MiRNA polymorphisms affect the prognosis of gastric cancer: insights from Xianyou, Fujian
Ping Wu, Yuling Zhang, Yanping Lyu, Jingwen Chen, Yu Jiang, Jianjun Xiang, Baoying Liu, Chuancheng Wu

TL;DR
This study shows that certain miRNA genetic variations are linked to the prognosis of gastric cancer patients in Xianyou, Fujian.
Contribution
The study identifies specific miRNA SNPs as independent predictors of gastric cancer prognosis in a regional population.
Findings
The GG genotype at MSH2 rs17502941 independently increases gastric cancer risk.
Several miRNA SNPs (rs17502941, rs884225, rs1468063, rs7143252, rs2271738) are associated with patient prognosis.
miRNA polymorphisms significantly affect survival time in gastric cancer patients.
Abstract
Gastric cancer, characterized by high incidence and substantial disease burden, has drawn continuous attention regarding its occurrence and prognosis. Genetics plays a crucial role in influencing the prognosis of gastric cancer, and single nucleotide polymorphisms are closely associated with the occurrence, development, and prognosis of this malignant tumor. Our study aims to conduct survival analysis on patients carrying different single nucleotide polymorphisms, exploring the relationship between miRNA single nucleotide polymorphisms and the prognosis of gastric cancer. Genetic data from 344 patients in Xianyou, Fujian, formed the basis of our study. We delineated the survival rate and median survival time, utilizing the log-rank test and COX regression analysis as statistical tools. Upon stratifying the data by sex or operation, it was discerned that the GG genotype at MSH2…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
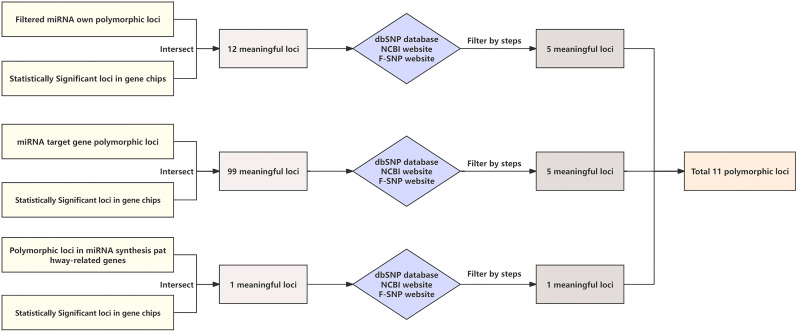 Figure 1
Figure 1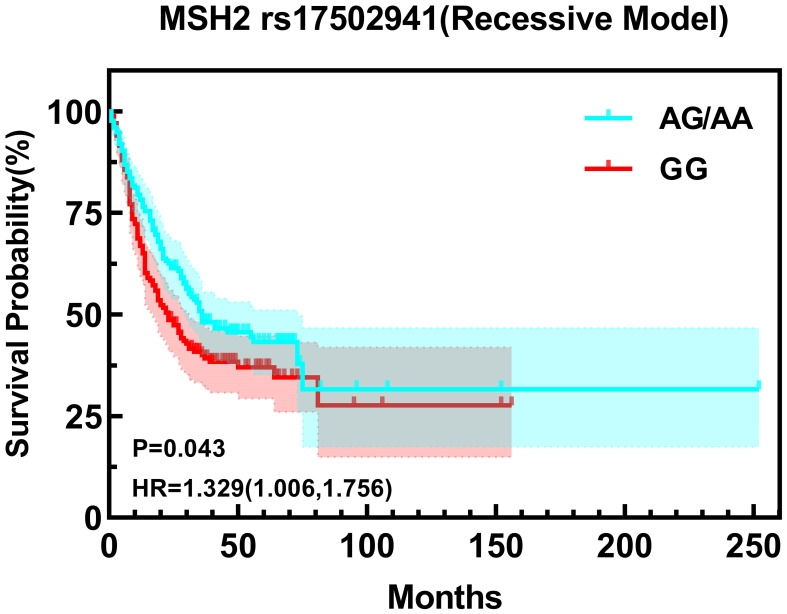 Figure 2
Figure 2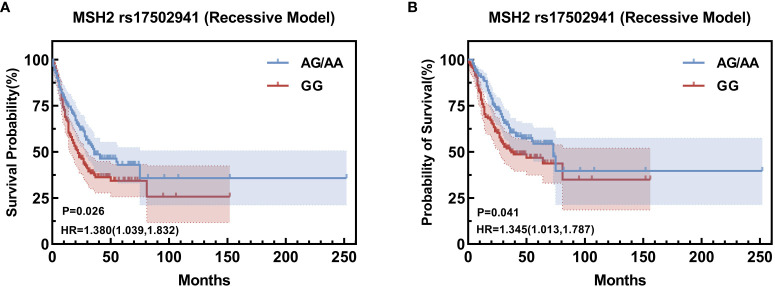 Figure 3
Figure 3| Polymorphisms | Amplification primers | Single-base extension primers |
|---|---|---|
| rs7143252 | F:ACGTTGGATGATTGGGTGAGTCACAGCTTG | ggaatTGTGAGCTAGTCTAGTCTAA |
| rs10413288 | F: ACGTTGGATGTGGTCAAAGAAAATTCCAGG | aaAGCCTGACATCTTCTTGCTC |
| rs9536676 | F: ACGTTGGATGCAGTTATTGTAGTGTTATGC | TCCATTTTTCTATCCTTTGAC |
| rs4713714 | F: ACGTTGGATGGGAAAAAGTGCTGATGGTG | TGGTGCTGCTTCCTCC |
| rs2724377 | F: ACGTTGGATGGAAGTAGGCAAGATCTGCAC | TCAGGACCCACTTCTTATC |
| rs884225 | F:ACGTTGGATGATGAGCGTTAGACTGACTTG | acagTGTTTTGAAACTCAGTATGC |
| rs10277413 | F: ACGTTGGATGTCGCTGCCAGATGATTGTTC | gggaGTCAGAAACCTGCAGGGAC |
| rs1468063 | F: ACGTTGGATGTCTGGATTTAGGAATTGCTC | TTGCTCTTGTCATACCC |
| rs17502941 | F: ACGTTGGATGACAAACCCACACCTTTCAGC | GCAGACACACAGCTC |
| rs11125144 | F: ACGTTGGATGTAGGGAATGGCAGGGTTTGG | GCTACCACTGCTATGAGAC |
| rs2271738 | F: ACGTTGGATGATCTCTTCTTGCCGATCGGG | gagCGGGCGCCGACCTAGCAGT |
| Variables | n | MST (M) | Survival rate (%) | HR (95%CI) | Log-rank P | ||
|---|---|---|---|---|---|---|---|
| 1-year | 3-year | 5-year | |||||
| Sex | |||||||
| Male | 252 | 29.00 | 72.56 | 45.39 | 38.84 | 1 | 0.841 |
| Age | |||||||
| ≦65 | 120 | 55.00 | 84.10 | 58.86 | 47.04 | 1 |
|
| 65- | 224 | 24.00 | 67.79 | 38.75 | 35.65 | 1.580 (1.163, 2.145) | |
