Protocol for a multicentre prospective exploratory mixed-methods study investigating the modifiable psychosocial variables influencing access to and outcomes after kidney transplantation in children and young people in the UK
Ji Soo Kim, Jo Wray, Deborah Ridout, Lucy Plumb, Dorothea Nitsch, Matthew Robb, Stephen D Marks

TL;DR
This study explores psychosocial factors affecting kidney transplant access and outcomes for children in the UK using mixed methods.
Contribution
The study introduces a mixed-methods protocol to identify modifiable psychosocial variables in pediatric kidney transplantation.
Findings
Qualitative interviews will inform questionnaire selection for a national cohort.
Health data will be integrated with psychosocial data to identify care improvement opportunities.
Results will be shared with families and through academic publications.
Abstract
Kidney transplantation is the preferred therapy for children with stage 5 chronic kidney disease (CKD-5). However, there is a wide variation in access to kidney transplantation across the UK for children. This study aims to explore the psychosocial factors that influence access to and outcomes after kidney transplantation in children in the UK using a mixed-methods prospective longitudinal design. Qualitative data will be collected through semistructured interviews with children affected by CKD-5, their carers and paediatric renal multidisciplinary team. Recruitment for interviews will continue till data saturation. These interviews will inform the choice of existing validated questionnaires, which will be distributed to a larger national cohort of children with pretransplant CKD-5 (n=180) and their carers. Follow-up questionnaires will be sent at protocolised time points regardless of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
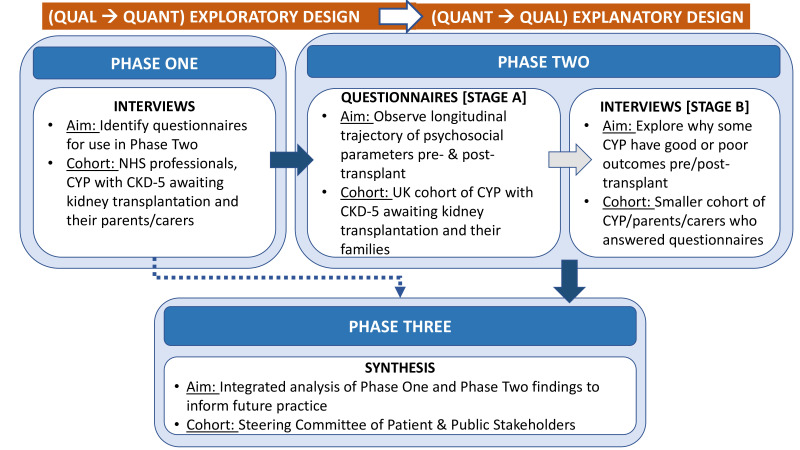 Figure 1
Figure 1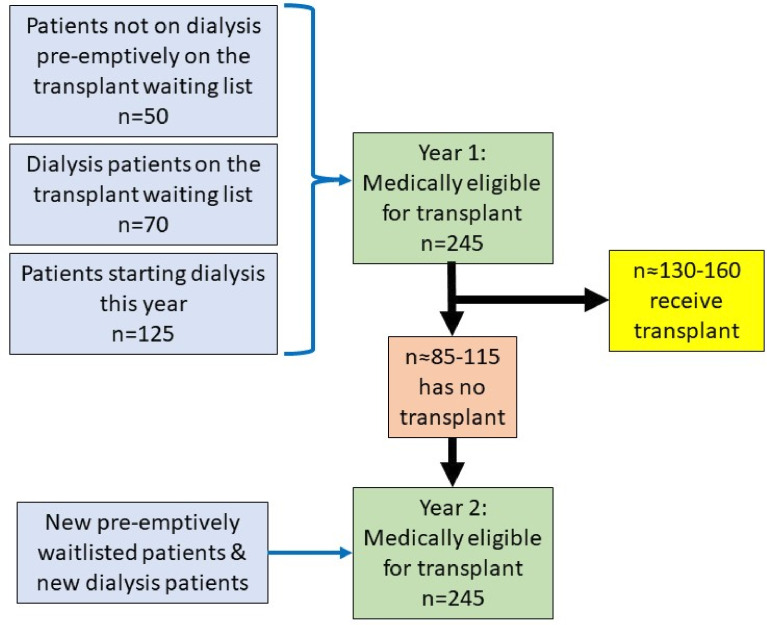 Figure 2
Figure 2| Baseline of all participating CYP | CYP not transplanted yet at 12 months follow-up | CYP who are post-transplant |
|
Ethnicity Primary renal diagnosis Other comorbidity diagnoses Modality of KRT if applicable Date confirming CKD-5 Date of starting KRT if applicable Date of previous kidney transplant reaching CKD-5 if applicable Height (cm) Weight (kg) Serum creatinine (μmol/L) Number and type of medications Post code* |
Modality of KRT if changed (if applicable) Date of starting new modality of KRT (if applicable) Height (cm) Weight (kg) Serum Creatinine (µmol/L) Number and type of medications | Only at 3 months post-transplant Type of transplant kidney (living related/living unrelated/deceased donor (after cardiac or brain death) Donor and recipient mismatch ABO blood group compatibility Cold ischaemic time Need for plasma exchange/immunoadsorption/Rituximab/intravenous immunoglobulin Changes to comorbidities if applicable Change of KRT modality if applicable Date of KRT modality change if applicable Height (cm) Weight (kg) Serum creatinine (µmol/L) Number and type of medications |
- —http://dx.doi.org/10.13039/501100000272National Institute for Health and Care Research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal Transplantation Outcomes and Treatments · Organ Transplantation Techniques and Outcomes · Organ Donation and Transplantation
Introduction
