Clinical approach and utilizing liquid biopsies to interrogate suspected acquired resistance to PD-1 blockade
Dilanka Lakshan De Silva, Jia Luo

TL;DR
The paper discusses how to clinically manage suspected resistance to PD-1 immunotherapy using liquid biopsies for better understanding and treatment decisions.
Contribution
The paper introduces a multi-modal clinical guide for evaluating suspected acquired resistance to PD-1 blockade using liquid biopsies.
Findings
Liquid biopsies offer real-time insights into treatment response and resistance mechanisms.
Discrepancies between imaging, clinical status, and sequencing data should be carefully investigated.
A systematic approach is needed to interrogate suspected resistance rather than assuming it.
Abstract
PD-1 blockade is now routine for nearly all patients with non-small lung cancer. Acquired resistance to PD-1 blockade – defined generally as an initial response followed later by progression [1-3] is a common yet poorly understood concept. A key clinical challenge to insight has been a lack of standard guidance for clinical management of a case of suspected acquired resistance. The infrequency of performing tumor biopsies and the uncertainty of actionability from tissue sampling likely also contribute to limited insight into the biology of acquired resistance [4]. To address this knowledge gap and to highlight the value of tumor and liquid biopsy, we present a representative case of suspected acquired resistance to PD-1 blockade and propose a multi-modal guide for approaching this clinical scenario. Acquired resistance to immunotherapy should not be assumed but should be thoroughly…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
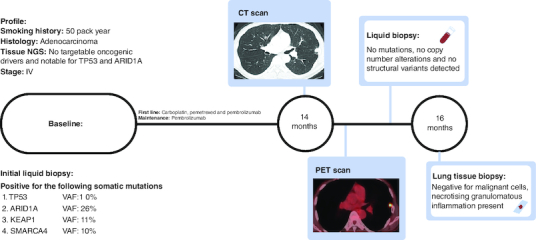 Figure 1
Figure 1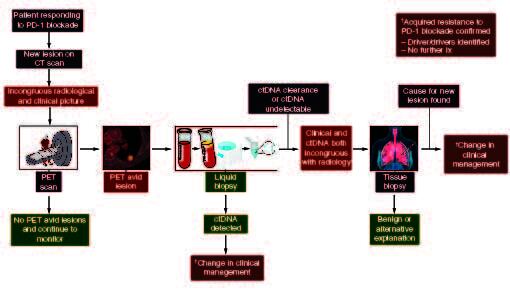 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Immunotherapy and Biomarkers · Immunotherapy and Immune Responses · Chronic Lymphocytic Leukemia Research
PD-1 blockade is now routine for nearly all patients with non-small lung cancer. However, the proper investigation of alternative explanations and the cause remains not intuitive for many clinicians. We present a case of a patient who benefitted from PD-1 blockade for more than a year, but later developed what was initially suspected to be radiological progression. A systematic approach to investigating with the utilization of clinical examination, radiology and comprehensive molecular profiling with tissue and liquid biopsy of the new pulmonary nodule revealed an alternate explanation, preventing the premature discontinuation of treatment and providing a framework for approaching this clinical scenario. In presenting this individual case, we aim to highlight the approach, considerations, and tools that can be used to address new radiologic changes suspected, but not certain, to be acquired resistance to PD-1 blockade.
Case presentation
A current smoker with a 50-pack-year smoking history presented to care with bilateral lung nodules and a suspicious left adrenal gland lesion. A diagnostic biopsy showed metastatic lung adenocarcinoma; scant tissue limited PD-L1 expression. Tissue underwent comprehensive molecular testing with MSK-IMPACT (Integrated Mutation Profile of Actionable Cancer Targets), the in-house FDA approved platform that can detect many mutations even at very low allele frequencies (<2%) [5]. As a companion diagnostic, he was offered MSK-ACCESS (Analysis of Circulating cfDNA to Evaluate Somatic Status), an in-house liquid biopsy platform. MSK-ACCESS can detect over 120 mutations even at a variable allele frequency of 0.5% with more than 99% sensitivity when paired with tissue sequencing, as with our patient [6]. MSK IMPACT tissue platform demonstrated no targetable mutations, but was notable for TP53 and ARID1A mutations. MSK-ACCESS liquid biopsy platform was congruous with the initial tissue biopsy, but additional mutations were discovered and were notable for detectable alterations in TP53, ARID1A, KEAP1, MAP2K and SMARCA4 (Figure 1). The patient initially received carboplatin, pemetrexed, and pembrolizumab and immediately achieved an excellent clinical and a complete radiological response. After four cycles of combination therapy, both carboplatin and pemetrexed were ceased and pembrolizumab was continued as maintenance therapy every 3 weeks. The deep response persisted for more than 14 months while on pembrolizumab alone, most consistent with an ongoing response to PD-1 blockade therapy.