| Location | |||||||
| Non-cardia | 179 | 28.00 | 72.07 | 44.68 | 39.76 | 1 | 0.503 |
| Cardia | 165 | 31.00 | 75.00 | 46.84 | 39.71 | 0.91 (0.688, 1.203) | |
| TNM stage | |||||||
| 1 | 51 | – | 94.12 | 81.40 | 78.59 | 1 |
|
| 2 | 166 | 75.00 | 91.57 | 62.45 | 54.34 |
| |
| 3 | 127 | 10.00 | 41.27 | 9.33 | 5.52 |
| |
| Operation | |||||||
| No | 76 | 8.00 | 35.53 | 5.24 | 3.50 | 1 |
|
| Yes | 268 | 64.00 | 84.27 | 57.17 | 49.92 |
| |
| Chemotherapy | |||||||
| No | 140 | 25.00 | 65.00 | 41.21 | 37.24 | 1 | 0.707 |
| Yes | 204 | 33.00 | 79.31 | 48.81 | 41.23 | 0.758 (0.572, 1.003) | |
| Radiotherapy | |||||||
| No | 245 | 31.00 | 72.95 | 46.11 | 42.24 | 1 | 0.592 |
| Yes | 99 | 28.00 | 74.75 | 44.73 | 30.93 | 1.086 (0.800, 1.474) | |
| No. | SNP ID | Gene name | Chromosome | Location | H-W P | MAF |
|---|---|---|---|---|---|---|
| 1 | rs7143252 | miRNA-379 | 14 | 101487621 | 0.331 | 0.211 |
| 2 | rs10413288 | miRNA-519b | 19 | 54197633 | 0.823 | 0.392 |
| 3 | rs9536676 | miRNA-1297 | 13 | 54886472 | 0.122 | 0.227 |
| 4 | rs4713714 | miRNA-7159 | 6 | 33865380 | 0.721 | 0.297 |
| 5 | rs2724377 | miRNA-29c | 1 | 207974818 | 0.373 | 0.170 |
| 6 | rs884225 |
| 7 | 55274048 | 0.931 | 0.187 |
| 7 | rs10277413 |
| 7 | 55238464 | 0.481 | 0.377 |
| 8 | rs1468063 | FAS | 10 | 90775291 | 0.812 | 0.243 |
| 9 | rs17502941 |
| 2 | 47762396 | 0.101 | 0.389 |
| 10 | rs11125144 |
| 2 | 47562636 | 0.830 | 0.159 |
| 11 | rs2271738 |
| 8 | 141566311 | 0.671 | 0.341 |
| rs9536676 | n | MST (M) | Survival rate (%) | HR (95%CI) | Log-rank P | ||
|---|---|---|---|---|---|---|---|
| 1-year | 3-year | 5-year | |||||
| Codominance | |||||||
| GG | 217 | 36.00 | 75.00 | 50.13 | 36.09 | 1 | 0.161 |
| AG | 105 | 20.00 | 67.62 | 40.88 | 32.29 | 1.287 (0.950-1.743) | |
| AA | 22 | 21.00 | 86.36 | 27.27 | 27.27 | 1.398 (0.829-2.359) | |
| Allele gene | |||||||
| G | 539 | 34.00 | 73.56 | 48.32 | 35.35 | 1 |
|
| A | 149 | 21.00 | 73.15 | 36.34 | 29.84 |
| |
| Dominant model | |||||||
| GG | 217 | 36.00 | 75.00 | 50.13 | 36.09 | 1 | 0.060 |
| AG+AA | 127 | 21.00 | 70.87 | 38.15 | 30.78 | 1.308 (0.985-1.736) | |
| Recessive model | |||||||
| GG+AG | 322 | 31.00 | 72.59 | 47.11 | 34.85 | 1 | 0.327 |
| AA | 22 | 21.00 | 86.36 | 27.27 | 27.27 | 1.287 (0.772-2.148) | |
| rs17502941 | n | MST (M) | Survival rate (%) | HR (95%CI) | Log-rank P | ||
|---|---|---|---|---|---|---|---|
| 1-year | 3-year | 5-year | |||||
| Codominance | |||||||
| AA | 31 | 29.00 | 87.10 | 43.83 | 38.96 | 1 | 0.127 |
| AG | 146 | 36.00 | 76.63 | 52.30 | 37.25 | 0.980 (0.579-1.656) | |
| GG | 167 | 23.00 | 68.17 | 40.16 | 30.74 | 1.307 (0.782-2.182) | |
| Allele gene | |||||||
| A | 208 | 36.00 | 79.76 | 50.02 | 37.59 | 1 | 0.077 |
| G | 480 | 27.00 | 70.74 | 43.85 | 32.59 | 1.213 (0.976-1.508) | |
| Dominant model | |||||||
| AA | 31 | 29.00 | 87.10 | 43.83 | 38.96 | 1 | 0.593 |
| AG+GG | 313 | 30.00 | 72.12 | 45.82 | 33.64 | 1.143 (0.695-1.880) | |
| Recessive model | |||||||
| AA+AG | 177 | 36.00 | 78.47 | 50.99 | 37.44 | 1 |
|
| GG | 167 | 23.00 | 68.17 | 40.16 | 30.74 |