Around 1000 children (aged 0–17 years) with stage 5 chronic kidney disease (CKD-5) in the UK receive kidney replacement therapy (KRT) in the form of either peritoneal dialysis, haemodialysis or kidney transplantation.1 2 Kidney transplantation is the gold-standard therapy for reducing mortality and improving outcomes for children.3 Minimising time on dialysis in favour of transplantation has been shown to reduce CKD-5-related complications and morbidity.4 Compared with dialysis, transplantation is also presumed to improve patients’ health-related quality of life (HR-QoL).5 Furthermore in the UK, for every year that the patient’s kidney transplant functions, transplantation is three times more cost-effective than dialysis for the National Health Service (NHS).6
However, not every child with CKD-5 can access kidney transplantation. There are approximately 193–217 prevalent children on dialysis each year.7 8 Annually only 130–160 paediatric kidney transplants are performed in the UK.9 There appears to be variation in transplantation access, practice and outcomes between UK paediatric nephrology units.1 2 9 A cross-sectional survey conducted by the British Association for Paediatric Nephrology examined reasons for paediatric kidney transplantation delay in the UK. The survey showed that psychosocial factors make up 19% of the barriers, although specific factors were not identified in this study.10 Compared with paediatrics, considerable research has been done in adult patients, regarding psychosocial factors implicated in transplant access. Formalised pretransplant and post-transplant psychosocial assessments have been widely researched for adult solid organ transplant recipients.11–14 The UK-wide study, ‘Access to Transplantation and Transplant Outcome Measures’ specifically investigated psychosocial barriers in adult kidney transplant recipients.15 Researchers found inequities in transplant access, in spite of a universal healthcare system, based on socioeconomic status, education level, health literacy and racial background.16 17 In terms of outcomes, they found no difference in post-transplant HR-QoL between living and deceased donor recipients and that recipient expectations influenced post-transplant recovery.15–19 However, for the UK children, it is less clear what these ‘psychosocial factors’ are and how they influence unit-specific decisions, access to kidney transplantation and outcomes.10 20 21 We acknowledge the recent progress being made in exploring these psychosocial factors in some countries.22–24 However, psychosocial studies for children with CKD-5 are still limited by retrospective or cross-sectional design or by single-centre or small study cohorts. There are no UK studies that prospectively explore how these factors impact paediatric kidney transplantation access over time.
Aims and objectives
This study aims to prospectively evaluate the psychosocial factors that are actual or perceived barriers to paediatric kidney transplantation which may be associated with poor transplant outcome. We anticipate these psychosocial factors to be broad at an individual, family and societal level and that they will encompass mental health and social determinants of health as defined by Marmot et al: ‘the conditions in which people are born, grow, live, work and age’25—we hypothesise that psychosocial factors implicated in transplant access can be quantified using formal, validated measures and that these factors may influence outcomes in the short-term period following transplantation.