Timeline of the patient.At baseline, no targetable mutations, but liquid biopsy detected TP53, ARID1A, KEAP1 and SMARCA4 mutations. After complete response, at 14 months, a solitary pulmonary nodule was detected on CT, and it was PET avid indicative of potentially acquired resistance to PD-1 therapy. Liquid biopsy detected clearance and was inconsistent with radiology. Further investigation with tissue biopsy at 16 months revealed a benign diagnosis and refuted the progression of the disease.
More recently, a routine interval CT scan showed a new 1.2 cm subpleural nodule in the lingula. The prior primary and metastatic lesions remained well controlled without progression. The patient clinically felt well. To inform the persistence and avidity of the new nodule, and to assess for additional suspicious sites of distant metastasis, we evaluated his disease status with a PET scan. This test redemonstrated the PET avid new nodule with an SUVmax of 6.2 and was suspicious for recurrent malignancy but identified no other distant sites of metastasis. We also surveyed for radiologically occult systemic recurrence using ctDNA testing, which returned no detectable somatic variants, with the clearance of previously detected somatic alterations. Given the radiologic suspicion of acquired resistance to PD-1 blockade, but the patient feeling clinically well and with no detectable ctDNA shedding in the blood, we next pursued a biopsy of the nodule to determine the diagnosis. Fortunately, pathology revealed no malignant cells and rather a necrotizing, granulomatous inflammation. No further intervention was pursued on the nodule, and the patient has remained well on pembrolizumab with no further evidence of progression.
Discussion
This case represents a common clinical scenario clinicians face in patients with non-small cell lung cancer and response to PD-1 blockade. Acquired resistance can occur in nearly 2/3rds of initial responders and, akin to this case, commonly occurs in a single site or oligo-pattern of progression [7]. Most clinicians in this context would acknowledge progression, especially after PET avidity, and explore other options such as local therapy or change of systemic treatment. Our approach to this scenario is multimodal and includes a comprehensive diagnostic evaluation rather than empirically pursuing a change in systemic therapy or palliative radiation (Figure 2). This multimodality approach utilizes comprehensive molecular profiling through tissue or liquid biopsies, traditional radiology, functional imaging and the patient's clinical status. The systematic approach helps prevent unnecessary complications associated with invasive investigations such as a tissue biopsy in a cohort of people already at high risk of complications such as pneumothorax [8,9]. This stepwise approach will guide a clinician through systemic interrogation to determine the cause for the acquired resistance and efficient deployment of resources yielding the maximum benefit to the patient and the healthcare setting.
Schema for investigation of acquired resistance to PD-1 blockade.After CT diagnosis of the pulmonary nodule, proceed with functional imaging with a PET scan. If PET avid, proceed to liquid biopsy to confirm progression, identify therapeutic targets, and for consideration of management change. If the liquid biopsy confirms clearance, i.e., ongoing response, proceed to tissue biopsy to characterize the pulmonary nodule.
Specifically, faced with a new nodule concerning acquired resistance to PD-1 blockade, we evaluated the patient's clinical status with an exam and history, informing the persistence relative suspicion of the nodule with a subsequent PET scan. Then we assessed the systemic status of detectable cancer with ctDNA testing to confirm the resistance and potentially identify new drivers and therapeutic options, including clinical trials if a driver was identified.