| |
| Gene locus | Model | n | MST (M) | HR (95%CI) | Log-rank P | |
|---|---|---|---|---|---|---|
| rs9536676 | Dominant model | GG | 160 | 29.0 | 1 | 0.049* |
| AG+AA | 93 | 19.0 | 1.382 (0.995-1.918) | |||
| rs17502941 | Recessive model | AA+AG | 123 | 30.0 | 1 | 0.034* |
| GG | 130 | 21.5 | 1.415 (1.022-1.960) | |||
| rs11125144 | Codominance | AA | 48 | 34.0 | 1 | 0.027* |
| AG | 36 | 18.5 | 2.118 (1.195-3.755) | |||
| GG | 7 | 34.0 | 1.184 (0.353-3.975) | |||
| Dominant model | AA | 48 | 34.0 | 1 | 0.015* | |
| AG+GG | 43 | 19.0 | 1.962 (1.121-3.432) |
| Gene locus | Model | n | MST (M) | HR (95%CI) | Log-rank P | |
|---|---|---|---|---|---|---|
| rs9536676 | Dominant model | GG | 140 | 27.0 | 1 | 0.044* |
| AG+AA | 84 | 17.0 | 1.380(0.987-1.930) |
| Gene locus | Model | n | MST (M) | HR (95%CI) | Log-rank P | |
|---|---|---|---|---|---|---|
| rs884225 | Codominance | TT | 38 | 25 | 1 | 0.015* |
| CT | 94 | 30.5 | 0.657 (0.405-1.066) | |||
| CC | 47 | 14.0 | 1.216 (0.722-2.046) | |||
| Recessive model | TT+CT | 132 | 27.0 | 1 | 0.017* | |
| CC | 47 | 14.0 | 1.633 (1.082-2.465) | |||
| rs10413288 | Codominance | AA | 23 | 19.0 | 1 | 0.043* |
| AG | 65 | 30.0 | 0.602 (0.338-1.074) | |||
| GG | 77 | 32.0 | 0.492 (0.278-0.870) | |||
| rs9536676 | Dominant model | GG | 116 | 32.0 | 1 | 0.045* |
| AG+AA | 49 | 20.0 | 1.520 (0.988-2.337) | |||
| rs1468063 | Recessive model | CC+CT | 131 | 30.0 | 1 | 0.025* |
| TT | 34 | 18.0 | 1.574 (0.981-2.523) |
| Gene locus | Model | n | MST (M) | HR (95%CI) | Log-rank P | |
|---|---|---|---|---|---|---|
| rs7143252 | Codominance | CC | 11 | 52.0 | 1 | 0.040* |
| CG | 94 | 35.0 | 1.938 (0.601-6.246) | |||
| GG | 112 | 37.5 | 1.123 (0.345-3.660) | |||
| Recessive model | CC+CG | 105 | 35.0 | 1 | 0.028* | |
| GG | 112 | 37.5 | 0.614 (0.395-0.955) |
| Gene locus | Model | n | MST (M) | HR (95%CI) | Log-rank P | |
|---|---|---|---|---|---|---|
| rs11125144 | Dominant model | AA | 32 | 6.5 | 1 | 0.039* |
| AG+GG | 44 | 9.0 | 0.616(0.381-0.998) | |||
| rs17502941 | Recessive model | AA+AG | 138 | 36.0 | 1 | 0.039* |
| GG | 130 | 29.5 | 1.438(1.014-2.039) |
| Gene locus | Model | n | MST (M) | HR (95%CI) | Log-rank P | |
|---|---|---|---|---|---|---|
| rs9536676 | Codominance | GG | 80 | 31.5 | 1 | 0.040* |
| AG | 50 | 16 | 1.444 (0.919-2.269) | |||
| AA | 10 | 18 | 2.233 (1.111-4.491) | |||
| Dominant model | GG | 80 | 31.5 | 1 | 0.033* | |
| AG+AA | 60 | 17.0 | 1.566 (1.026-2.392) | |||
| rs10413288 | Dominant model | AA | 30 | 19.0 | 1 | 0.020* |
| AG+GG | 174 | 30.0 | 0.575 (0.357-0.928) | |||
| rs2271738 | Recessive model | CC+CT | 98 | 24.5 | 1 | 0.014* |
| TT | 106 | 30.0 | 0.631 (0.433-0.918) |
| Variables | β | SE | HR (95%CI) | P |
|---|---|---|---|---|
| TNM stage (1,2 vs 3) | 1.534 | 0.176 | 4.636 (3.284-6.544) | <0.001 |
| Operation (No vs Yes) | -0.870 | 0.182 | 0.419 (0.293-0.599) | <0.001 |
| Radiotherapy (No vs Yes) | 0.397 | 0.163 | 1.488 (1.082-2.046) | 0.014 |
| rs17502941 (GG vs. AA/AG) | 0.332 | 0.145 | 1.380 (1.039-1.832) | 0.026 |
| Variables | β | SE | HR (95%CI) | P |
|---|---|---|---|---|
