gas insufflation during the procedure.15–17 Post-LIHR urinary retention appeared more common, although robust evidence is lacking.18,19 The return to routine activities was significantly quicker with LIHR, which has been echoed in various studies.20,21 Regarding late postoperative complications, a higher recurrence rate in LIHR was noted, which might be associated with the steep learning curve of this procedure.2,22 While the recurrence rates seemed higher in the LIHR group, the statistical analysis did not find a significant difference. This could be attributed to various factors such as the smaller sample size in the LIHR group, which might have limited the study’s ability to detect a significant difference. Additionally, other confounding factors, such as the learning curve, varying surgical techniques or patient selection, might have influenced recurrence rates. However, risk factors such as DM and wound infection did not significantly affect recurrence rates.23,24 The study findings deviated from the consensus in terms of chronic pain incidence, which was higher with LIHR, aligning with Huerta et al.16,25 This departure from the trend may be ascribed to the early experience stage of the institution with laparoscopic techniques for managing inguinal hernias.
In recent years, there has been increasing interest in the integration of artificial intelligence (AI) and deep learning into surgical practice, aimed at enhancing surgical precision, optimising patient outcomes and reducing complications.26 While the current study focuses on traditional laparoscopic and open hernia repairs, the evolution of surgery with technological advancements cannot be ignored. It is imperative to acknowledge the potential challenges and benefits of integrating AI into surgical procedures.26 As hernia repair techniques continue to evolve, it is crucial to remain updated with the latest technological advancements and their implications.
The current study has several limitations that need to be considered while interpreting the results. First, the retrospective nature of the research inherently carries the risk of information bias, with potential discrepancies in the data recording process over time. The long study period also exposes the analysis to changes in surgical techniques, equipment and postoperative care protocols, all of which could affect outcomes. Second, the marked difference in the sample sizes between the OIHR (n = 2,690) and LIHR (n = 158) groups pose challenges in drawing direct comparisons and could potentially skew the findings. The smaller sample size in the LIHR group could have made the detection of rare complications less likely compared to that in the larger OIHR group. Finally, the grading of surgeon expertise based solely on years of experience in LIHR, though a useful proxy, does not consider other vital factors such as the volume of surgeries performed, specific training and continuous skill upgrades. This grading may overlook nuances in surgical proficiency, as years of experience might not directly correlate with skill or outcomes. Future studies should employ a more comprehensive and objective measure of surgical expertise to further elucidate the role of surgeon skill in patient outcomes.
Conclusion
The research findings underscore the importance of the surgical learning curve in achieving optimal outcomes in LIHR. While LIHR demonstrated faster recovery times compared to OIHR, it also revealed a higher incidence of recurrence and chronic pain. These trends may be attributed to the institution’s relative early experience with LIHR. Furthermore, the current study highlights the significance of comorbidities and lifestyle factors in hernia development and postoperative complications. Despite the limitations inherent in a retrospective study, this investigation provides valuable insights into the management of inguinal hernias. Future prospective studies with larger cohorts are needed to confirm the study findings and enhance the understanding of LIHR outcomes concerning the learning curve and early experience of surgeons.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jenkins JTO’Dwyer PJ Inguinal hernias BMJ 2008 336 269 72 10.1136/bmj.39450.428275.ad 18244999 PMC 2223000 · doi ↗ · pubmed ↗
- 2Hernia Surge Group International guidelines for groin hernia management Hernia 2018 22 1 165 10.1007/s 10029-017-1668-x PMC 580958229330835 · doi ↗ · pubmed ↗
- 3Bullen NL Massey LH Antoniou SA Smart NJ Fortelny RH Open versus laparoscopic mesh repair of primary unilateral uncomplicated inguinal hernia: A systematic review with meta-analysis and trial sequential analysis Hernia 2019 23 461 72 10.1007/s 10029-019-01989-7 31161285 · doi ↗ · pubmed ↗
- 4Perez AJ Strassle PD Sadava EE Gaber C Schlottmann F Nationwide analysis of inpatient laparoscopic versus open inguinal hernia repair J Laparoendosc Adv Surg Tech A 2020 30 292 8 10.1089/lap.2019.0656 31934801 · doi ↗ · pubmed ↗
- 5Butters M Redecke JKöninger J Long-term results of a randomized clinical trial of Shouldice, Lichtenstein and transabdominal preperitoneal hernia repairs Br J Surg 2007 94 562 5 10.1002/bjs.5733 17443855 · doi ↗ · pubmed ↗
- 6Eklund AS Montgomery AK Rasmussen IC Sandbue RP Bergkvist LA Rudberg CR Low recurrence rate after laparoscopic (TEP) and open (Lichtenstein) inguinal hernia repair: A randomized, multicenter trial with 5-year follow-up Ann Surg 2009 249 33 8 10.1097/sla.0b 013e 31819255 d 0 19106673 · doi ↗ · pubmed ↗
- 7Feliu-PalàX Martín-Gómez M Morales-Conde S Fernández-Sallent E The impact of the surgeon’s experience on the results of laparoscopic hernia repair Surg Endosc 2001 15 1467 70 10.1007/s 00464-001-9017-6 11965467 · doi ↗ · pubmed ↗
- 8Ruhl CE Everhart JE Risk factors for inguinal hernia among adults in the US population Am J Epidemiol 2007 165 1154 61 10.1093/aje/kwm 011 17374852 · doi ↗ · pubmed ↗