This will be achieved through the following research objectives:
Describe the psychosocial factors perceived by clinicians as barriers to kidney transplantation.Describe current interventions (if any) implemented to address these psychosocial factors.Explore the experiences and beliefs of children and their families regarding any psychosocial challenges or facilitators in accessing a kidney transplant.Quantify the identified psychosocial factors implicated in CKD management.Measure the prevalence of identified psychosocial factors (positive and negative) in the national cohort of patients being pre-emptively worked up for transplant, on dialysis or listed for transplant.Examine these psychosocial factors regarding their association with time to transplant and their changes following transplantation.Synthesise findings from each phase to inform recommendations about which psychosocial factors are potential barriers or facilitators to accessing kidney transplantation.
Findings synthesised from this study will inform the development of a complex intervention to improve uptake of kidney transplantation in children with CKD-5 who would benefit most from one.
Methods and analysis
Study design overview
This prospective study has three phases, commencing with a sequential exploratory mixed-methods design, followed by a sequential explanatory mixed-methods design (figure 1).26 This approach was chosen to first gain new insights by becoming familiar with the range of potential psychosocial factors and then longitudinally observing the influence of these factors on kidney transplantation access and outcomes for children.27 Phase 1 will consist of exploratory interviews with purposively selected participants. These interviews will inform which questionnaires will be distributed at baseline and follow-up to the wider cohort of children with CKD-5 and their carer(s) in phase 2 stage A. Using the interviews to inform questionnaire selection will ensure questionnaires are relevant to, and resonate with, families. Participant families with outlier findings from phase 2 stage A will then be invited for explanatory interviews in phase 2 stage B. Finally, in phase 3, the qualitative and quantitative data from the previous phases will be analysed together to develop an integrated understanding of psychosocial factors that influence access to kidney transplantation.
Flow diagram of sequential mixed-method study design. CYP, children and young people; NHS, National Health Service.
Patient and public involvement
All elements of the study design were codeveloped and approved by our Research Partner Family and study steering group. Our Research Partner Family (a young person and parent dyad) and steering group members have lived experience of CKD, dialysis and kidney transplantation in childhood either as a patient or carer. The Great Ormond Street Hospital Young Persons Advisory Group has also approved the research question and study design. The Young Persons Advisory Group consists of children affiliated with Great Ormond Street Hospital for Children NHS Foundation Trust as a patient or family member of a patient and therefore who have the lived experience needed to advise researchers designing studies involving children.
Population
This study aims to include children, carer and staff participants from all 13 UK paediatric nephrology units, of which 10 units offer kidney transplantation surgery on site and 3 units which do not offer transplantation surgery at their own site but offer shared transplant care with nearby units.
In phase 1 and phase 2 stage A, children (aged 0–17 years inclusive) with CKD-5 on chronic dialysis, being worked up for pre-emptive kidney transplantation or on the waiting list for deceased donation (active or suspended) or awaiting living donation, will be invited to participate with their carer(s). Where appropriate, children aged 5 years and above will be invited to directly participate. For children aged under 5 years or those who are unable to assent or consent, their carers will be consulted and offered an opportunity to participate through proxy measures. Members of the multidisciplinary team (MDT) involved in pretransplantation workup at their local unit (eg, paediatric nephrologists, transplant surgeons, nurse specialists, social workers, family therapists, play therapists and members of the psychosocial team) will be invited for interviews in phase 1 only. Patients or carer(s) who are unable to give informed consent or patients who have been deemed too unwell to participate or had a recent acute hospital admission in the last 14 days will not be approached to participate in the study.
Phase 1 interviews
A purposive sampling matrix will be used to maximise the diversity of views. Criteria for sampling will include age, sex and ethnicity of children, modality of KRT, whether the kidney unit offers transplantation surgery or not and role in the MDT. Completed interviews will be analysed in parallel with ongoing recruitment. Participant recruitment will stop when no new themes are generated from the data.
Analysis of these interviews will contribute towards selecting questionnaires for use in phase 2 stage A.
Phase 2 stage A questionnaires
In this phase, we will aim to recruit every child with CKD-5 who meets the inclusion criteria at pretransplant baseline with an anticipated recruitment rate of 60%–70%.
At the time of study design, the predicted annual numbers across all 13 UK paediatric nephrology units as per UK Renal Registry (UKRR) reports were as follows1 2:
Number of dialysis patients on the transplant waiting-list in a year; n=70.Number of patients starting dialysis in a year; n=125.Number of patients not on dialysis but pre-emptively on the transplant waiting list; n=50.Transplant rate; 130–160 patients per year.