| TNM stage (1,2 vs 3) | 1.572 | 0.176 | 4.815 (3.411-6.798) | <0.001 |
| Radiotherapy (No vs Yes) | 0.365 | 0.162 | 1.441 (1.050-1.978) | 0.024 |
| rs17502941 (GG vs. AA/AG) | 0.296 | 0.145 | 1.345 (1.013-1.787) | 0.041 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMicroRNA in disease regulation · Cancer-related molecular mechanisms research · Circular RNAs in diseases
Introduction
1
According to cancer incidence and mortality data for the year 2018 from the International Agency for Research on Cancer (IARC), gastric cancer constituted 8.2% of all cancer-related deaths (1). A substantial number of patients receive a diagnosis of advanced-stage cancer, indicative of a low rate of early detection (2). Simultaneously, the prognosis of gastric cancer is intricately linked to various factors, encompassing the degree of differentiation, sex, tumor microenvironment, and the epithelial-mesenchymal transition (EMT) signature associated with metastasis (3–5). Heredity stands out as a significant factor influencing the prognosis of gastric cancer, with single nucleotide polymorphism closely intertwined with the onset, progression, and prognosis of this malignancy. A comprehensive meta-analysis indicates that diminished microRNA expression is detrimental to patient prognosis and may expedite the progression of gastric cancer (6). Discrepancies in miRNA blood levels have been identified in patients with gastric cancer (GC), affirming the utility of miRNA expression as a diagnostic and prognostic biomarker for this condition (7). Moreover, investigations have proposed a close association between miRNA and multidrug resistance (8, 9). There is suggestive evidence that miR-214 can regulate the expression of FGF9, impeding the migration and invasion of gastric cancer (GC) cells. Conversely, miR-519a-3p has been implicated in promoting liver metastasis in gastric cancer and is associated with an unfavorable prognosis (10, 11). Several studies have identified miRNA-21 rs1292037 and miR-149 rs2292832C/T as potential prognostic indicators for hepatocellular carcinoma (12, 13). Additionally, investigations have linked miR-34 rs4938723 and miR-195-5p to the prognosis of colorectal cancer (14, 15). Moreover, research findings indicate that single nucleotide polymorphisms in miRNAs are correlated with the prognosis of various types of tumors (16–19). While numerous studies have established associations between miRNA single nucleotide polymorphisms and the prognosis of various types of tumors, limited attention has been directed toward exploring the connection between miRNA single nucleotide polymorphisms and the prognosis of gastric cancer. Our research complements the existing knowledge body in this specific domain.