In our patient, the clinical and the complete ctDNA clearance [10] indicated ongoing response, which was incongruous with the radiology and necessitated proceeding to the final step in the scheme: a diagnostic biopsy. It is important to note that if the ctDNA was congruent with the clinical picture, it confirmed oligoprogression and could provide invaluable information regarding the underlying driver of progression and allude to targets and therapeutic options. In addition, it makes the next step, as suggested in Figure 2, proceeding to an invasive biopsy redundant. Fortunately, a benign diagnosis was discovered, and no further intervention was required preventing premature discontinuation of treatment or unnecessary radiation. This case serves as a reminder that acquired resistance should not be assumed but instead approached thoughtfully and carefully examined prior to pursuing interventions that may not be necessary or prematurely stopping the current line of therapy. Additionally, this case highlights the value of pursuing a more comprehensive molecular characterization, either from a traditional tissue biopsy or liquid biopsy, in the context of suspected acquired resistance to PD-1 blockade. This may facilitate the discovery of the molecular underpinnings of resistance and inform the development of rational therapeutic strategies in the future.
Conclusion
A new lesion in a patient otherwise responding well to PD-1 blockade should not be presumed to be acquired resistance and should instead be investigated in a stepwise manner.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brahmer JR, Govindan R, Anders RA et al. The Society for Immunotherapy of Cancer consensus statement on immunotherapy for the treatment of non-small cell lung cancer (NSCLC). J. Immunother. Cancer 6(1), 75 (2018).30012210 10.1186/s 40425-018-0382-2PMC 6048854 · doi ↗ · pubmed ↗
- 2Sharma P, Hu-Lieskovan S, Wargo JA, Ribas A. Primary, Adaptive, and Acquired Resistance to Cancer Immunotherapy. Cell 168(4), 707–723 (2017).28187290 10.1016/j.cell.2017.01.017PMC 5391692 · doi ↗ · pubmed ↗
- 3Kluger HM, Tawbi HA, Ascierto ML et al. Defining tumor resistance to PD-1 pathway blockade: recommendations from the first meeting of the SITC Immunotherapy Resistance Taskforce. J. Immunother. Cancer 8(1), 398 (2020).10.1136/jitc-2019-000398 PMC 717406332238470 · doi ↗ · pubmed ↗
- 4Schoenfeld AJ, Hellmann MD. Acquired Resistance to Immune Checkpoint Inhibitors. Cancer Cell 37(4), 443–455 (2020).32289269 10.1016/j.ccell.2020.03.017PMC 7182070 · doi ↗ · pubmed ↗
- 5Cheng DT, Mitchell TN, Zehir A et al. Memorial Sloan Kettering-Integrated Mutation Profiling of Actionable Cancer Targets (MSK-IMPACT): A Hybridization Capture-Based Next-Generation Sequencing Clinical Assay for Solid Tumor Molecular Oncology. J. Mol. Diagn. 17(3), 251–264 (2015).25801821 10.1016/j.jmoldx.2014.12.006PMC 5808190 · doi ↗ · pubmed ↗
- 6Rose Brannon A, Jayakumaran G, Diosdado M et al. Enhanced specificity of clinical high-sensitivity tumor mutation profiling in cell-free DNA via paired normal sequencing using MSK-ACCESS. Nat. Commun. 12(1), 3770 (2021).34145282 10.1038/s 41467-021-24109-5PMC 8213710 · doi ↗ · pubmed ↗
- 7Shah S, Wood K, Labadie B et al. Clinical and molecular features of innate and acquired resistance to anti-PD-1/PD-L 1 therapy in lung cancer. Oncotarget 9(4), 4375–4384 (2018).29435109 10.18632/oncotarget.23315 PMC 5796980 · doi ↗ · pubmed ↗
- 8Huo YR, Chan MV, Habib AR, Lui I, Ridley L. Pneumothorax rates in CT-Guided lung biopsies: a comprehensive systematic review and meta-analysis of risk factors. Br. J. Radiol. 93(1108), 20190866 (2020).31860329 10.1259/bjr.20190866 PMC 7362905 · doi ↗ · pubmed ↗