Based on these numbers, the predicted maximum number of eligible participants in a 1-year period would be 245. We chose a 2-year period for our sample size calculation, which would be a population size of 490, to include children who experience delays and receive their transplant after 1 year (see figure 2). We plan to recruit 180 patients and after allowing for a 20% drop-out, we expect to include 141 families. Assuming a prevalence of pertinent psychosocial factors in the national cohort of patients being pre-emptively worked up for transplant, on dialysis or listed for transplant of 15%, then with 141 families we will be able to estimate this with 5% precision. At the time of sample size calculation, there were no paediatric studies specifically measuring this nor studies encompassing all psychosocial factors. Therefore, we used the assumed prevalence of 15% based on a study measuring psychological distress in potential adult transplant candidates.28
Flow diagram illustrating predicted number of CYP who are eligible for transplantation and receive one across 2 years. CYP, children and young people.
We expect some overlap in the cohort between phase 1 and phase 2 stage A and appreciate some families may develop research fatigue. Families who already took part in phase 1 will be asked whether they would like to also take part in phase 2 stage A or prefer to opt-out.
Phase 2 stage B
Results from phase 2 stage A will be reviewed for negative and positive cases. Families who have outlier findings, in terms of their answers to the validated questionnaires, will be invited to interview in phase 2 stage B, with the aim of reviewing and refining themes to develop additional theoretical explanation for the influence of psychosocial factors on transplant access and outcomes. The exact parameters to define outliers and sample size will be dependent on findings from phase 2 stage A.
Outcomes measured
Phase 1
Using a Topic Guide (online supplemental material 1), qualitative data will be collected in phase 1 to address research objectives 1–4 through semistructured, in-depth interviews undertaken by the investigator (JSK). This format was chosen over focus groups to enable participation of younger or less verbal children and avoid further inconveniencing families through multiple research appointments by having separate interviews for young children and focus groups for carers. The family interview format will be based on the child’s decision to either interview with or separately from their carers, depending on which setting they find more comfortable. To ensure no participant is unfairly excluded from interviews due to English not being their first language, interpreters will be present to support their participation. The same principle of minimising communication barriers will be applied to younger children or young people who may prefer communicating through other creative outputs such as drawing or Talking Mats. The research goals for family interviews will include exploring what families feel their life is like now living with CKD-5, what good HR-QoL looks like and what they believe delays or enables how soon they receive a kidney transplant. Similarly, research goals for MDT member interviews will include exploring what the professionals think matters most to families whose child has CKD-5 when it comes to a good HR-QoL and what they, as professionals, believe impacts how soon children access a kidney transplant in terms of psychosocial factors.
10.1136/bmjopen-2023-078150.supp1Supplementary data
The Topic Guide has been developed from the investigator’s systematic literature review on the subject matter and in consultation with the Young Persons Advisory Group and the Research Partner Family.29 To minimise any inconvenience in joining the study, all participants will be interviewed using their preferred modality (telephone, video-call or face-to-face consultations) in keeping with COVID-19 safety recommendations.30 Interview time with young children will be kept to less than half an hour to minimise interview fatigue. All interviews will be audio or video recorded depending on participant preference.
Participants may become distressed as they reflect on their experiences due to the sensitive nature of some of the interview topics around their mental health or transplant delays. Therefore, the participant and JSK will agree on a ‘stop signal’ before commencing the interview for use should they feel uncomfortable. If the participant uses the ‘stop signal’, they will be offered a break. The participant and JSK will then discuss whether they would like to continue, reschedule or withdraw from the interview altogether. Once the interview recording stops, there will be an opportunity to discuss the participant’s feelings and, if appropriate, they will be signposted to their local support services.
The acceptability of existing validated age-appropriate questionnaires that measure outcomes relevant to the preliminary themes will be discussed with the steering group. Potential validated questionnaires that capture the preliminary themes will be identified from the systematic literature review and a wider search of the literature. These questionnaires will be checked in terms of their psychometric properties such as internal consistency (Cronbach alpha of at least 0.7) and test–retest reliability and aspects such as availability of the measures, respondent type (parent, child or other respondent) and age range for which the questionnaire has been validated, to enable the most appropriate questionnaire to be chosen to measure each theme. The selected questionnaires will then be discussed with the steering group, considering the language of the questionnaire, acceptability and level of burden for the participant. If the list of questionnaires is too onerous for the participating family, a consensus will be reached with the steering group on which preliminary themes and therefore which questionnaires should be prioritised. Once the final list of questionnaires is agreed on, these will be submitted to the Health Research Authority for final approval.