Our study aimed to scrutinize the correlation between miRNA polymorphisms and the prognosis of gastric cancer. We meticulously selected 11 miRNA loci and assessed their impact on gastric cancer prognosis using four distinct models: Co-dominance, Allele gene, dominant model, and recessive model. Subsequently, a stratified analysis was conducted based on parameters such as sex, age, location, TNM stage, the performance of surgery, and administration of chemotherapy. Multivariate COX analysis was then applied to sites demonstrating statistical significance in the stratified analysis, thereby delving into the factors exerting independent risk effects on the prognosis of gastric cancer.
Materials and methods
2
Study populations
2.1
This research encompassed the distribution of 555 questionnaires, of which 96 cases posed challenges for investigation due to reasons such as removal, denial of dis-ease, and rejection of examination. (recovery rate: 82.7%) Following a thorough examination of the questionnaires, 115 incomplete and unqualified counts were excluded, and ultimately, 344 questionnaires were finally adopted. Therefore, our study included 344 patients, with peripheral blood samples collected from each patient. The inclusion criteria were as follows: (1) voluntary participation in the study and signing of informed consent by the researchers, (2) patients confirmed by endoscopic biopsy or surgical specimens to have gastric adenocarcinoma, (3) residing in Xianyou for more than 10 years, (4) confirmed between April 2013 and November 2017, with the final follow-up conducted in December 2022. Exclusion criteria were: (1) patients simultaneously diagnosed with other types of tumors besides gastric adenocarcinoma, (2) severe mental illness or poor compliance leading to inability to follow-up, (3) severe genetic diseases, including chromosomal number and structural abnormalities. The histological type of tumors was evaluated according to the standards of the World Health Organization (WHO), and tumor staging was classified according to the guidelines outlined in the American Joint Committee on Cancer Staging Manual (7th edition).
Selection of polymorphism loci
2.2
Previous studies have identified 112 loci associated with gastric cancer, including 12 miRNA polymorphic loci, 99 miRNA target gene polymorphic loci, and 1 miRNA synthesis pathway gene polymorphic locus (Figure 1). To further identify the miRNA-SNPs most closely related to gastric cancer, we selected 11 loci for this study through the following steps:
Initially, utilizing the dbSNP database (http://www.ncbi.nlm.nih.gov/projects/SNP/), we determined the minimum allele frequency (MAF) of each SNP locus in the Chinese population. Loci with MAF between 0.15 and 0.40 were chosen.Subsequently, based on information from the NCBI website (https://pubmed.ncbi.nlm.nih.gov/), we selected loci associated with gastrointestinal (GI) tumors.Finally, using the F-SNP website (http://compbio.cs.queensu.ca/F-SNP/), we screened for loci with corresponding functions.
Flowchart for selecting required loci.
SNP genotyping
2.3
The 11 selected miRNA candidate loci were examined using the Sequenom Mass ARRAY SNP method. The process involved the following steps:
- Designing Primers:
Design PCR amplification primers and single-base extension primers for SNP locus to be tested using Genotyping Tools and Mass ARRAY Assay Design software (Table 1).
