Endoscopic transpapillary gallbladder drainage using a novel drill dilator
Jun Noda, Yuichi Takano, Masataka Yamawaki, Tetsushi Azami, Fumitaka Niiya, Fumiya Nishimoto, Masatsugu Nagahama

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
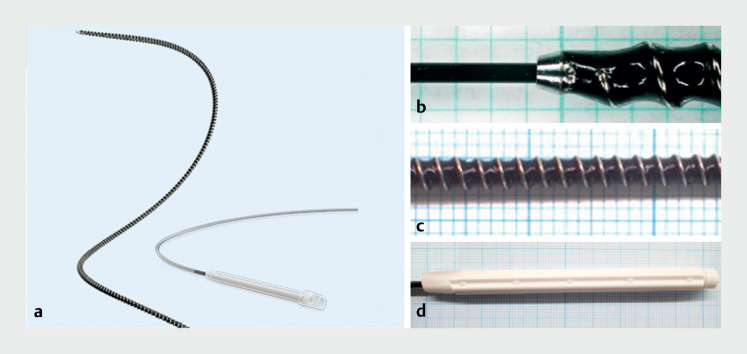 Fig. 1
Fig. 1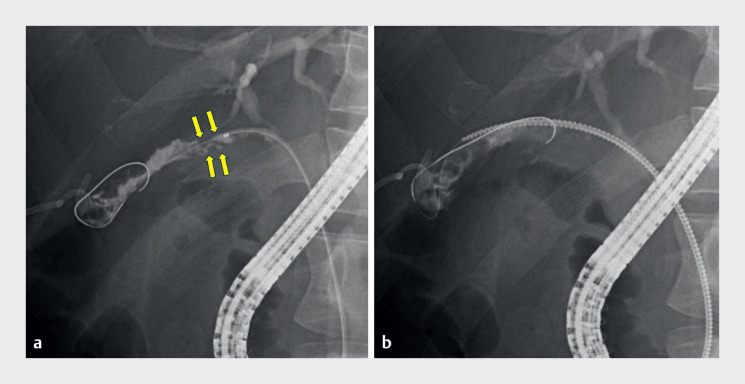 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Esophageal and GI Pathology · Pediatric Hepatobiliary Diseases and Treatments
In endoscopic transpapillary gallbladder drainage (ETGBD), device insertion through the cystic duct to the gallbladder is challenging 1 . Even if a guidewire can be placed in the gallbladder, the device cannot be inserted due to stone or inflammation of the cystic duct in some cases 2 3 . We experienced a case in which ETGBD was successfully performed using a novel drill-type dilator ( Fig. 1 ).
Details of the novel drill-type dilator. a The Tornus ES (Olympus Medical Systems, Tokyo, Japan) is a novel spiral drill dilator designed with an outer diameter of 7 Fr. b The dilator tip is tapered to match the outer diameter of the guidewire. c The shaft is coiled to ensure flexibility. d The handle is easy to rotate. Source for Fig. 1 a : Olympus Corporation.
A 49-year-old man was brought to the emergency department due to acute cholecystitis and cholangitis, and percutaneous transhepatic gallbladder drainage (PTGBD) was performed. Endoscopic ultrasound revealed a 3-mm stone in the common bile duct. Endoscopic retrograde cholangiopancreatography was performed, and endoscopic stone extraction was performed after endoscopic sphincterotomy. We attempted placement of an endoscopic gallbladder stent (EGBS) until elective cholecystectomy. Although the cystic duct was breached with a guidewire (Visiglide2; Olympus Medical Systems, Tokyo, Japan), the catheter (PR-V614M; Olympus) could not be inserted to the gallbladder due to a stone in the cystic duct ( Fig. 2 a ). The novel drill-type dilator was inserted, rotated clockwise, and successfully passed through the cystic duct ( Fig. 2 b ). After dilation, a catheter could be inserted into the gallbladder. We switched to a 0.035-inch hard-type guidewire (Revowave Hard; Piolax, Kanagawa, Japan) and a 5 Fr × 32 cm EGBS (IYO-stent; Gadelius, Tokyo, Japan) was successfully placed ( Video 1 ). There were no adverse events associated with the procedure. PTGBD was removed and the patient was scheduled for cholecystectomy.
Fluoroscopic images. a The catheter could not be inserted to the gallbladder due to a stone (arrows) in the cystic duct. b The novel drill-type dilator was carefully inserted and successfully passed through the cystic duct.
We successfully placed a gallbladder stent using the novel drill dilator to breach the cystic duct stricture.Video 1
In cases where device insertion into the gallbladder is difficult, this novel drill-type dilator can be an effective option.
Endoscopy_UCTN_Code_TTT_1AR_2AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mohan B Khan S Adler D Endoscopic ultrasound-guided gallbladder drainage, transpapillary drainage, or percutaneous drainage in high risk acute cholecystitis patients: a systematic review and comparative meta-analysis Endoscopy 2020529610610.1055/a-1020-393231645067 · doi ↗ · pubmed ↗
- 2Maruta A Iwata K Shimizu M Factors affecting technical success of endoscopic transpapillary gallbladder drainage for acute cholecystitis J Hepatobiliary Pancreat Sci 20202742943610.1002/jhbp.74432352636 · doi ↗ · pubmed ↗
- 3Yoshida M Naitoh I Kataoka H Theoretical step approach with ‘Three-pillar’ device assistance for successful endoscopic transpapillary gallbladder drainage P Lo S One 202318 e 028160536758010 10.1371/journal.pone.0281605 PMC 9910654 · doi ↗ · pubmed ↗