Phase 2 stage A
In phase 2 stage A, research objectives 5–6 will be addressed by measuring the following primary outcome variables: HR-QoL, psychosocial functioning and time taken to receive a kidney transplant since the date confirming CKD-5. To understand changes in psychosocial factors over time, their associations with health burden or short-term allograft deterioration must be accounted for, Therefore, we will measure the following secondary outcome: the child’s estimated glomerular filtration rate (eGFR) over time. The eGFR will be calculated with their height and serum creatinine using the CkiD U25 formula.31 32
Questionnaires measuring HR-QoL and psychosocial functioning, selected from phase 1, will be distributed to a larger, national cohort of children with CKD-5 and their carers at their pretransplant baseline. Follow-up questionnaires will be sent post-transplant at 3, 6 and 12 months later or 12 months after their first questionnaire if they still have not received a kidney transplant in that time frame. These follow-up time points were chosen to reflect the initial period of post-transplant adaptation, which is comparable with similar studies in adults and children at the time of protocol-writing.33–35 For children who have not received a transplant, a 12-month interval was advised by our steering group to avoid distress triggered by frequent questionnaires reminding them of their non-transplanted state. As families are more likely to participate if they can choose which questionnaire modality is most suited to their lifestyle, participant families will be offered either paper or online questionnaires.36 Health morbidity and coexisting disease data, including their underlying primary kidney diagnosis, as described in table 1, will be mapped to each questionnaire time point.
An additional questionnaire (see online supplemental material 2) has been codesigned with the steering group to retrieve information on the participating family’s demographic background. Data on medication burden will also be collected due to its’ possible confounding effect HR-QoL as described in current literature.37
10.1136/bmjopen-2023-078150.supp2Supplementary data
Phase 2 stage B
The Interview Topic Guide for phase 2 stage B has been designed with flexibility since the interview will depend on the nature of the outlier findings from phase 2 stage A.
Data analysis plan
Phase 1
To address research objectives 1–4, JSK will thematically analyse interview transcripts, following the approach of Braun and Clarke.38 Deidentified transcripts will be managed using NVivo software.39 For the purposes of qualitative rigour, JSK will maintain a reflexivity journal after interviews and throughout data analysis, to ensure potential researcher biases and insights are noted. Maintaining a reflexivity journal is a gold-standard practice in qualitative research, which increases the credibility and deepens the understanding of the findings by describing the context in which data were collected and analysed.40 41 A sample of transcripts will be examined by JW and discussed with JSK. Throughout all stages of data collection and analysis, findings will be shared and discussed by JSK, JW and SM.
Phase 2 stage A
Participant demographics will be described using descriptive statistics. It will also be used to address research objective 4 by describing the prevalence of psychosocial factors.
Research objective 6 will be addressed through the following:
First, descriptive statistics will again be used to describe how participants’ psychosocial functioning and HR-QoL variables change before and after transplantation at each data collection time point.
Second, to describe the impact waiting to access a kidney transplant and receiving one has on psychosocial functioning and HR-QoL over time, repeated measure analysis of variance will be undertaken.
Third, the association between clinical, demographic and psychosocial factors with accessing a kidney transplant will be measured using logistic regression modelling and Kaplan-Meier statistics.
Fourth, the association of clinical, demographic and psychosocial factors with failing transplant allograft in short-term follow-up between 1 and 2 years post-transplantation will be assessed. Where the outcome variable is the child’s eGFR, linear regression modelling will be used. Where the outcome variable defines a failing post-transplant kidney as reaching an eGFR equivalent to stage IV CKD (eGFR 15–29 mL/min/1.73 m^2^), logistic regression modelling and Kaplan-Meier statistics will be used.
Separately, the level of agreement between child and carer responses will be assessed. Choice of statistical tests will depend on the type of data, for example, Cohen’s kappa for binary data, weighted kappa for ordinal data or interclass correlation coefficients for continuous data.
Where relevant, all statistical analyses will be adjusted for (but not limited to) child’s age, gender, ethnicity, socioeconomic status and KRT status at baseline.
Phase 2 stage B
Interview data will be analysed using thematic analysis underpinned by the same principles as in phase 1.