- PCR Amplification:
Perform PCR amplification reactions for the selected loci.
- Product Processing:
Process the PCR amplification products.
- Mass ARRAY Dispensing:
Initiate the Mass ARRAY RS1000 dispenser and deposit the processed product onto the SpectroCHIP (Sequenom) chip.
- SpectroCHIP Detection:
Employ Mass ARRAY MALDI-TOP to detect the SpectroCHIP, capturing the type and output of results.
- Result Analysis:
Analyze the results using TYPER4.0 software.
This methodology allows for the precise genotyping of the selected miRNA candidate loci.
Quality control
2.4
Quality of questionnaires
2.4.1
Throughout the on-site investigation, the inspectors meticulously adhered to the questionnaire requirements. Following the survey, the questionnaire data underwent a thorough examination. Any incomplete questionnaires were promptly supplemented with as much information as possible. To ensure data accuracy, a double data entry method was employed, involving logical corrections and consistency testing. Additionally, a random sample of 10% of the entries underwent further review to enhance the overall quality and reliability of the data.
Quality of genotyping
2.4.2
Dish QC (DQC) serves as a pivotal metric for evaluating the quality of genotyping. This assessment relies on comparing the distribution of signal values with background signal values, where a greater difference signifies a more effective experimental process and higher genotyping quality for the respective sample. In this experiment, all DQC results exceeded 0.82, indicating excellent genotyping quality. Genotypes were determined in a blinded manner, and 2% of the samples underwent random selection for repeated testing. The concordance rate in these repeated tests was found to be 98.47%. This robust quality control process ensures the reliability and accuracy of the genotyping results.
Statistical analysis
2.5
Survival rates for different genotypes of the same polymorphic locus in the 1st, 3rd, and 5th years were derived from the mortality table. The Kaplan-Meier method was employed to calculate the survival time of patients with different genotypes, and corresponding survival curves were graphically represented. The log-rank test was then applied to analyze the correlation between single nucleotide polymorphism and the prognosis of gastric cancer. Hazard ratios (HRs) and 95% confidence intervals (CIs) were computed using both univariate and multivariate COX regression modeling methods.
For statistical analysis, the significance level (α) was set at 0.05, and all P values were based on two-sided tests. The statistical software utilized for these analyses was SPSS 24.0, ensuring robust and standardized statistical evaluation of the data.
Ethics approval
2.6
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Fujian Medical University, China (No. 97,2014).
Results
3
Characteristics of study populations
3.1
Among the 344 patients included in the study, there were 252 male patients and 92 female patients, ranging in age from 36 to 96 years, with an average age of (69.15 ± 9.34) years and a median age of 69 years. The survival rates for the 344 gastric cancer patients were recorded at 73.47%, 45.71%, and 39.67% in the 1st, 3rd, and 5th years, respectively, with a median survival time of 30.00 months.
To explore the relationship between the overall condition and prognosis of patients with stomach cancer, the aforementioned statistical methods were employed. It was observed that age, TNM stage, and whether surgery was performed were all correlated with the prognosis of gastric cancer patients (P<0.05) (Table 2).
Relationship between polymorphism and prognosis of gastric cancer
3.2
The study incorporated a total of 11 miRNA polymorphic sites, with detailed information provided in Table 3. The results of the statistical analysis revealed a significant difference in the survival time associated with the A mutant gene of the polymorphic locus miRNA-1297 rs9536676 in comparison to the wild-type gene G. Specifically, the risk of death for patients carrying the A allele was 1.258 times higher than that of patients carrying the G allele (HR=1.258, 95% CI=1.000-1.581, Log-rank P = 0.046). In the case of the polymorphic locus MSH2 rs17502941, survival times exhibited statistical significance in the recessive model (AA+AG/GG). Patients carrying the GG genotype had a 1.329 times higher risk of death compared to those carrying the AA/AG genotype (HR=1.329, 95% CI=1.006-1.756, Log-rank P=0.043) None of the other polymorphic loci were found to be associated with the prognosis of gastric cancer (Tables 4, 5).
Stratified analysis
3.3
In the dominant model, the AG and AA genotypes at miRNA-1297 rs9536676 emerge as risk factors for patients aged over 65 years, male patients, and those diagnosed with cardiac cancer. Similarly, the AG and GG genotypes at miRNA-519b rs10413288 serve as protective factors for patients with cardiac cancer and those who have undergone chemotherapy, as per the dominant model. Notably, the AG and GG genotypes at MSH2 rs11125144 act as risk factors for female patients (co-dominant and dominant models) but as a protective factor for patients who did not undergo surgery (recessive model).
In the stratified analysis, rs17502941, rs884225, rs1468063, rs7143252, and rs2271738 were all identified as significant factors linked to the prognosis of patients (Tables 6–11).
COX multifactor analysis
3.4
Building upon the insights garnered from the Univariate survival analysis, a comprehensive COX multifactor analysis was conducted specifically for MSH2 rs17502941 (Figures 2, 3). Stratifying the analysis by sex or operation, it was found that the GG genotype at MSH2 rs17502941 (recessive model) serves as an independent risk factor for the prognosis of gastric cancer (Tables 12, 13).
Kaplan-Meier Curve for rs17502941 based on univariate analysis.
Kaplan-Meier Curve for rs17502941 based on comprehensive COX multifactor analysi, stratified by male (A), stratified by operation (B).
Discussion
4
Our study uncovered a robust association between the single nucleotide poly-morphism of MSH2 rs17502941 and the prognosis of gastric cancer. Employing COX stratification analysis, we identified that the GG locus of rs17502941 was indicative of a poor prognosis in male patients and those who underwent surgery in a recessive model. Numerous studies have consistently highlighted the intricate relationship between diverse miRNAs and the prognosis of gastric cancer. Elevated expression levels of miR-203, miR-218, and miR-194 have been correlated with a favorable prognosis for gastric cancer, while diminished expression of miR-17-5p and miR-34a serves as a marker for an unfavorable prognosis (6, 20, 21). Furthermore, a diminished expression of PARP-1, a DNA damage response (DDR)-associated protein, has been identified as a prognostic indicator for patients with stage 2 and 3 gastric cancer (22). Given its role as a DDR-associated gene, the low expression of MSH2 may similarly contribute to an unfavorable prognosis. Numerous investigations have proposed associations between MSH2 and various cancers, including prostate, colorectal, and ovarian cancers (23, 24), in addition to its linkage with the risk of gastric cancer (25, 26). Additionally, a separate study identified a correlation between the TC+CC genotype of MSH2 rs2303428 and a diminished survival rate in non-cardia cancers (27). In our investigation, we observed that the GG genotype of MSH2 rs2303428 stood out as an independent risk factor for an unfavorable prognosis among male, surgical patients, aligning with previous findings. However, in multifactorial analyses, we did not discern their significant effects on the prognosis of gastric cancer.
Earlier studies had implicated these miRNAs in the prognosis of gastric cancer. A research endeavor from Hubei, China, underscored that the diminished expression of miRNA-379 served as an independent risk factor for patients’ prognosis (28). Likewise, a study conducted in Xi’an, China, revealed that miRNA-1297 exhibited low expression in gastric cancer tissues, and this reduced expression independently correlated with compromised disease-free survival for patients (29). However, our investigation sorely yielded statistically significant associations between miRNA-379 rs7143252, miRNA-1297 rs9536676, and gastric cancer prognosis. This discrepancy may be indicative of regional variations in gastric cancer genotyping, and the presence of a complex interplay of confounding factors and genes cannot be discounted. Further research is imperative, as there remains a possibility that multiple loci identified in the univariate analysis are indeed linked to the prognosis of gastric cancer.
Research endeavors have identified risk factors affecting the prognosis of gastric cancer as well as specific loci that could be associated with its prognosis. These findings offer crucial insights, laying the groundwork for further exploration. Some miRNAs related to gastric cancer risk and prognosis have already been collected and arranged by academics, including miR-499, miR-146a, and so on (30), it’s noteworthy that the loci unveiled in our study are not among them. This discrepancy suggests, on the one hand, the significance of our research, and on the other hand, underscores the vast untapped potential within this field. Global epidemiological studies on gastric cancer have unveiled intriguing patterns, emphasizing the distinct genetic landscape in Asian populations. Notably, Asians exhibit a heightened frequency of IL-10 and IL-17 gene diversity. This diversity, in con-junction with environmental factors and lifestyle habits, collectively influences the risk and prognosis of gastric cancer (31). Moreover, specific regional variations have been observed, such as the unique characteristics of gastric cancer in the Tibetan Plateau compared to other regions. This dissimilarity encompasses differences in incidence rates, mutation types, and molecular variations among patients from the highlands and Western countries, as well as Han Chinese and ethnic minorities, have different molecular variations in their mutated gene, For instance, an analysis revealed a notable discrepancy in notch2 mutations, with only one out of 12 Han Chinese exhibiting this mutation compared to seven out of 18 ethnic minorities (32). These findings underscore the imperative need for region-specific sequencing efforts, particularly in areas marked by elevated gastric cancer rates.