Phase 3
An integrative analysis of data from phases 1 and 2 will be undertaken to address research objective 7 and create a conceptual model of how psychosocial factors influence transplant access and outcomes. The quantitative and qualitative data will be reviewed together to understand where they converge, complement or diverge from the other dataset or have findings that are novel. A final lay report will be cowritten with the steering group to ensure it is meaningful, relevant and accessible to families whose child has CKD.
Ethics
This study protocol has been peer reviewed by the National Institute for Health Research Academy and has been approved under IRAS number 270493 by the Wales Research Ethics Committee 4 (ref: 20/WA/0285) and the Scotland A Research Ethics Committee (ref: 21/SS/0038).
Coercive pressure of joining the study will be minimised. Research participants will not be paid for participation. Participant information sheets will indicate that there will be no added benefit or disruption to their medical care.
Informed written consent will be obtained from all participants aged ≥16 years old and written assent from participants aged 5–15 years old. Consent will be obtained for all research activities including interviews, questionnaires and retrieving health information from national databases and hospital records.
Participant confidentiality will be upheld by fully adhering to the Data Protection Act. Participant identifiers will be handled with appropriate pseudonymisation and all data will be kept on General Data Protection Regulation (GDPR) compliant encrypted devices or stored on hard drives with restricted access with the relevant encryption and password protection. The only instance where confidentiality will be breached is if a participant discloses information that has direct implications for child or adult safeguarding. Potential participants will be made aware of this as part of informed consent. All interviews will be digitally recorded, transcribed verbatim and have identifiable data redacted. Audio files will be transcribed either by JSK or by a third-party interview transcription company (Take Note). To minimise data handling breaches, all engagement with Take Note will only be through their secure web platform. All video files will be transcribed only by JSK to remove third-party involvement in the deidentification process. Once deidentified, only quotes that cannot lead to participant identification will be used in reports. Care will be taken in reporting findings to ensure individuals cannot be identified by their role, diagnosis, gender, age or geographic locality.
Dissemination
Research participants will be updated about the findings through newsletters. Lay summaries approved by the steering group will be disseminated across charity websites accessed by children and families affected by CKD. To ensure that professionals who work with families affected by CKD are being reached, findings will be disseminated widely in relevant peer-reviewed journals and at national and international conferences. Finally, if appropriate, a dissemination strategy will be cocreated between JSK and the steering group for other professionals (eg, teachers) who may encounter vulnerable families with CKD and need early referral for psychosocial intervention.
Supplementary Material
Reviewer comments
Author's manuscript
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Plumb L , Casula A , Pyart R , et al . The 21st UK renal Registry annual report: a summary of analyses of Paediatric data in 2017. Nephron 2020;144:67–71. 10.1159/000504852 31825936 · doi ↗ · pubmed ↗
- 2Plumb L , Wong E , Casula A , et al . Chapter 4 demography of the UK Paediatric renal replacement therapy population in 2016. Nephron 2018;139 Suppl 1:105–16. 10.1159/000490962 29991000 · doi ↗ · pubmed ↗
- 3Wolfe RA , Ashby VB , Milford EL , et al . Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first Cadaveric transplant. N Engl J Med 1999;341:1725–30. 10.1056/NEJM 199912023412303 10580071 · doi ↗ · pubmed ↗
- 4Pruthi R , Casula A , Inward C , et al . Early requirement for RRT in children at presentation in the United kingdom: association with transplantation and survival. Clin J Am Soc Nephrol 2016;11:795–802. 10.2215/CJN.08190815 26912550 PMC 4858480 · doi ↗ · pubmed ↗
- 5Park K-S , Hwang YJ , Cho MH , et al . Quality of life in children with end-stage renal disease based on a Pedsql ESRD Module. Pediatr Nephrol 2012;27:2293–300. 10.1007/s 00467-012-2262-1 22832667 · doi ↗ · pubmed ↗
- 6Kerr M , Bray B , Medcalf J , et al . Estimating the financial cost of chronic kidney disease to the NHS in England. Nephrol Dial Transplant 2012;27 Suppl 3:iii 73–80. 10.1093/ndt/gfs 269 22815543 PMC 3484716 · doi ↗ · pubmed ↗
- 7UKRR . UK renal Registry 21st annual report - data to 31/12/2017. Bristol; 2019. Available: https://www.renalreg.org/publications-reports/
- 8UKRR . UK renal Registry 24th annual report - data to 31/12/2020. Bristol; 2022. Available: https://ukkidney.org/audit-research/annual-report