Gaining insight into diverse mutation types and single nucleotide polymorphisms across different regions not only establishes a theoretical framework but also lays the molecular foundation for the development of miRNA therapy in gastric cancer. This breakthrough holds the promise of tailoring treatments according to the distinct mutation profiles of patients in various regions. Furthermore, it paves the way for the creation of genetic databases encompassing patients from diverse geographical areas. These databases will serve as valuable reservoirs of background information, facilitating future investigations into the underlying molecular mechanisms. We anticipate that on-going and advanced research endeavors will propel miRNA therapy for gastric cancer from theory to reality. This therapeutic approach, already under exploration in diverse fields such as non-alcoholic liver disease, diabetes mellitus, myocardial fibrosis, and resensitization of chemotherapy-resistant cancer cells, holds immense potential (33). However, it is essential to acknowledge the limitations of our current study. Primarily, the outcomes may not be universally applicable, as our sample pool is derived from Xianyou, Fujian. Additionally, future studies necessitate larger sample sizes to ensure a more precise exploration of influencing factors.
Persisting as the primary contributor to cancer-related mortality on a global scale, gastric cancer maintains a dynamic temporal trend. It continues to be characterized by high incidence, elevated morbidity, and a substantial disease burden (34). Our research serves as a foundational reference for future investigations into molecular mechanisms, contributing to a comprehensive understanding of the involvement of single nucleotide polymorphisms (SNPs) in the pathogenesis of gastric cancer.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: The data are not publicly available due to privacy. Requests to access these datasets should be directed to [email protected].
Ethics statement
The studies involving humans were approved by the Ethics Committee of Fujian Medical University, China. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
PW: Writing – original draft. YZ: Validation, Writing – review & editing. YL: Visualization, Methodology, Writing – review & editing. JC: Formal analysis, Conceptualization, Writing – review & editing. YJ: Writing – review & editing, Data curation. JX: Writing – review & editing. BL: Writing – review & editing, Project administration. CW: Writing – review & editing, Supervision, Resources.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ferlay J Colombet M Soerjomataram I Mathers C Parkin DM Pineros M. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J OF Cancer. (2019) 144:1941–53. doi: 10.1002/ijc.31937 30350310 · doi ↗ · pubmed ↗
- 2Tan Z. Recent advances in the surgical treatment of advanced gastric cancer: A review. Med Sci MONITOR. (2019) 25:3537–41. doi: 10.12659/MSM.916475 PMC 652854431080234 · doi ↗ · pubmed ↗
- 3Zeng D Li M Zhou R Zhang J Sun H Shi M. Tumor microenvironment characterization in gastric cancer identifies prognostic and immunotherapeutically relevant gene signatures. Cancer Immunol Res. (2019) 7:737–50. doi: 10.1158/2326-6066.CIR-18-0436 30842092 · doi ↗ · pubmed ↗
- 4Song J Wei R Huo S Gao J Liu X. Metastasis related epithelial-mesenchymal transition signature predicts prognosis and response to immunotherapy in gastric cancer. Front Immunol. (2022) 13:920512. doi: 10.3389/fimmu.2022.920512 35769483 PMC 9234207 · doi ↗ · pubmed ↗
- 5Sexton RE Hallak MNA Uddin H Diab M Azmi AS. Gastric cancer heterogeneity and clinical outcomes. Technol IN Cancer Res Treat. (2020) 19:1079203125. doi: 10.1177/1533033820935477 PMC 743298732799763 · doi ↗ · pubmed ↗
- 6Li Z Liu Z-M Xu B-H. A meta-analysis of the effect of micro RNA-34a on the progression and prognosis of gastric cancer. Eur Rev Med Pharmacol Sci. (2018) 22:8281–7. doi: 10.26355/eurrev_201812_16525 30556868 · doi ↗ · pubmed ↗
- 7Link A Kupcinskas J. Micro RN As as non-invasive diagnostic biomarkers for gastric cancer: Current insights and future perspectives. World J OF Gastroenterol. (2018) 24:3313–29. doi: 10.3748/wjg.v 24.i 30.3313 PMC 609258330122873 · doi ↗ · pubmed ↗
- 8Wei L Sun J Zhang N Zheng Y Wang X Lv L. Noncoding RN As in gastric cancer: implications for drug resistance. Mol Cancer. (2020) 19:62. doi: 10.1186/s 12943-020-01185-7 32192494 PMC 7081551 · doi ↗ · pubmed ↗